Minimally Invasive SERI Hallux Valgus Correction: An Intraoperative Masterclass
Key Takeaway
Master the Minimally Invasive SERI technique for hallux valgus correction. This intraoperative guide covers comprehensive anatomy, meticulous preoperative planning, and granular, real-time surgical execution. Learn precise instrument handling, critical decision-making, and advanced strategies for managing complications. Gain insights into postoperative rehabilitation for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of hallux valgus has undergone a profound paradigm shift over the past two decades, pivoting from extensive open procedures to increasingly sophisticated minimally invasive techniques. Among these, the SERI technique—an acronym for Simple, Effective, Rapid, and Inexpensive—stands out as a highly elegant, reproducible, and biomechanically sound approach for correcting mild to moderate hallux valgus deformities. Pioneered and popularized by Sandro Giannini, this technique represents a masterclass in leveraging percutaneous osteotomies and minimal internal fixation to achieve powerful triplanar correction while respecting the delicate soft tissue envelope of the forefoot. This chapter serves as an exhaustive, definitive guide to mastering the SERI technique, providing the orthopedic surgeon with the nuanced intraoperative knowledge required to execute this procedure flawlessly.
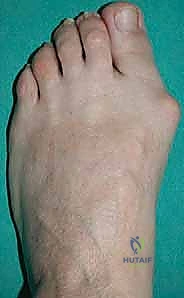
Before embarking on surgical intervention, one must possess a profound understanding of the patho-epidemiology of hallux valgus. Hallux valgus is not merely an exostosis or a simple "bunion"; it is a complex, progressive, multi-planar deformity of the first ray. It is characterized by the lateral deviation and pronation of the proximal phalanx of the great toe, coupled with the medial deviation and pronation of the first metatarsal. This skeletal malalignment initiates a devastating cascade of biomechanical failures. As the metatarsal head drifts medially, it slips off the sesamoid apparatus. The sesamoids, tethered by the transverse metatarsal ligament and adductor hallucis, remain in their anatomical position relative to the second metatarsal, effectively becoming laterally subluxated relative to the first metatarsal head.
Epidemiologically, hallux valgus is overwhelmingly prevalent in adult females, with a strong hereditary predisposition often linked to generalized ligamentous laxity. The pathogenesis is multifactorial, involving an interplay of intrinsic anatomical variants (such as a rounded metatarsal head, hypermobility of the first tarsometatarsal joint, or a long first metatarsal) and extrinsic factors like constricting, high-heeled footwear. As the deformity progresses, the intrinsic musculature—specifically the abductor hallucis—migrates plantarly, transforming from an abductor into a plantarflexor and pronator, thereby exacerbating the deformity. The extensor hallucis longus (EHL) and flexor hallucis longus (FHL) bowstring laterally across the metatarsophalangeal (MTP) joint, creating a relentless deforming vector. Understanding this dynamic soft-tissue imbalance is critical, as the SERI technique relies on the strategic translation of the metatarsal head to effectively "auto-reduce" these deforming forces without the need for a formal, open lateral soft-tissue release.
Detailed Surgical Anatomy and Biomechanics
Mastery of the SERI technique requires an intimate, three-dimensional spatial awareness of the first ray's surgical anatomy, particularly the neurovascular structures that are placed at risk during minimally invasive approaches. The first metatarsal is the primary weight-bearing axis of the medial forefoot. Its distal articular surface is highly congruent with the base of the proximal phalanx, and its plantar surface features two distinct longitudinal grooves separated by the crista, which articulate with the medial (tibial) and lateral (fibular) sesamoids.

Vascular Supply and the Extracapsular Ring
The vascularity of the first metatarsal head is robust but highly susceptible to iatrogenic injury during osteotomy and capsular stripping. The primary blood supply is derived from the first dorsal metatarsal artery and the first plantar metatarsal artery. These vessels contribute to a rich, extracapsular arterial ring that encircles the anatomical neck of the metatarsal. Branches from this ring penetrate the bone at the metaphyseal-diaphyseal junction. The SERI technique's reliance on a strictly medial, minimal incision with limited subperiosteal dissection is specifically designed to preserve this vascular network. By avoiding extensive lateral capsular stripping—a common step in traditional open chevron or scarf osteotomies—the risk of avascular necrosis (AVN) of the metatarsal head is dramatically reduced, even when significant lateral translation is achieved.

Neuroanatomy and Musculotendinous Vectors
Neurologically, the surgeon must be acutely aware of the medial dorsal cutaneous nerve, a branch of the superficial peroneal nerve. This nerve courses superficially over the dorsomedial aspect of the first MTP joint and is highly vulnerable during the initial percutaneous incision and subsequent retractor placement. Plantarly, the proper plantar digital nerve supplies sensation to the medial hallux. Careful, blunt dissection down to the joint capsule is imperative to sweep these nerves safely out of the operative field.
Biomechanically, the first MTP joint is stabilized by a complex hammock of ligaments and tendons. Medially, the abductor hallucis inserts into the medial sesamoid and the base of the proximal phalanx; laterally, the adductor hallucis (transverse and oblique heads) inserts into the lateral sesamoid and proximal phalanx. In a hallux valgus deformity, the medial collateral ligament becomes attenuated, while the lateral structures contract. The brilliance of the SERI osteotomy lies in its biomechanical consequence: by performing an extra-articular transverse or slightly oblique osteotomy and translating the metatarsal head laterally, the surgeon effectively shortens the path of the lateral structures, relaxing the adductor hallucis and lateral capsule. Simultaneously, this lateral translation repositions the metatarsal head squarely over the sesamoid complex, restoring the physiological windlass mechanism without requiring direct surgical manipulation of the sesamoids themselves.

Exhaustive Indications and Contraindications
Patient selection is the cornerstone of success in minimally invasive forefoot surgery. The SERI technique is not a panacea for all hallux valgus deformities; it is a highly specific tool optimized for a distinct subset of pathologies. The ideal candidate is a patient with a symptomatic, mild to moderate hallux valgus deformity where the primary pathology is localized to the first MTP joint, without profound instability at the first tarsometatarsal (TMT) joint.
| Category | Specific Parameters / Conditions |
|---|---|
| Primary Indications | Symptomatic Hallux Valgus unresponsive to conservative care. |
| Mild to Moderate Deformity: Hallux Valgus Angle (HVA) 15° to 35°. | |
| Intermetatarsal Angle (IMA) 10° to 15°. | |
| Congruent or subluxated joint that is manually reducible. | |
| Pain localized to the medial eminence (bunion pain). | |
| Relative Contraindications | Severe Deformity: HVA > 40° or IMA > 20° (High risk of undercorrection). |
| Osteoporosis or poor bone stock (Risk of K-wire cut-out or loss of fixation). | |
| Mild first TMT joint hypermobility (May require concomitant stabilization). | |
| Previous failed hallux valgus surgery (Revision cases often require open approaches). | |
| Absolute Contraindications | Severe first TMT joint hypermobility or clinical instability (Requires Lapidus arthrodesis). |
| Advanced Hallux Rigidus / severe degenerative joint disease of the 1st MTP joint. | |
| Active local or systemic infection. | |
| Severe peripheral vascular disease or profound neuropathy (e.g., Charcot arthropathy). | |
| Spasticity or severe neuromuscular disorders leading to uncontrollable deforming forces. |
When assessing a patient, clinical examination must evaluate the reducibility of the deformity and the presence of hypermobility at the first TMT joint. If grasping the first metatarsal head and translating it laterally fully corrects the hallux valgus without significant resistance, the patient is an excellent candidate for SERI. Conversely, if the deformity is rigid, or if there is profound sagittal plane instability at the TMT joint (evidenced by dorsal elevation of the first ray during the hypermobility test), an isolated distal metatarsal osteotomy will likely fail, and a proximal fusion (Lapidus procedure) should be considered.
Pre-Operative Planning, Templating, and Patient Positioning
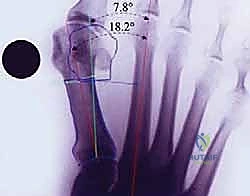
Meticulous preoperative planning is non-negotiable. Standardized, weight-bearing anteroposterior (AP) and lateral radiographs of the foot are mandatory. The surgeon must systematically analyze these images to dictate the precise geometry of the intraoperative osteotomy.
Radiographic Parameter Analysis
Key parameters include the Hallux Valgus Angle (HVA), the Intermetatarsal Angle (IMA), and the Distal Metatarsal Articular Angle (DMAA). The DMAA is particularly critical; if the articular cartilage is laterally deviated (high DMAA), the osteotomy must be tailored to not only translate the head laterally but also to rotate it medially to restore joint congruency. Furthermore, the metatarsal formula (relative lengths of the first and second metatarsals) must be assessed. If the first metatarsal is excessively long, the osteotomy cut can be angled from distal-dorsal to proximal-plantar to purposefully shorten the ray, thereby decompressing the joint and reducing the risk of postoperative stiffness. Conversely, if the first metatarsal is short, the cut must be strictly perpendicular to the shaft axis to prevent further shortening, which could precipitate devastating transfer metatarsalgia to the lesser rays.
Anesthesia and Patient Setup
Regional anesthesia is strongly preferred. A popliteal sciatic nerve block, combined with a saphenous nerve block, provides profound intraoperative anesthesia and excellent postoperative analgesia, facilitating immediate weight-bearing—a key component of the SERI protocol. The patient is positioned supine on a radiolucent operating table. A bump may be placed under the ipsilateral hip to internally rotate the leg, allowing the foot to rest in a neutral position, though many surgeons prefer to externally rotate the leg to bring the medial border of the foot directly facing the ceiling.
A pneumatic thigh or calf tourniquet is applied to ensure a bloodless field, which is vital for visualizing the small percutaneous incision and preventing thermal necrosis during the osteotomy by allowing irrigation fluid to cool the burr or saw blade effectively. The C-arm fluoroscopy unit is draped sterilely and brought in either from the contralateral side or over the top, positioned to provide effortless, immediate AP and lateral views without requiring the surgeon to reposition the foot awkwardly.
Step-by-Step Surgical Approach and Fixation Technique
The execution of the SERI technique demands surgical finesse, strict adherence to anatomical planes, and constant fluoroscopic vigilance.
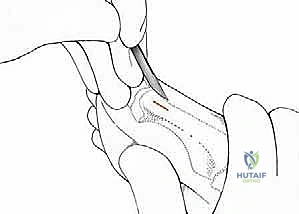
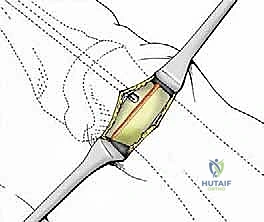
1. The Percutaneous Incision and Soft Tissue Handling
The procedure begins with a precise 1-cm to 1.5-cm longitudinal incision placed strictly on the medial midline of the first metatarsal, centered over the anatomical neck, just proximal to the medial eminence.

Using a #15 blade, the incision is carried sharply through the epidermis and dermis. From this point, blunt dissection is mandatory. Using a small hemostat or tenotomy scissors, the subcutaneous tissues are gently spread. This maneuver pushes the terminal branches of the medial dorsal cutaneous nerve superiorly and the plantar neural structures inferiorly. The periosteum over the medial metatarsal neck is incised longitudinally.
Two small, specially designed blunt retractors (or miniature Hohmann retractors) are inserted subperiosteally—one sweeping dorsally and one plantarly. This creates a safe working corridor, protecting the extensor and flexor tendons, as well as the neurovascular bundles, from the oscillating saw or burr.
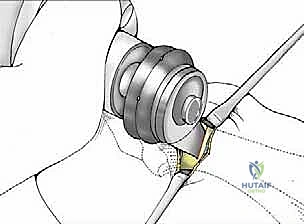
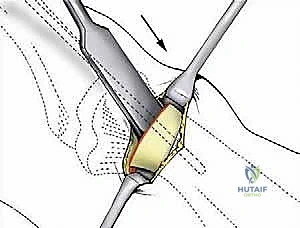
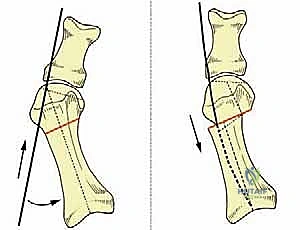
2. The Osteotomy Execution
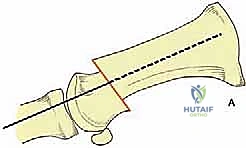
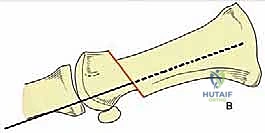
The critical step is the osteotomy. While Giannini originally described using a low-speed Shannon burr, many modern surgeons utilize a micro-sagittal saw for a cleaner, flatter cut that provides superior bone-to-bone contact during translation. The osteotomy is performed at the subcapital level (the anatomical neck).
Under direct vision and fluoroscopic guidance, the saw blade is introduced. The orientation of this cut dictates the final three-dimensional position of the metatarsal head. For a standard correction without shortening, the cut is made strictly perpendicular to the longitudinal axis of the first metatarsal shaft in both the sagittal and transverse planes.
Copious cold saline irrigation is directed into the wound during cutting to prevent thermal necrosis of the bone, which is a leading cause of delayed union or AVN in minimally invasive surgery. The cut must be complete; any remaining plantar-lateral cortical hinge will tether the head and prevent adequate lateral translation.
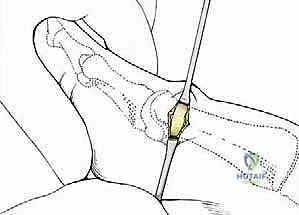
3. Translation, Reduction, and K-Wire Fixation
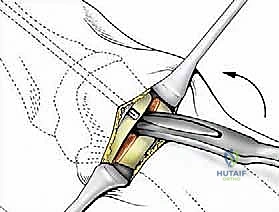
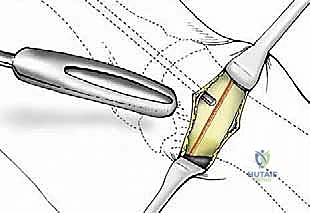
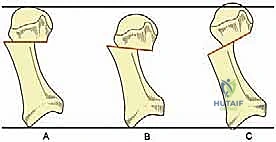
Once the osteotomy is complete, the retractors are removed. The surgeon grasps the great toe and applies manual traction, slight plantarflexion, and varus stress. Simultaneously, thumb pressure is applied to the medial aspect of the metatarsal head, pushing it laterally. The metatarsal head should translate laterally by 50% to 80% of the shaft width, depending on the severity of the IMA.
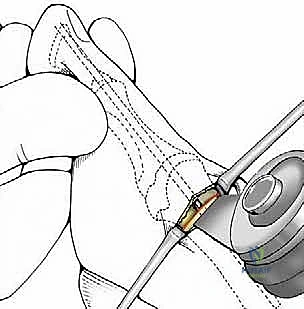
This lateral shift is the essence of the SERI technique. It reduces the IMA, realigns the metatarsal head over the sesamoids, and dynamically relaxes the lateral soft tissues.
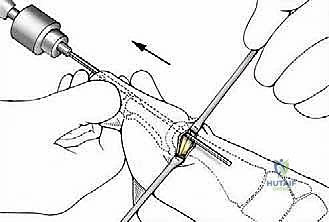
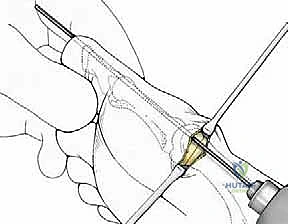
Fixation is achieved using a single, stout 2.0 mm Kirschner wire (K-wire). The K-wire is introduced percutaneously at the tip of the great toe, just plantar and medial to the eponychium to avoid nail bed injury. It is driven axially through the distal phalanx, the interphalangeal joint, the proximal phalanx, and across the MTP joint into the translated metatarsal head.
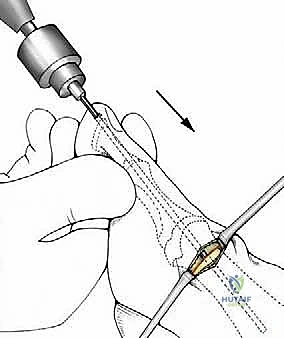
The critical maneuver occurs as the K-wire exits the proximal aspect of the metatarsal head. The surgeon must lever the K-wire (and thus the toe and metatarsal head) to ensure perfect alignment. The K-wire is then driven into the medullary canal of the first metatarsal shaft, effectively locking the laterally translated head against the medial cortex of the shaft.
4. Final Fluoroscopic Verification and Closure
Extensive fluoroscopic imaging is now performed. AP views confirm the reduction of the HVA and IMA, the lateral translation of the head, and the restoration of the sesamoid position. Lateral views are paramount to ensure there is no dorsal elevation of the metatarsal head, which would inevitably lead to transfer metatarsalgia. The K-wire must be confirmed to be intramedullary within the proximal metatarsal shaft.



Once alignment is deemed perfect, the K-wire is bent and cut outside the skin at the tip of the toe to allow for easy removal in the clinic. The small medial incision is closed with one or two non-absorbable sutures. No medial eminence resection (bunionectomy) is typically required, as the medial prominence is functionally eliminated by the lateral translation of the head.
Complications, Incidence Rates, and Salvage Management
While the SERI technique is elegant, it is not without risks. The learning curve is steep, and complications often stem from technical errors during the osteotomy or K-wire placement.


| Complication | Estimated Incidence | Etiology / Technical Error | Salvage / Management Strategy |
|---|---|---|---|
| Pin Tract Infection | 5% - 10% | Prolonged K-wire retention, poor patient hygiene, friction in footwear. | Oral antibiotics (e.g., Cephalexin). Early pin removal if union is sufficient. Rarely requires IV antibiotics. |
| Transfer Metatarsalgia | 3% - 8% | Unintentional dorsal elevation of the 1st metatarsal head during K-wire fixation; excessive shortening of the 1st ray. | Conservative: Custom orthotics with metatarsal pads. Surgical: Weil osteotomies of the affected lesser metatarsals. |
| Loss of Correction / Recurrence | 4% - 7% | Premature K-wire removal, patient non-compliance with taping, unrecognized 1st TMT hypermobility. | Revision surgery, often requiring an open approach or a Lapidus arthrodesis to stabilize the medial column. |
| Avascular Necrosis (AVN) | < 1% | Excessive lateral soft tissue stripping, thermal necrosis from the saw/burr without adequate irrigation. | Protected weight-bearing. If severe collapse occurs, progression to 1st MTP joint arthrodesis is required. |
| Delayed Union / Nonunion | 1% - 3% | Thermal necrosis, inadequate bone-to-bone contact after translation, excessive motion at the osteotomy site. | Prolonged immobilization, bone stimulators. If symptomatic nonunion persists, revision with rigid internal fixation and bone grafting. |
| Hallux Varus | 1% - 2% | Over-translation of the metatarsal head laterally, over-tightening of the medial capsule. | Conservative: Taping into valgus. Surgical: Soft tissue release, reverse osteotomy, or MTP joint fusion in severe cases. |

A meticulous surgical technique is the best prevention. Ensuring the K-wire is perfectly intramedullary prevents dorsal tilt. Copious irrigation prevents thermal damage, mitigating the risk of AVN and nonunion.
Phased Post-Operative Rehabilitation Protocols
The postoperative protocol is as critical as the surgical execution in the SERI technique. Because the fixation relies solely on a single K-wire and soft tissue tension, strict adherence to rehabilitation guidelines is required to maintain the correction while bone healing occurs.
Phase 1: Immediate Post-Op to Week 4
Immediately following surgery, a specialized, rigid postoperative dressing is applied. The toe is taped securely into a slightly overcorrected varus and plantarflexed position. This taping is paramount; it acts as an external splint, counteracting the deforming forces of the EHL and adductor hallucis. The patient is placed in a stiff-soled, flat postoperative shoe. Remarkably, full weight-bearing on the heel and lateral border of the foot is permitted and encouraged immediately, as axial loading compresses the osteotomy site, promoting primary bone healing. The patient is instructed to perform daily pin-site care with alcohol or betadine drops.
Phase 2: Week 4 to Week 6
At approximately 4 weeks postoperatively, clinical and radiographic evaluation is performed. Radiographs should demonstrate early callus formation at the osteotomy site. At this juncture, the transarticular K-wire is easily removed in the outpatient clinic without the need for local anesthesia. Once the pin is removed, the patient is instructed to begin gentle, active, and passive range of motion (ROM) exercises of the first MTP joint to prevent capsular contracture and stiffness. The toe must continue to be taped in the corrected position for an additional 2 to 4 weeks to allow the soft tissues to heal in their new, lengthened or shortened states.
Phase 3: Week 6 and Beyond
By week 6, patients typically transition out of the stiff postoperative shoe into a wide-toebox, supportive athletic shoe. High-impact activities and tight-fitting footwear are strictly prohibited until at least 12 weeks postoperatively, when radiographic consolidation of the osteotomy is complete. Physical therapy may be utilized to optimize gait mechanics, maximize MTP joint dorsiflexion, and strengthen the intrinsic foot musculature.
Summary of Landmark Literature and Clinical Guidelines
The SERI technique is heavily supported by robust clinical literature, demonstrating outcomes comparable to, and in some metrics superior to, traditional open osteotomies. Giannini's original prospective studies established the foundation, reporting significant improvements in AOFAS (American Orthopaedic Foot and Ankle Society) scores and reliable radiographic correction with a remarkably low complication rate.
Subsequent independent meta-analyses have validated these findings. When compared to the open Scarf or Chevron osteotomies, the SERI technique consistently demonstrates shorter operative times, reduced postoperative pain scores in the first two weeks, and smaller scar formations, leading to higher patient satisfaction regarding cosmesis. However, the literature also emphasizes the steep learning curve associated with minimally invasive foot surgery. Misjudging the osteotomy plane or failing to secure intramedullary K-wire purchase are well-documented pitfalls that lead to malunion and transfer metatarsalgia.
Current clinical guidelines from major orthopedic foot and ankle societies recognize percutaneous extra-articular osteotomies (like SERI) as highly effective interventions for mild to moderate hallux valgus. They stress, however, that these techniques should be reserved for surgeons who have undergone specialized training in percutaneous methods and possess a thorough understanding of three-dimensional forefoot fluoroscopic anatomy. When executed correctly, the SERI technique is a powerful, elegant procedure that restores the complex
