Revision Hallux Valgus Correction

Comprehensive Introduction and Patho-Epidemiology
Recurrent hallux valgus represents one of the most formidable challenges in modern foot and ankle reconstructive surgery, defined clinically and radiographically as a partial or complete return of valgus deformity at the first metatarsophalangeal (MTP) joint following an index surgical correction. The true incidence of recurrence varies widely in the orthopedic literature, largely depending on the initial procedure selected, the severity of the primary deformity, and the length of postoperative follow-up. However, it is universally acknowledged that when recurrence occurs, it is rarely merely a cosmetic failure; rather, it signifies a profound biomechanical collapse of the first ray. This collapse often leads to debilitating pain, altered gait mechanics, and progressive degeneration of the adjacent forefoot structures. Addressing this complex pathology requires a meticulous understanding of both the primary etiology and the specific reasons for the failure of the index procedure.
The pathogenesis of recurrent hallux valgus is multifactorial, but it is most frequently attributed to an improperly chosen initial surgical procedure or flawed surgical technique. A classic example is the application of a simple distal chevron osteotomy for a deformity that possesses a severe first-second intermetatarsal angle (IMA), where a proximal osteotomy or a first tarsometatarsal (TMT) arthrodesis (Lapidus procedure) would have been biomechanically requisite. Unrecognized or uncorrected metatarsus primus varus is a major culprit in these failures. Metatarsus primus varus involves an increase in the IMA secondary to the obliquity, hypermobility, or inherent instability of the first TMT joint. If this proximal instability is left unaddressed, the persistent metatarsus primus varus will inevitably create a relentless valgus moment at the first MTP joint, ensuring that the deformity will progress over time regardless of the distal correction achieved.


Soft tissue imbalances also play a critical role in the patho-epidemiology of recurrence. An intact adductor hallucis tendon or a persistently tight lateral joint capsule will continuously exacerbate the valgus moment across the first MTP joint. During the primary surgery, failure to perform an adequate lateral soft tissue release allows these deforming forces to overpower the medial capsulorrhaphy and bony fixation. Less frequently, but equally important, factors such as poor host bone or soft tissue quality, deep space infection, patient noncompliance with postoperative weight-bearing restrictions, and catastrophic instrumentation failure can precipitate recurrent hallux valgus. Furthermore, underlying systemic conditions such as generalized ligamentous laxity (e.g., Ehlers-Danlos or Marfan syndrome) or rheumatoid arthritis can predispose patients to rapid recurrence despite technically sound primary interventions.
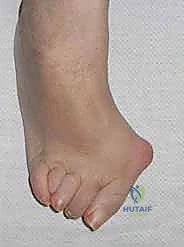
The natural history of recurrent hallux valgus is generally one of progressive deterioration, though some mild, partial recurrences may remain asymptomatic and tolerable with nonoperative management. As the deformity worsens, the medial eminence prominence leads to localized pain, exquisite tenderness, and recurrent overlying adventitial bursitis. More insidiously, the progressive valgus drift and lateralization of the hallux compromise the weight-bearing capacity of the first ray. This insufficiency inevitably leads to transfer metatarsalgia, characterized by second toe overload, plantar plate attenuation, and ultimately, structural failure of the lesser MTP joints. Prolonged hallux valgus, particularly in the setting of an incongruent first MTP joint, will eventually precipitate degenerative chondral changes and advanced osteoarthritis at both the first MTP and the first and second TMT joints.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy of the first ray is non-negotiable when undertaking revision hallux valgus correction, as the normal anatomical planes are frequently obliterated by postoperative scarring from the index procedure. The foundation of the first ray is the first TMT joint, which anatomically measures approximately 27 to 30 mm in depth and possesses a highly irregular, kidney-shaped articular surface. This articulation is stabilized by a robust capsuloligamentous complex, including the critical Lisfranc ligament, which tethers the medial cuneiform to the base of the second metatarsal. Hypermobility at this first TMT joint—defined clinically as the elevation of the first metatarsal head more than 5 to 8 mm above the level of the second metatarsal head in the sagittal plane—creates a profound valgus moment at the distal MTP joint. This proximal instability is a primary biomechanical contributor to the failure of isolated distal hallux valgus corrections.



The neurovascular anatomy surrounding the first ray is complex and highly vulnerable during revision exposures. The dorsalis pedis artery and the deep peroneal nerve course just lateral to the extensor hallucis longus (EHL) tendon as it crosses the TMT joint. Careful dissection is required to avoid devascularizing the first metatarsal or causing debilitating neuromas. Distally, the dorsal medial cutaneous branch of the superficial peroneal nerve runs along the dorsal medial aspect of the first MTP joint, a structure frequently encountered and occasionally injured during standard medial surgical approaches. On the plantar aspect, the plantar medial cutaneous branches of the medial plantar nerve run adjacent to the first MTP joint near the articulations of the sesamoids. The intraosseous and extraosseous blood supply to the first metatarsal head is particularly tenuous in revision scenarios; the primary arterial supply enters the lateral capsule, making simultaneous aggressive lateral soft tissue releases and distal osteotomies highly risky for inducing avascular necrosis (AVN).
The sesamoid complex and its associated musculotendinous units are integral to the biomechanical stability of the first MTP joint. The medial (tibial) and lateral (fibular) sesamoids are intimately contained within the capsuloligamentous complex of the plantar plate. The two heads of the adductor hallucis muscle (oblique and transverse) converge to form a single tendinous insertion on the base of the proximal phalanx and the lateral sesamoid. In a pathologically subluxated joint, the metatarsal head drifts medially off the sesamoid apparatus, leaving the sesamoids resting in the first web space. If the index surgery failed to restore the sesamoids to their anatomic position beneath the metatarsal head, the intrinsic pull of the adductor hallucis will relentlessly recreate the valgus deformity. Furthermore, chronic subluxation often leads to painful degenerative arthritis at the sesamoid–first metatarsal articulations.
Biomechanically, the first ray must function as a rigid lever arm during the terminal stance phase of the gait cycle. When recurrent hallux valgus occurs, the first metatarsal frequently dorsiflexes and supinates, effectively shortening the functional length of the medial column. This loss of weight-bearing capacity forces the lesser metatarsals—particularly the second metatarsal—to absorb supraphysiologic loads. This lesser metatarsal overload is a hallmark of failed bunion surgery and is a common primary complaint driving patients to seek secondary surgical intervention. The resulting transfer metatarsalgia is often accompanied by the development of intractable plantar keratoses, plantar plate tears, and progressive claw toe deformities, creating a cascading failure of the entire forefoot architecture.

Exhaustive Indications and Contraindications
The decision to proceed with revision hallux valgus surgery must be predicated on a comprehensive clinical evaluation, as the indications are strictly reserved for patients who have failed exhaustive nonoperative management and exhibit clear, objectively identifiable sources of pain and dysfunction. Patients typically present with a primary complaint of a recurrent or uncorrected valgus deformity at the first MTP joint, often accompanied by severe pain over the medial eminence, difficulty accommodating standard footwear, and an overlying adventitial bursitis. A critical indication for operative intervention is the presence of secondary forefoot pathology resulting from first ray insufficiency. Patients frequently report feeling as if there is a "rock in their shoe," which correlates clinically with tenderness under the second MTP joint, callosity or ulceration, and the development of rigid claw toe or hammer toe deformities.
Nonoperative management should always be the first line of defense, particularly for patients with mild to moderate recurrences or those with significant medical comorbidities. Conservative strategies include aggressive shoe wear modification (utilizing footwear with a wide, deep toe box and low heels), custom orthotics with medial arch support for associated pes planus, and targeted metatarsal pads to offload associated second toe overload. Activity modification and the use of toe spacers or night splints may provide symptomatic relief, although they will not alter the structural progression of the deformity. Surgery is indicated only when these nonoperative measures have been exhausted and the patient's quality of life remains unacceptably compromised by pain and functional limitation.
Contraindications to revision surgery must be rigorously respected to avoid catastrophic postoperative complications. Absolute contraindications include active local or systemic infection, severe peripheral arterial disease compromising the vascularity of the foot, and profound patient noncompliance or severe psychiatric illness that would preclude adherence to strict postoperative weight-bearing protocols. Relative contraindications include advanced peripheral neuropathy (e.g., Charcot neuroarthropathy), poorly controlled diabetes mellitus, and severe osteopenia or osteoporosis, which may compromise the integrity of internal fixation. In cases of generalized tissue laxity or profound hypermobility, isolated osteotomies are relatively contraindicated, and the surgeon must strongly consider arthrodesis to achieve durable stability.
The differential diagnosis for a painful, recurrent deformity must be systematically evaluated before finalizing the surgical plan. The surgeon must differentiate between a true biomechanical recurrence and other etiologies such as loss of initial fixation, hardware failure, or an indolent deep space infection. Tenderness at the first TMT joint line, accompanied by dorsal osteophytes, suggests degenerative changes rather than simple hypermobility, which dictates a different surgical approach (e.g., Lapidus arthrodesis rather than a proximal osteotomy). The examiner must also carefully assess the range of motion of the first MTP joint with the hallux valgus deformity passively corrected; severely limited or painful motion is a strong indication that joint-sparing osteotomies will fail and that a primary MTP joint arthrodesis is the most appropriate salvage procedure.
| Category | Specific Factors to Evaluate | Clinical Implications |
|---|---|---|
| Primary Indications | Persistent medial eminence pain, failed conservative care, transfer metatarsalgia, progressive lesser toe deformities. | Warrants surgical reconstruction tailored to the specific anatomical failure (e.g., Lapidus for hypermobility). |
| Absolute Contraindications | Active deep space infection, severe peripheral vascular disease, absolute patient noncompliance. | High risk of amputation, nonunion, or catastrophic failure. Nonoperative management is mandatory. |
| Relative Contraindications | Severe osteoporosis, uncontrolled diabetes mellitus, heavy tobacco use, advanced peripheral neuropathy. | Requires extensive preoperative optimization. Consider arthrodesis over osteotomy to maximize stability. |
| Differential Diagnosis | Indolent hardware infection, nonunion of previous osteotomy, complex regional pain syndrome (CRPS). | Must rule out infection with inflammatory markers/aspiration. Hardware removal and cultures may be required. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for revision hallux valgus correction is an exacting process that begins with a meticulous physical examination. The examiner must actively evaluate for symptoms and signs associated with metatarsus primus varus and first TMT joint hypermobility. Mobility of the first TMT joint is dynamically tested by stabilizing the lesser metatarsal heads with one hand while passively dorsiflexing and plantarflexing the first metatarsal head with the other. The medial lesser toes must be closely inspected for crossover deformity, structural overlap, large plantar keratoses, or impending plantar ulcerations. The plantar surface of the lesser MTP joints is palpated for localized tenderness, and the proximal phalanx is translated dorsally and volarly to evaluate for plantar plate insufficiency and MTP joint instability.



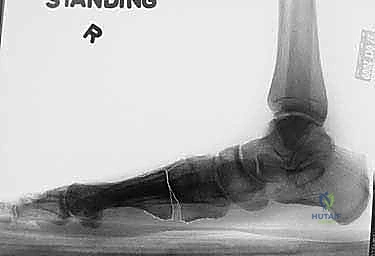
High-quality imaging is the cornerstone of surgical templating. Standard anteroposterior (AP), lateral, and oblique weight-bearing radiographs of the foot must be obtained. The surgeon must systematically evaluate these images for surgical changes from the initial intervention, including the location and integrity of any retained instrumentation. Critical angular measurements include the Hallux Valgus Angle (HVA, normal < 15 degrees), the first-second Intermetatarsal Angle (IMA, normal < 9 degrees), and the Distal Metatarsal Articular Angle (DMAA, normal < 15 degrees). The congruency of the first MTP joint must be assessed; an incongruent joint implies persistent soft tissue imbalance or intrinsic bony deformity. Radiologic signs of metatarsus primus varus include an increased IMA and a visible plantar gap at the first TMT joint on the weight-bearing lateral radiograph, which indicates dorsal translation and instability of the first metatarsal.
Surgical templating involves determining the exact location and geometry of the proposed osteotomies or fusions. Seldom can a failed distal or shaft procedure be successfully revised with another isolated distal procedure. Most salvage operations rely on stabilizing the base of the first metatarsal, as it is possible to achieve significantly greater angular correction at the proximal metaphysis or the TMT joint. The surgeon must account for the age, orientation, and vascular implications of previous surgical incisions. Furthermore, preoperative templating must calculate the anticipated change in first ray length. If the patient already exhibits a relatively short first metatarsal compared to the second metatarsal, further shortening via closing wedge osteotomies must be avoided, and length-preserving or lengthening procedures (such as an opening wedge proximal osteotomy) should be selected. The need for concurrent procedures, such as lesser metatarsal shortening (Weil osteotomies), claw toe corrections, or an Akin phalangeal osteotomy, must be planned in advance.
Patient positioning is standardized but requires attention to detail to facilitate intraoperative imaging and optimal surgical ergonomics. The patient is positioned supine on the operating table. A pneumatic tourniquet is typically placed on the proximal thigh rather than the calf to allow for full evaluation of the gastrocnemius-soleus complex and to provide a larger sterile field, though a calf tourniquet may be used based on surgeon preference. The foot is positioned at the very edge of the bed, often supported by a bump under the ipsilateral hip to internally rotate the leg to a neutral position. The operative extremity must be draped free to allow for unobstructed, multi-planar access for the fluoroscopy C-arm, which is utilized extensively throughout the procedure to verify osteotomy trajectories, hardware placement, and final angular corrections.
Step-by-Step Surgical Approach and Fixation Technique
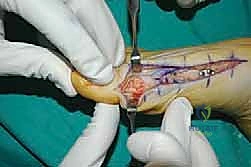
The surgical approach in revision hallux valgus surgery is heavily dictated by the location of prior incisions and the specific reconstructive procedures planned. Whenever possible, previous incisions should be utilized to minimize the risk of skin necrosis, provided they offer adequate exposure. A standard dorsomedial approach is frequently employed; in revision scenarios, this incision is often extended more proximally to expose the metatarsal shaft and base for proximal osteotomies or TMT arthrodesis. Meticulous soft tissue handling is paramount. The dorsal medial cutaneous nerve must be identified and protected. Deep dissection should preserve the periosteal blood supply as much as possible, recognizing that the intraosseous blood supply to the metatarsal head may have been completely disrupted during the prior surgery.


Addressing the distal soft tissue contractures is the next critical step. A lateral release is often necessary to mobilize the MTP joint, typically performed through a separate dorsal first webspace incision. This release may include a transverse adductor tenotomy, release of the fibular sesamoid suspensory ligament, and occasionally a lateral capsulotomy. However, in the setting of a prior distal osteotomy, the blood supply to the metatarsal head is already at significant risk. The primary arterial inflow is located distal to the lateral capsule; therefore, the lateral release must be performed judiciously and selectively to avoid precipitating avascular necrosis of the metatarsal head. Once the soft tissues are balanced, the actual (rather than purely radiographic) Distal Metatarsal Articular Angle (DMAA) can be directly visualized and evaluated.



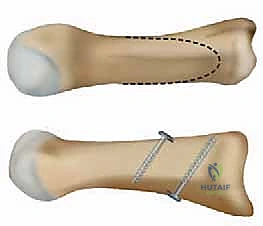
For the bony correction, a proximal osteotomy is frequently indicated to address severe IMA and preserve length. A proximal medial opening wedge osteotomy is an excellent choice when the first metatarsal is short and the patient is experiencing second metatarsal head overload. Under fluoroscopic guidance, a reference pin is placed to determine the trajectory of the osteotomy. A microsagittal saw is used to create an oblique cut, targeting the more proximal aspect of the lateral metatarsal base where the cortex is wider and soft tissue support is robust. The saw cut approaches, but strictly does not violate, the lateral cortex, leaving it intact to act as a stabilizing hinge. The osteotomy is then gently distracted using a sequential triple osteotome technique. This preserves length and reduces the tendency for dorsiflexion malunion. The defect is bone grafted (often with autograft harvested from the lateral calcaneus) and secured with a low-profile medial locking plate and spacer, with at least one proximal screw placed across the osteotomy for enhanced construct rigidity.


In cases where the proximal osteotomy
Clinical & Radiographic Imaging Archive