Akin Osteotomy Masterclass: Precision Correction for Hallux Valgus Interphalangeus

Key Takeaway
Welcome to the OR, fellows. Today, we're performing an Akin osteotomy, a crucial procedure for correcting hallux valgus interphalangeus. This masterclass will guide you through meticulous preoperative planning, essential surgical anatomy, and a granular, step-by-step intraoperative execution. We'll cover precise instrument use, critical pearls, and potential pitfalls, ensuring a comprehensive understanding of this powerful corrective technique.
Comprehensive Introduction and PathoEpidemiology
The Akin osteotomy, initially described by Dr. Charles F. Akin in 1925, remains a cornerstone procedure in modern forefoot reconstructive surgery. Designed as a proximal medial closing wedge osteotomy of the proximal phalanx of the great toe, its primary objective is the precise correction of hallux valgus interphalangeus (HVI). While the original description proposed the Akin osteotomy as an isolated treatment for hallux valgus, contemporary orthopedic consensus strictly reserves this procedure for addressing structural deformities intrinsic to the proximal phalanx or the interphalangeal joint itself. It is now universally recognized that utilizing an isolated Akin osteotomy to correct a primary metatarsophalangeal (MTP) joint deformity is a biomechanical fallacy that inevitably leads to inadequate correction, altered forefoot kinematics, and high rates of clinical recurrence.
Pathophysiologically, hallux valgus interphalangeus is characterized by a lateral deviation of the distal phalanx relative to the longitudinal axis of the proximal phalanx. This deviation can be congenital, stemming from an asymmetric distal articular surface of the proximal phalanx (often termed a "DASA" abnormality—Distal Articular Set Angle), or acquired secondary to long-standing hallux valgus where the interphalangeal joint undergoes adaptive, albeit pathologic, remodeling. The epidemiological profile of HVI suggests a strong female predilection, mirroring the demographics of standard hallux valgus, though isolated congenital HVI can present equally across sexes in pediatric and adolescent populations. Understanding the specific locus of the deformity is paramount; the surgeon must differentiate between MTP joint subluxation, an abnormal proximal articular set angle (PASA), and true HVI to formulate an accurate operative blueprint.
In contemporary practice, the Akin osteotomy is most frequently deployed as a powerful adjunctive procedure. When performing proximal or diaphyseal first metatarsal osteotomies—such as the Scarf, Chevron, or Lapidus arthrodesis—surgeons often encounter residual valgus of the hallux. This residual deformity, even after perfect MTP joint realignment, is typically unmasked by a dynamic load stimulation test intraoperatively. If left uncorrected, the residual interphalangeal valgus will cause the great toe to impinge upon the second digit, leading to crossover toe deformities, transfer metatarsalgia, and patient dissatisfaction. By executing a precisely calculated Akin osteotomy within the robust metaphyseal cancellous bone of the proximal phalanx base, the surgeon can achieve a harmonious, rectus alignment of the entire first ray, optimizing both cosmetic appearance and biomechanical function.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy surrounding the first ray is non-negotiable for the safe execution of the Akin osteotomy. Osteologically, the proximal phalanx of the hallux consists of a concave proximal base, a diaphyseal shaft, and a bicondylar distal head. The optimal site for the Akin osteotomy is within the proximal metaphyseal region, approximately 3 to 5 millimeters distal to the proximal phalangeal flare. This specific anatomical zone is targeted because it is rich in vascularized cancellous bone, which provides an exceptionally favorable environment for rapid osteosynthesis and primary bone healing. Furthermore, operating in this metaphyseal footprint ensures that the osteotomy remains extra-articular, preserving the integrity of the critical MTP joint capsule and articular cartilage.
The soft tissue envelope and musculotendinous structures surrounding the proximal phalanx require meticulous handling. Dorsally, the extensor hallucis longus (EHL) tendon traverses the midline, functioning as the primary dorsiflexor of the interphalangeal joint. Plantarly, the flexor hallucis longus (FHL) tendon runs within a fibrous sheath between the sesamoids and inserts onto the base of the distal phalanx. Medially, the abductor hallucis tendon inserts onto the medial aspect of the proximal phalanx base, while laterally, the adductor hallucis (comprising oblique and transverse heads) inserts onto the lateral base. During a medial approach for an Akin osteotomy, the surgeon must execute a precise subperiosteal dissection to elevate the periosteum without violating the EHL or FHL tendinous sheaths, as iatrogenic injury to these structures can precipitate severe functional deficits, including extensor lag or claw toe deformities.
Neurovascular preservation is perhaps the most critical element of the surgical exposure. The medial dorsal cutaneous nerve, a terminal branch of the superficial peroneal nerve, provides sensory innervation to the dorsomedial aspect of the hallux and is highly vulnerable during the initial skin incision and superficial dissection. Accompanying this nerve are the dorsal digital arteries, which, while smaller than their plantar counterparts, contribute significantly to the angiosome of the dorsal skin flap. Deep to the operative field lie the proper plantar digital nerves and arteries. While a standard medial subperiosteal approach inherently protects these deeper plantar structures, overzealous retraction, errant drilling, or plunging with an oscillating saw can cause catastrophic neurovascular compromise. Biomechanically, correcting the HVI with an Akin osteotomy restores the parallel alignment of the EHL and FHL tendons relative to the longitudinal axis of the first ray, thereby re-establishing the windlass mechanism and ensuring efficient load transfer during the terminal stance phase of the gait cycle.
Exhaustive Indications and Contraindications
The decision to perform an Akin osteotomy must be rooted in stringent clinical and radiographic criteria. The absolute primary indication is symptomatic hallux valgus interphalangeus (HVI), defined radiographically as an interphalangeal angle exceeding 10 degrees. This is most frequently identified intraoperatively following the completion of a first metatarsal osteotomy. The "dynamic load stimulation test"—performed by applying upward pressure on the first metatarsal head to simulate weight-bearing—will unmask any residual valgus at the interphalangeal level. If the hallux continues to abut or under-ride the second toe despite a fully reduced MTP joint, an adjunctive Akin osteotomy is strictly indicated to achieve a congruent, rectus first ray and prevent postoperative hardware failure or deformity recurrence.
Conversely, the contraindications for an Akin osteotomy are equally critical to understand. The most egregious error a surgeon can make is utilizing an isolated Akin osteotomy as the primary surgical intervention for a bunion deformity originating at the MTP joint. Because the Akin procedure does not address the intermetatarsal angle (IMA), the hallux valgus angle (HVA), or MTP joint subluxation, utilizing it in isolation for these pathologies will result in immediate biomechanical failure. Furthermore, advanced degenerative joint disease (osteoarthritis) of the interphalangeal joint is a relative contraindication; in such cases, an interphalangeal joint arthrodesis is the preferred reconstructive option. Active soft tissue infection, osteomyelitis, and severe peripheral vascular disease represent absolute contraindications to any elective forefoot osteotomy.
To facilitate rapid clinical decision-making, the following table delineates the precise indications and contraindications for the Akin osteotomy.
| Clinical Scenario | Status | Rationale and Biomechanical Justification |
|---|---|---|
| Symptomatic Hallux Valgus Interphalangeus (HVI > 10°) | Absolute Indication | Directly addresses the structural deformity within the proximal phalanx or IP joint, restoring linear alignment of the hallux. |
| Residual Valgus Post-Metatarsal Osteotomy | Absolute Indication | Unmasked during dynamic loading; prevents impingement on the lesser digits and restores the parallel pull of the EHL/FHL tendons. |
| Congenital DASA Abnormality | Indication | Corrects the asymmetric distal articular set angle of the proximal phalanx often seen in pediatric/adolescent populations. |
| Primary Treatment for MTP Hallux Valgus | Absolute Contraindication | Fails to address the apex of the deformity (IMA/HVA). Leads to inadequate correction, altered kinematics, and guaranteed recurrence. |
| Advanced IP Joint Osteoarthritis | Relative Contraindication | Osteotomy will not relieve arthritic pain; IP joint arthrodesis is the gold standard for combined deformity and severe arthritis. |
| Severe Peripheral Arterial Disease (PAD) | Absolute Contraindication | High risk of non-healing surgical wounds, avascular necrosis, and potential progression to gangrene or amputation. |
PreOperative Planning Templating and Patient Positioning
Meticulous preoperative planning is the foundation of a successful Akin osteotomy. The clinical assessment must include a thorough evaluation of the patient's neurovascular status, soft tissue envelope, and dynamic gait mechanics. Radiographic analysis requires weight-bearing anteroposterior (AP), lateral, and sesamoid axial views of the foot. The surgeon must systematically measure the intermetatarsal angle (IMA), the hallux valgus angle (HVA), the distal metatarsal articular angle (DMAA), and crucially, the hallux valgus interphalangeus (HVI) angle. The HVI angle is subtended by the longitudinal bisection of the proximal phalanx and the longitudinal bisection of the distal phalanx. An angle greater than 10 degrees confirms the presence of HVI and justifies the inclusion of an Akin osteotomy in the surgical plan.
Radiographic templating is utilized to determine the exact geometry of the closing wedge. The fundamental geometric principle of the Akin osteotomy dictates that for every 1 millimeter of bone resected at the medial base of the wedge, approximately 3 degrees of angular correction is achieved. Therefore, a 15-degree HVI deformity would necessitate a precisely measured 5-millimeter medial wedge resection. During this phase, the surgeon must also pre-select the method of osteosynthesis. While Kirschner wires and interfragmentary screws are viable options, the modern gold standard for metaphyseal fixation in this region is the varisation staple or a shape-memory nitinol staple. These implants provide dynamic, continuous compression across the osteotomy site, mitigating the risk of nonunion and allowing for earlier mobilization.
Optimal patient positioning and anesthetic management are critical for operative efficiency. The procedure is typically performed under a regional anesthetic block—specifically a popliteal sciatic block combined with a saphenous nerve block, or a localized ankle block—supplemented by monitored anesthesia care (MAC) or general anesthesia. This multimodal approach ensures profound intraoperative anesthesia and excellent postoperative analgesia. A pneumatic thigh or calf tourniquet is applied and inflated to 250 mmHg following exsanguination via an Esmarch bandage, providing the requisite bloodless surgical field. The patient is positioned supine on the operating table, with the foot of the bed lowered or removed to grant the surgeon unencumbered 360-degree access to the forefoot. A small bump is placed beneath the ipsilateral hip to neutralize the natural external rotation of the lower extremity, bringing the medial column of the foot directly into the surgeon's line of sight. Finally, the fluoroscopy unit (C-arm) is positioned strategically—usually entering from the contralateral side or the foot of the bed—to allow instantaneous AP and lateral imaging without disrupting the sterile field or requiring patient repositioning.
Step By Step Surgical Approach and Fixation Technique
Incision and Subperiosteal Exposure
The procedure commences with a precise medial longitudinal incision. If the Akin osteotomy is being performed as an adjunct to a first metatarsal osteotomy (e.g., a Scarf procedure), the existing medial incision is simply extended distally over the medial aspect of the proximal phalanx. For an isolated Akin, a 3-to-4-centimeter incision is centered over the medial diaphysis and metaphysis of the proximal phalanx. The incision is carried sharply through the epidermis and dermis. Utilizing blunt dissection with fine scissors, the subcutaneous tissues are carefully parted to identify and mobilize the medial dorsal cutaneous nerve and the accompanying dorsal digital veins, which are gently retracted dorsally.
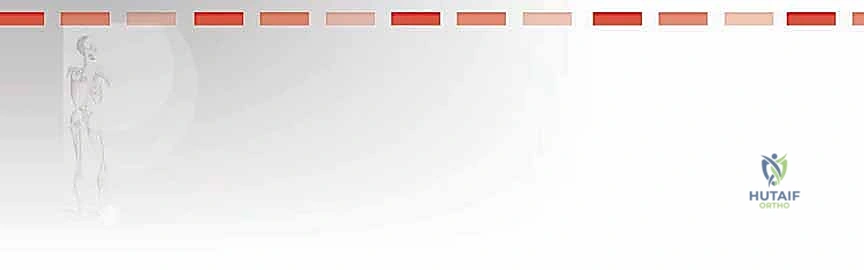
Once the periosteum is visualized, a sharp longitudinal incision is made directly down to bone. A small Freer or Cobb elevator is then employed to perform a meticulous subperiosteal dissection. It is imperative to elevate the periosteum dorsally and plantarly just enough to expose the metaphyseal bone, creating a safe zone that inherently protects the extensor hallucis longus (EHL) dorsally and the flexor hallucis longus (FHL) plantarly from the oscillating saw blade.
Tendon Protection and Retraction
With the osseous anatomy exposed, specialized retractors are deployed to maintain the surgical corridor while safeguarding the vital soft tissues. Two small, pointed retractors—such as mini-Hohmann or Senn retractors—are placed subperiosteally. The dorsal retractor is carefully positioned to elevate and protect the EHL tendon and the dorsal neurovascular bundle. The plantar retractor is positioned to depress and protect the FHL tendon and the plantar neurovascular structures.
The surgeon must visually confirm that the tips of the retractors are resting securely on the bone and are not inadvertently compressing or tethering the neurovascular bundles. This stable, highly visible window is the prerequisite for accurate osteotomy execution.
Kirschner Wire Placement and Joint Verification
To dictate the trajectory and precise location of the proximal osteotomy cut, a 1.0mm or 1.2mm Kirschner wire (K-wire) is driven into the medial aspect of the proximal phalanx. The entry point is meticulously selected to be approximately 3 to 5 millimeters distal to the proximal phalangeal flare. The K-wire is directed laterally, parallel to the articular surface of the MTP joint.
Before proceeding, the surgeon must absolutely verify that this guide wire is extra-articular. This is achieved clinically by applying gentle axial traction to the hallux and directly visualizing the interphalangeal joint space to ensure the wire has not breached the cartilage.

If there is any ambiguity, multi-planar fluoroscopy must be utilized to confirm the extra-articular status of the K-wire. Once verified, the K-wire is removed, and the pilot hole is marked with a sterile surgical marker or methylene blue. This mark serves as the definitive reference point for the proximal saw cut.

Performing the Closing Wedge Osteotomy
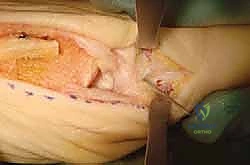
The osteotomy is performed using a sagittal oscillating saw equipped with a fine-toothed, narrow blade. The proximal cut is initiated at the marked pilot hole and directed laterally, strictly parallel to the base of the proximal phalanx. The most critical technical nuance of the Akin osteotomy is the preservation of the lateral cortical hinge. The surgeon must score the lateral cortex but deliberately avoid full penetration.
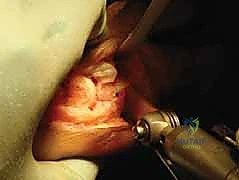
Following the proximal cut, the distal cut is initiated. The starting point for the distal cut on the medial cortex is determined by the preoperatively templated wedge size (e.g., 3-5 millimeters distal to the first cut). The saw blade is angled proximally and laterally to intersect the apex of the proximal cut, precisely at the intact lateral cortex.
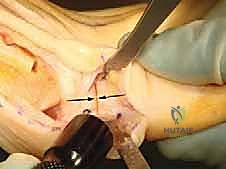
Once both cuts intersect, the resulting triangular wedge of cancellous bone is carefully extracted using a small osteotome, curette, or rongeur. The removal of this wedge must be complete to ensure there is no bony debris obstructing the closure of the osteotomy gap.

Osteoclasis, Closure, and Stable Fixation
With the wedge removed, the surgeon performs a controlled osteoclasis—often referred to as "greensticking" the lateral cortex. By applying a gentle, sustained varus force to the distal phalanx, the medial osteotomy gap is closed. The intact lateral cortex acts as a tension band and hinge, providing immense intrinsic stability to the construct.

Once the osteotomy is fully reduced and the hallux is clinically straight, fixation is applied. While various methods exist, a varisation staple or a shape-memory nitinol staple is highly favored. Drill holes are created on either side of the osteotomy line, parallel to each other and perpendicular to the medial cortex.
The chosen staple is then inserted and fully seated using a tamp and mallet. The compressive forces of the staple ensure intimate bone-to-bone contact across the metaphyseal osteotomy site.

The final construct is rigorously tested for stability, and intraoperative fluoroscopy is utilized to confirm perfect alignment, complete closure of the medial wedge, preservation of the lateral hinge, and extra-articular hardware placement. The wound is then copiously irrigated, and the periosteum, subcutaneous tissue, and skin are closed in a layered fashion.
Complications Incidence Rates and Salvage Management
While the Akin osteotomy is generally considered a highly successful and reliable procedure, it is not immune to complications. The most frequently encountered intraoperative complication is the inadvertent fracture or complete transection of the lateral cortical hinge. This instantly converts a highly stable, hinged osteotomy into a highly unstable, complete transverse fracture. If the lateral hinge is breached, staple fixation alone is often insufficient. The surgeon must immediately pivot to a more rigid osteosynthesis strategy, typically involving crossed Kirschner wires or a specialized locking mini-plate to prevent postoperative displacement, malunion, or nonunion.
Postoperative complications include delayed union or nonunion, which, while rare in the highly vascularized metaphyseal bone, can occur in patients with compromised healing capacity (e.g., smokers, diabetics) or if thermal necrosis occurred due to aggressive saw use without adequate irrigation. Hardware prominence is another notable issue; staples or screw heads left proud on the medial cortex can cause significant soft tissue irritation and bursitis, necessitating secondary surgical procedures for hardware removal once radiographic union is achieved.
Iatrogenic neurovascular injury, particularly to the medial dorsal cutaneous nerve, can result in painful neuromas or localized dysesthesia. Overcorrection (resulting in hallux varus) or undercorrection (residual hallux valgus) usually stems from inaccurate preoperative templating or failure to respect the 1mm to 3-degree correction ratio. The following table summarizes these complications, their estimated incidence, and salvage management strategies.
| Complication | Estimated Incidence | Prevention Strategy | Salvage and Management |
|---|---|---|---|
| Lateral Cortical Hinge Fracture | 5% - 10% | Careful tactile feedback with the oscillating saw; stopping 1-2mm short of the lateral cortex. | Abandon staple; convert to crossed K-wires or a mini-fragment locking plate for rigid stability. |
| Hardware Prominence/Irritation | 10% - 15% | Use low-profile implants; ensure staples are fully tamped and flush with the medial cortex. | Conservative shoe wear modification; elective hardware removal post-radiographic union (typically > 6 months). |
| Delayed Union / Nonunion | < 2% | Operate strictly within the metaphyseal flare; use continuous irrigation to prevent thermal necrosis. | Prolonged immobilization; bone stimulators; revision surgery with bone grafting and rigid internal fixation. |
| Overcorrection (Hallux Varus) | 1% - 3% | Precise geometric templating; avoid excessive wedge resection; confirm alignment under fluoroscopy. | Soft tissue releases (abductor hallucis); revision opening wedge osteotomy if deformity is rigid and symptomatic. |
| Nerve Injury / Neuroma | 2% - 5% | Meticulous blunt superficial dissection; strict subperiosteal plane adherence. | Desensitization therapy; gabapentinoids; surgical excision of neuroma and burying the proximal stump into muscle/bone. |
Phased PostOperative Rehabilitation Protocols
The postoperative rehabilitation following an Akin osteotomy is dictated by the stability of the fixation and whether the procedure was performed in isolation or in conjunction with a more proximal metatarsal osteotomy. In the standard scenario where an Akin is combined with a Scarf or Chevron osteotomy, the rehabilitation protocol is phased to protect the osteotomies while preventing debilitating joint stiffness. Phase I (Weeks 0-2) focuses on wound healing and edema control. The patient is typically placed in a rigid, flat-bottomed postoperative shoe or a controlled ankle motion (CAM) boot. Weight-bearing is strictly limited to heel-touch or flat-foot weight-bearing, explicitly avoiding any propulsive toe-off mechanics that would place sheer stress across the healing proximal phalanx.
Phase II (Weeks 2-6) marks the transition to active rehabilitation. Once the sutures are removed and the incisions are fully healed, patients are encouraged to begin gentle, active range-of-motion (ROM) exercises for both the MTP and interphalangeal joints. This is critical to prevent arthrofibrosis, a common complication that can severely limit functional outcomes. Weight-bearing in the rigid shoe is progressively increased as tolerated. Radiographs are typically obtained at the 4-to-6-week mark to assess callus formation and progression toward clinical union. If the lateral hinge was preserved and fixation is secure, evidence of early osseous bridging should be visible.
Phase III (Weeks 6-12) involves the gradual transition back to normal footwear and functional activities. Once radiographic union is confirmed, the patient is weaned out of the postoperative shoe and into a supportive, wide-toed athletic shoe. Physical therapy focuses on aggressive ROM restoration, strengthening of the intrinsic foot musculature, and gait retraining to restore a normal heel-to-toe propulsive gait cycle. High-impact activities, such as running or jumping, are strictly prohibited until at least 10 to 12 weeks postoperatively, ensuring that the metaphyseal bone has fully remodeled and can withstand physiologic loading forces without risk of stress fracture or hardware failure.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the Akin osteotomy is well-documented in the orthopedic literature, reflecting its transition from a primary procedure to an indispensable adjunctive technique. Dr. Charles Akin’s original 1925 publication in the Journal of Bone and Joint Surgery laid the geometric foundation for the proximal phalangeal closing wedge, though his assertion that it could independently cure hallux valgus has been definitively refuted by modern biomechanical studies. The seminal work by Barouk in the late 1990s and early 2000s revolutionized forefoot surgery by demonstrating the synergistic power of combining the Scarf metatarsal osteotomy with the Akin phalangeal osteotomy. Barouk’s extensive clinical series proved that addressing both the metatarsal and phalangeal apices of deformity yielded significantly lower recurrence rates and higher patient satisfaction scores compared to isolated metatarsal procedures.
Recent literature has heavily focused on the optimization of fixation techniques. A landmark prospective randomized controlled trial comparing staple fixation versus single interfragmentary screw fixation for Akin osteotomies demonstrated no statistically significant difference in ultimate union rates. However, the staple cohort exhibited a shorter operative time and a lower incidence of symptomatic hardware requiring subsequent removal. Furthermore, biomechanical studies evaluating shape-memory nitinol staples have shown superior continuous compressive forces across the osteotomy gap compared to static titanium staples, theoretically enhancing the biological environment for primary bone healing.
Current clinical guidelines from leading orthopedic and podiatric surgical societies emphasize that the Akin osteotomy should be viewed as a precision tool for fine-tuning first ray alignment. The consensus strictly advises against its use as a standalone procedure for MTP joint pathology. Surgeons are encouraged to routinely utilize intraoperative dynamic loading tests to unmask residual HVI and to have a low threshold for adding an Akin osteotomy to their reconstructive algorithms. By respecting the intricate anatomy, adhering to strict geometric principles, and utilizing modern stable fixation, the Akin osteotomy remains an elegantly simple yet profoundly effective procedure in the master surgeon's armamentarium.
