Masterclass in the Scarf Osteotomy: Biomechanics, Technique, and Outcomes

Key Takeaway
The Scarf osteotomy is a highly versatile, horizontally directed displacement Z-osteotomy performed at the first metatarsal diaphysis. Renowned for its exceptional sagittal plane stability and broad healing surface, it effectively corrects mild-to-moderate hallux valgus deformities. This guide details the precise surgical technique, biomechanical principles, and critical strategies to prevent complications such as troughing, ensuring optimal outcomes for orthopedic surgeons and their patients.
Comprehensive Introduction and Patho-Epidemiology
The Scarf osteotomy represents one of the most powerful and versatile diaphyseal procedures available to the modern foot and ankle surgeon for the correction of hallux valgus. Originally conceptualized in the mid-20th century and later popularized and refined by pioneers such as Weil and Barouk in the 1990s, the procedure derives its name from a classic carpentry technique. In architectural terminology, a "scarf" joint is created by notching, grooving, or cutting the ends of two distinct pieces of wood and fastening them together so that they overlap, thereby forming one continuous, structurally sound, and mechanically robust piece. When translated to orthopedic surgery, this configuration yields an extraordinarily high level of intrinsic stability—particularly in the sagittal plane—and provides a remarkably broad surface area of exposed cancellous bone, which is highly conducive to rapid primary bone healing.
Hallux valgus is not merely a static two-dimensional deformity but a complex, multi-planar pathoanatomical cascade that involves transverse plane divergence (increased intermetatarsal angle), sagittal plane instability (elevation of the first ray), and coronal plane rotation (pronation of the metatarsal and hallux). The patho-epidemiology of this condition dictates that as the first metatarsal drifts medially, the sesamoid apparatus remains anatomically tethered to the second metatarsal via the deep transverse metatarsal ligament. Consequently, the metatarsal head subluxates medially off the sesamoid complex, leading to a functional failure of the windlass mechanism and a transfer of weight-bearing forces to the lesser metatarsals. The Scarf osteotomy is uniquely designed to address these complex multi-planar deformities by allowing for precise, multi-directional translation of the capital fragment while maintaining rigid internal fixation.

Biomechanical cadaveric studies have definitively confirmed that under physiological loaded conditions, the Scarf osteotomy possesses double the stability of a distal chevron or a proximal crescentic osteotomy. Beyond its robust stability, the enduring popularity of the Scarf osteotomy among foot and ankle specialists lies in its unparalleled versatility. By meticulously altering the orientation of the diaphyseal and transverse osteotomy cuts, the surgeon can achieve lateral displacement of the plantar bone fragment to reduce the intermetatarsal angle (IMA), medial displacement of the capital fragment to correct iatrogenic hallux varus, plantar displacement to increase the load-bearing capacity of the first ray, or elongation/shortening of the first metatarsal to restore the harmonious cascade of the forefoot. Because of this profound intrinsic stability, patients are often permitted early weight-bearing, facilitating a faster return to baseline activities and minimizing the risk of disuse osteopenia and joint stiffness.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy of the first ray is an absolute prerequisite for the safe and effective execution of the Scarf osteotomy. The vascular supply to the first metatarsal is the most critical anatomical consideration, as iatrogenic disruption can lead to the catastrophic complication of avascular necrosis (AVN) of the metatarsal head. The primary blood supply to the first metatarsal head is derived from the first dorsal metatarsal artery, the first plantar metatarsal artery, and the superficial branch of the medial plantar artery. These vessels form an intricate extraosseous anastomotic ring at the anatomical neck of the metatarsal. The intraosseous blood supply is primarily delivered via the nutrient artery, which enters the lateral aspect of the diaphyseal shaft. Because the Scarf osteotomy involves an extensive diaphyseal cut that inherently disrupts the intraosseous medullary blood supply, the viability of the capital fragment becomes entirely dependent on the intact extraosseous capsular and periosteal vascular networks.
To preserve this delicate vascularity, the surgeon must adhere to strict anatomical boundaries during dissection. The plantar periosteum and the lateral soft tissue attachments to the metatarsal head must be meticulously preserved. Stripping the plantar capsule or aggressively dissecting the lateral aspect of the metatarsal neck will devascularize the plantar-distal fragment, drastically increasing the risk of osteonecrosis. Furthermore, the medial approach utilized in the Scarf osteotomy must carefully protect the dorsal medial cutaneous nerve and the proper plantar digital nerve, which run in close proximity to the standard surgical incision. Retraction of these neurovascular bundles must be gentle, utilizing blunt retractors to avoid neuropraxia or the formation of painful postoperative neuromas.

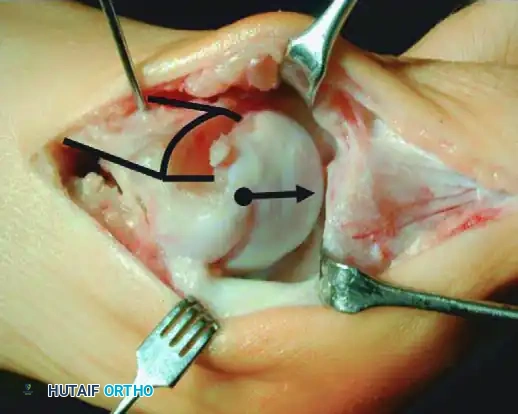
From a biomechanical perspective, the Scarf osteotomy is governed by strict geometric principles. The procedure relies on a precise Z-cut, consisting of a long longitudinal diaphyseal cut and two short transverse cuts (one distal-dorsal, one proximal-plantar). The spatial orientation of these cuts dictates the three-dimensional movement of the capital fragment. Standard lateral translation is achieved when the short osteotomy cuts are perfectly perpendicular to the longitudinal axis of the second metatarsal. If shortening of the first ray is desired—often necessary in severe deformities to decompress the metatarsophalangeal joint—the transverse cuts are oriented obliquely from medial-distal to lateral-proximal. Conversely, orienting the transverse cuts from medial-proximal to distal-lateral allows for distal translation and lengthening. Furthermore, by angulating the longitudinal cut from dorsal-medial to plantar-lateral, the surgeon can induce plantarflexion of the metatarsal head during lateral translation, thereby restoring the weight-bearing function of the medial column and addressing concomitant transfer metatarsalgia.

Exhaustive Indications and Contraindications
Current indications for the Scarf osteotomy encompass a broad spectrum of mild, moderate, and selectively severe hallux valgus deformities. It is generally considered the procedure of choice for patients presenting with an Intermetatarsal Angle (IMA) between 11 and 18 degrees and a Hallux Valgus Angle (HVA) between 20 and 40 degrees. However, the true limiting factor for the Scarf osteotomy is not solely the angular severity of the deformity, but rather the anatomical width of the first metatarsal diaphysis. Because the procedure relies on the overlapping of the dorsal and plantar bone fragments, the absolute limit of lateral correction is dictated by the available bone stock. The wider the metatarsal, the greater the potential for lateral translation. To maintain structural integrity and provide adequate surface area for primary bone healing, the minimal overlapping between the two fragments must be at least one-third of the metatarsal width.
While highly experienced surgeons may occasionally push this limit to a one-fourth overlap in exceptional cases, doing so significantly increases the risk of mechanical failure, troughing, and non-union. Therefore, patients with an exceptionally narrow first metatarsal ("pipestem" metatarsal) are poor candidates for a Scarf osteotomy, even if their angular deformity falls within the accepted parameters. In such cases, a proximal crescentic osteotomy or a Lapidus procedure (first tarsometatarsal arthrodesis) is biomechanically superior. Additionally, the Scarf osteotomy is highly effective for correcting an abnormal Distal Metatarsal Articular Angle (DMAA). By rotating the capital fragment internally during lateral translation, the surgeon can effectively dial in the articular congruity of the MTP joint, a critical step in preventing postoperative recurrence of the deformity.

Contraindications to the Scarf osteotomy must be rigorously respected to avoid catastrophic postoperative failures. Absolute contraindications include first ray instability or hypermobility localized to the first tarsometatarsal (Lisfranc) joint. If a hypermobile TMT joint is present, a diaphyseal osteotomy will fail to address the apex of the deformity, leading to inevitable recurrence; these patients require a Lapidus arthrodesis. Furthermore, degenerative joint disease (osteoarthritis) of the first metatarsophalangeal joint precludes any joint-sparing procedure; a first MTP arthrodesis is the gold standard in this scenario. Severe osteoporosis or osteopenia is another major contraindication, as poor bone stock drastically increases the risk of hardware pull-out and the dreaded "troughing" complication, where the hard cortical bone of one fragment sinks into the soft cancellous bone of the other.
| Parameter | Indications for Scarf Osteotomy | Contraindications |
|---|---|---|
| Intermetatarsal Angle (IMA) | 11° to 18° (Moderate to Severe) | > 20° (Relative contraindication, consider Lapidus) |
| Hallux Valgus Angle (HVA) | 20° to 40° | > 50° with severe soft tissue contracture |
| Metatarsal Width | Wide diaphysis allowing > 1/3 overlap | Narrow "pipestem" metatarsal (< 1/3 overlap possible) |
| First TMT Joint Stability | Stable TMT joint | Hypermobility / Ligamentous laxity at TMT joint |
| MTP Joint Status | Congruent or subluxated, no arthritis | Hallux rigidus / Advanced Osteoarthritis |
| Bone Quality | Normal bone mineral density | Severe Osteoporosis / Rheumatoid Arthritis |
| Patient Age/Status | Skeletally mature adults | Open physes (Pediatric patients) |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful Scarf osteotomy. The clinical evaluation must include a comprehensive assessment of the patient's gait, hindfoot alignment, and Achilles tendon flexibility. A tight Achilles tendon or gastrocnemius complex will exert a profound plantarflexory force on the forefoot, exacerbating the hallux valgus deformity and increasing the risk of postoperative recurrence or transfer metatarsalgia. If a severe equinus contracture is identified, a concomitant gastrocnemius recession or Achilles lengthening should be considered. The surgeon must also carefully evaluate the stability of the first tarsometatarsal joint in the sagittal plane. The modified Klaue test can be utilized to assess hypermobility; excessive dorsal excursion of the first ray relative to the lesser metatarsals indicates TMT instability, which may necessitate a shift in the surgical plan toward a Lapidus procedure.

Radiographic templating requires standardized weight-bearing anteroposterior (AP), lateral, and sesamoid axial views of the foot. On the AP radiograph, the surgeon must meticulously measure the Hallux Valgus Angle (HVA), the Intermetatarsal Angle (IMA), and the Distal Metatarsal Articular Angle (DMAA). The width of the first metatarsal diaphysis is measured at the planned osteotomy site to ensure that a minimum of one-third overlap can be achieved after the required lateral translation. The lateral radiograph is scrutinized to assess the sagittal elevation of the first metatarsal and to rule out any midfoot arthritis or flatfoot deformity that could compromise the outcome. The sesamoid axial view is critical for evaluating the degree of lateral sesamoid subluxation and checking for any degenerative changes within the metatarsosesamoid articulation.

Patient positioning in the operating room is standardized but requires attention to detail. The patient is placed in the supine position on the operating table. A small bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral position and allowing the surgeon direct, unimpeded access to the medial aspect of the first ray. A well-padded pneumatic tourniquet is applied to the thigh or calf, depending on surgeon preference and the planned duration of the procedure. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation. The fluoroscopy unit (C-arm) is positioned on the opposite side of the table, allowing for seamless intraoperative imaging without disrupting the sterile field. Proper lighting and the availability of specialized mini-fragment fixation sets and oscillating microsaws are confirmed before the initial incision is made.

Step-by-Step Surgical Approach and Fixation Technique
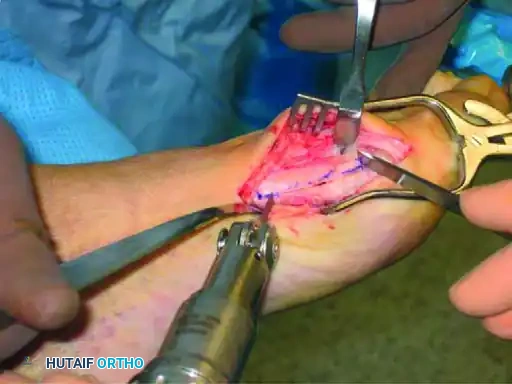
The Scarf osteotomy is technically demanding and carries a steep learning curve. Meticulous attention to detail during the osseous cuts is required to prevent catastrophic complications. The procedure begins with a medial longitudinal skin incision centered over the first MTP joint, extending from the proximal half of the proximal phalanx to the middle third of the first metatarsal diaphysis. The incision is deepened through the subcutaneous tissue, taking care to identify and retract the dorsal medial cutaneous nerve. A medial capsulotomy is performed—typically a longitudinal, L-shaped, or inverted L-shaped incision—to expose the medial eminence and the articular surface of the metatarsal head. A subperiosteal dissection is then carried out to free the dorsal aspects of the proximal phalanx and the first metatarsal. It is an absolute imperative to preserve the critical intraosseous and extraosseous blood supply to the distal capital fragment; therefore, the surgeon must not strip or detach the soft tissues on the plantar aspect of the first metatarsal.

Prior to the osteotomy, a lateral soft tissue release is often performed, either transarticularly through the MTP joint or via a separate dorsal incision in the first web space. This release typically includes a tenotomy of the adductor hallucis, release of the deep transverse metatarsal ligament, and fenestration of the lateral capsule to allow the sesamoid apparatus to reduce beneath the metatarsal head. Once the lateral release is complete, the medial eminence is conservatively resected using an oscillating saw, parallel to the medial border of the foot. The surgeon then proceeds with the three-cut Z-shaped osteotomy. The longitudinal cut begins at the level of the metatarsal head, approximately 5 mm proximal to the articular cartilage, positioned at the junction between the dorsal one-third and the plantar two-thirds of the metatarsal shaft, and extends proximally into the diaphysis. In the frontal plane, this cut should be parallel to the weight-bearing surface, or slightly oblique (dorsomedial to plantar-lateral) if plantarflexion of the metatarsal head is desired.

The execution of the short transverse cuts is the most critical step in avoiding an intraoperative fracture. The distal transverse cut is made dorsally, perpendicular to the long axis of the second metatarsal to maintain metatarsal length. The proximal transverse cut is made plantar at the proximal end of the longitudinal cut. A strict surgical warning must be observed: the two short transverse arms of the Z-cut must be strictly parallel to one another. If these cuts converge, they will create a locking effect, making lateral displacement of the capital fragment impossible without fracturing the bone. Once the cuts are completed, specialized osteotomes or a lamina spreader are used to gently mobilize the fragments. The plantar-distal portion is translated laterally to close the intermetatarsal gap. If the proximal-lateral corner of the head fragment impinges on the second metatarsal (preventing full correction), this corner is carefully resected.
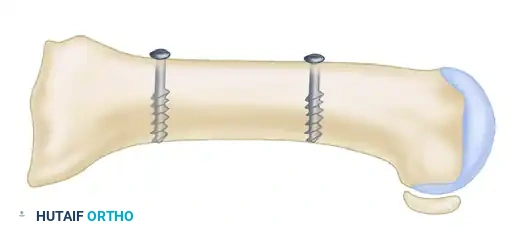
Following satisfactory translation and rotation (to correct the DMAA), the osteotomy is temporarily stabilized with a Kirschner wire inserted from the proximal fragment distally into the distal fragment. Using a K-wire instead of a reduction clamp prevents crushing the delicate plantar soft tissues, thereby preserving vascularity. An intraoperative simulated weight-bearing loading test is performed to assess the MTP joint congruity and sesamoid reduction. Definitive fixation is then achieved using two minifragment screws (typically 2.0 mm, 2.7 mm, or 3.0 mm headless compression screws), utilizing standard lag technique to achieve rigid interfragmentary compression. The overhanging medial cortical shelf of the proximal fragment is resected flush with the translated capital fragment. The medial joint capsule is meticulously repaired. If residual hallux valgus remains despite congruent joint reduction, a closing-wedge proximal phalangeal (Akin) osteotomy is performed before final closure.


Complications, Incidence Rates, and Salvage Management
While reported patient satisfaction rates for the Scarf osteotomy consistently hover around 90%, the procedure is technically unforgiving and carries a distinct profile of potential complications. Minor complications include delayed wound healing, superficial infection, and transient neuropraxia of the dorsal medial cutaneous nerve. More significant complications include delayed union, rotational malunion, proximal stress fractures (often originating from the proximal transverse cut if a stress riser is created), osteonecrosis (AVN) of the first metatarsal head, prominent hardware requiring removal, and complex regional pain syndrome (CRPS). The incidence of AVN is historically reported between 1% and 3%, largely mitigated by modern techniques that strictly preserve the plantar and lateral soft tissue attachments to the metatarsal head.

However, the most frequently reported and biomechanically significant complication unique to the Scarf osteotomy is the "troughing" phenomenon. Occurring in up to one-third of patients in early historical series (though significantly less common with modern modifications), troughing happens when the hard cortical bone of the diaphyseal fragment wedges, or sinks, into the softer, less dense cancellous bone of the opposing metatarsal shaft. This subsidence leads to a catastrophic loss of metatarsal height, resulting in a functional malunion characterized by elevation (dorsiflexion) of the first ray. Clinically, this manifests as a pronated first metatarsal, loss of medial column weight-bearing, and severe, recalcitrant transfer metatarsalgia to the lesser metatarsals. Prevention of troughing requires meticulous patient selection (avoiding osteoporotic patients), ensuring adequate bone overlap (minimum one-third), and utilizing rigid bi-cortical screw fixation.
Salvage management of a failed Scarf osteotomy depends entirely on the nature of the failure. In cases of severe troughing with resultant elevation and transfer metatarsalgia, a corrective plantarflexing opening-wedge osteotomy of the medial cuneiform or the base of the first metatarsal, supplemented with structural bone graft, is often required to restore the sagittal alignment of the medial column. If AVN of the metatarsal head occurs leading to secondary osteoarthritis and joint collapse, joint-sparing procedures are no longer viable. The definitive salvage in this scenario is a first MTP joint arthrodesis, which may require structural interpositional allograft if significant bone loss or shortening has occurred. In cases of recurrent hallux valgus secondary to unrecognized TMT hypermobility, a revision to a Lapidus arthrodesis is the gold standard.
| Complication | Estimated Incidence | Mechanism / Risk Factor | Salvage / Management Strategy |
|---|---|---|---|
| Troughing | 5% - 15% | Cortical bone wedging into cancellous bone; Osteoporosis | Plantarflexing corrective osteotomy with bone graft |
| Avascular Necrosis (AVN) | 1% - 3% | Stripping of plantar/lateral soft tissues; Aggressive lateral release | 1st MTP Arthrodesis (often requiring structural graft) |
| Proximal Stress Fracture | 2% - 5% | Stress riser at the proximal transverse cut | Non-weight bearing cast; ORIF if displaced |
| Recurrence of Deformity | 5% - 10% | Unrecognized TMT hypermobility; Inadequate lateral translation | Lapidus Arthrodesis |
| Hardware Irritation | 10% - 20% | Prominent screw heads beneath medial skin | Elective hardware removal after clinical union |
| Transfer Metatarsalgia | 5% - 12% | Excessive shortening or elevation of 1st ray | Orthotics; Lesser metatarsal Weil osteotomies |

Phased Post-Operative Rehabilitation Protocols
The robust intrinsic stability of the Scarf osteotomy allows for a more accelerated rehabilitation protocol compared to proximal osteotomies or arthrodesis procedures, though careful adherence to phased progression is vital to prevent hardware failure and ensure optimal functional outcomes. Phase 1 (Weeks 0-2) focuses on strict wound healing and edema control. The patient is placed in a bulky, compressive soft dressing and fitted with a rigid, flat-bottom postoperative shoe or a heel-wedge shoe. Weight-bearing is typically restricted to heel-touch or strict non-weight-bearing with crutches, depending on bone quality and the surgeon's intraoperative assessment of fixation stability. Strict elevation of the operative extremity above the level of the heart is mandated to mitigate swelling, which is the primary driver of postoperative pain and wound dehiscence.

Phase 2 (Weeks 2-6) marks the transition to protected weight-bearing and the initiation of early range of motion. At the two-week mark, sutures are removed, and clinical and radiographic assessments are performed to ensure maintenance of alignment. The patient is permitted to transition to flat-foot weight-bearing in a stiff-soled postoperative shoe. Crucially, active and passive range of motion exercises of the first MTP joint are initiated during this phase. The patient is instructed to perform manual plantarflexion and dorsiflexion of the hallux to prevent capsular adhesions and joint stiffness, which are common sequelae of the extensive soft tissue dissection required for the procedure. Night splints or toe spacers may be utilized to maintain the corrected alignment of the hallux.

Phase 3 (Weeks 6-12) involves the transition to normal footwear and the restoration of normal gait mechanics. At six weeks, weight-bearing radiographs are obtained to confirm radiographic union, evidenced by bridging trabeculae across the osteotomy site. Once union is confirmed, the patient is transitioned into a wide-toe-box, supportive athletic shoe. Physical therapy is intensified, focusing on intrinsic foot muscle strengthening, restoration of the windlass mechanism, and proprioceptive training. Phase 4 (Beyond 12 weeks) represents the return to high-impact activities and sports. Patients are counseled that while clinical union occurs by 6-8 weeks, maximal medical improvement and complete resolution of residual edema may take up to 6-12 months.

Summary of Landmark Literature and Clinical Guidelines
The evolution and validation of the Scarf osteotomy are deeply rooted in several landmark orthopedic studies that have shaped modern clinical guidelines. The seminal work by L.S. Barouk in the 1990s was instrumental in popularizing the procedure across Europe and subsequently the United States. Barouk's expansive case series demonstrated the unparalleled versatility of the Scarf osteotomy in addressing severe deformities, highlighting the ability to simultaneously correct the IMA, DMAA, and sagittal elevation. His meticulous description of the surgical technique, particularly the emphasis on preserving the plantar blood supply and the precise angulation of the Z-cuts, remains the foundational text for modern foot and ankle fellows.

Conversely, the critical review published by Coetzee in The Journal of Bone and Joint Surgery served as a necessary cautionary tale, bringing the complication of "troughing" into the mainstream
Clinical & Radiographic Imaging Archive