Surgical Management of Patellofemoral Instability and Dislocation
Key Takeaway
Surgical intervention for patellar dislocation is dictated by the underlying pathoanatomy. Acute operative indications include osteochondral fractures and loose bodies. For recurrent instability, procedures range from medial patellofemoral ligament (MPFL) reconstruction to distal tibial tubercle osteotomies. Successful outcomes rely on correcting specific anatomical deficits, such as abnormal tibial tubercle-trochlear groove (TT-TG) distances, while avoiding complications like medial overtightening or physeal arrest in pediatric patients.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of patellofemoral instability represents one of the most complex, highly scrutinized, and nuanced domains in operative orthopaedics. The patellofemoral joint relies on an intricate, highly interdependent interplay of static osseous geometry, passive ligamentous restraints, and dynamic muscular forces. When this delicate biomechanical balance is disrupted—whether through an acute, high-energy traumatic event or chronic, insidious anatomical malalignment—the resulting instability inevitably leads to profound functional impairment, debilitating apprehension, and progressive chondral degeneration. Historically, more than 100 distinct surgical procedures have been described for the treatment of patellofemoral instability in the orthopaedic literature. This staggering number reflects both the inherent complexity of the joint’s functional anatomy and a historical lack of consensus on a single universally applicable "gold standard" procedure. Today, the orthopaedic paradigm has definitively shifted toward an à la carte approach, wherein the surgical strategy is meticulously tailored to the specific pathoanatomic deficits of the individual patient.
The epidemiology of patellofemoral dislocation demonstrates a distinct predilection for the young, active population, with the highest incidence occurring in adolescents and young adults in their second decade of life. The overall incidence of primary patellar dislocation is estimated to be between 5.8 and 29 per 100,000 person-years, but this figure spikes dramatically to over 100 per 100,000 in the high-risk demographic of adolescent females. The natural history of a first-time dislocator managed non-operatively is fraught with high recurrence rates, ranging from 15% to 44%, and this risk escalates exponentially with each subsequent dislocation event. Furthermore, patients with baseline anatomical risk factors, such as trochlear dysplasia, patella alta, or excessive lateralization of the tibial tubercle, face an even higher propensity for recurrent instability and early-onset patellofemoral osteoarthritis.
The progressive deterioration of the knee joint in the setting of recurrent instability is multifactorial and biologically devastating. Without surgical stabilization, the patient often develops profound apprehension, consciously or subconsciously altering their gait and avoiding activities that load the extensor mechanism in flexion. With continued recurrence, the articulating surfaces degenerate not merely because the patella occasionally dislocates, but because the excursions of the patella are fundamentally abnormal during every single cycle of knee motion. This chronic maltracking causes repetitive microtrauma, elevated shear stresses, and focal overloading of the articular cartilage, particularly on the lateral facet and the median ridge of the patella.
Therefore, the key to successful surgical intervention is correctly identifying and addressing the specific pathological anatomy producing the instability. No single operation is universally successful; rather, the complexity of the procedure chosen must be precisely matched to the problem identified. The contemporary orthopaedic surgeon must focus on reproducible, low-risk, high-reward techniques with historically high success rates, avoiding the temptation to apply a uniform surgical algorithm to a highly heterogeneous patient population.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of patellofemoral anatomy and biomechanics is the foundational prerequisite for any surgeon attempting to correct instability. The stability of the patella within the trochlear groove is governed by three primary categories of restraints: active muscular stabilizers, passive soft-tissue tethers, and static osseous geometry. The primary active stabilizer is the quadriceps musculature, specifically the vastus medialis obliquus (VMO). The VMO fibers insert onto the superomedial border of the patella at an angle of 50 to 55 degrees relative to the femoral shaft, providing a crucial dynamic medializing vector that opposes the natural lateralizing pull of the vastus lateralis and the overall extensor mechanism. In the setting of chronic instability, the VMO often becomes dysplastic or atrophic, exacerbating the lateral tracking of the patella.
The passive soft-tissue restraints are dominated by the Medial Patellofemoral Ligament (MPFL), a distinct thickening of the medial retinaculum located in layer two of the medial knee. Advanced cadaveric and biomechanical studies have definitively established that the MPFL is the primary passive restraint against lateral patellar translation, providing 50% to 60% of the restraining force from 0 to 30 degrees of knee flexion. The MPFL originates from a highly specific footprint on the medial femur, famously mapped radiographically by Schöttle et al. (Schöttle's point). This origin is located between the adductor tubercle and the medial epicondyle, slightly posterior to the posterior extension of Blumensaat's line on a true lateral radiograph. From this origin, the ligament fans out to insert on the proximal half to upper two-thirds of the medial patellar border. Secondary soft-tissue stabilizers include the medial patellotibial ligament (MPTL) and the medial patellomeniscal ligament (MPML), which contribute to stability at higher degrees of flexion once the MPFL becomes relatively lax.
The static osseous geometry of the patellofemoral joint becomes the dominant stabilizing factor as the knee flexes past 30 degrees. At this point, the patella fully engages the trochlear groove of the femur. The depth and morphology of the trochlea are critical; a dysplastic, flattened, or convex trochlea (as classified by Dejour) removes this essential bony constraint, allowing the patella to subluxate laterally even under normal physiological loads. The lateral facet of the normal trochlea is higher and more prominent than the medial facet, providing a physical buttress against lateral patellar excursion. When this buttress is deficient, the soft-tissue restraints are subjected to supraphysiologic stresses, inevitably leading to failure.
Furthermore, the overall alignment of the extensor mechanism, quantified by the Q-angle and the Tibial Tubercle-Trochlear Groove (TT-TG) distance, plays a pivotal role in patellofemoral biomechanics. A TT-TG distance greater than 20 mm on axial computed tomography (CT) indicates a severe lateralization of the extensor vector, which cannot be overcome by soft-tissue reconstruction alone. Similarly, patella alta (an abnormally high-riding patella) delays the engagement of the patella into the protective trochlear groove during early flexion, leaving the joint entirely dependent on the vulnerable MPFL for stability during the critical 0 to 30-degree arc of motion.
Exhaustive Indications and Contraindications
The decision-making process for surgical intervention in patellofemoral instability requires a meticulous synthesis of the patient's clinical history, physical examination, and advanced imaging findings. The indications for surgery are broadly divided into the management of acute, first-time dislocations and the treatment of chronic, recurrent instability. While the majority of first-time, acute patellar dislocations are managed nonoperatively with a brief period of immobilization followed by aggressive physical therapy, specific clinical scenarios mandate early surgical intervention to prevent irreversible joint damage.
Operative intervention for an acute, first-time patellar dislocation is strictly indicated in the presence of an osteochondral fracture, which often occurs as the medial facet of the patella violently impacts the lateral femoral condyle during the dislocation or the subsequent spontaneous reduction. Intra-articular loose body formation, resulting from these shear fractures, acts as a mechanical block to motion and a source of third-body wear, necessitating arthroscopic removal or fixation. Significant disruption of the articular surface requiring anatomical reduction and internal fixation is an absolute indication for acute surgery. Additionally, elite athletic status may prompt early surgical consideration; competitive athletes at or near the end of their season who plan to pursue high-level athletic activities may opt for acute stabilization to mitigate the unacceptable risk of recurrent instability during critical competition.
In the setting of chronic, recurrent patellofemoral malalignment and subluxation, surgical intervention is indicated when exhaustive nonoperative treatment—including core, gluteal, and targeted VMO strengthening—has failed to provide functional stability. If the patient continues to experience dislocations, or if they exhibit profound apprehension that prevents them from engaging in activities of daily living, surgical realignment is necessary. The presence of progressive chondromalacia of the patella, symptomatic osteochondral free fragments, or secondary meniscal pathology further strengthens the indication for operative management. The specific procedure chosen is dictated by the underlying pathoanatomy: isolated soft-tissue failure warrants MPFL reconstruction, while severe bony malalignment necessitates distal realignment via osteotomy.
Conversely, there are strict contraindications to specific patellofemoral procedures that must be rigorously respected to avoid catastrophic iatrogenic complications. The most critical of these pertains to distal realignment procedures involving the tibial tubercle. Bony realignment is absolutely contraindicated in skeletally immature patients with open proximal tibial physes. Furthermore, medializing procedures must be approached with extreme caution in the presence of isolated medial compartment or medial patellar facet arthrosis, as these procedures will invariably increase the contact pressures on the already damaged medial articular surfaces.
| Surgical Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Acute MPFL Repair | Acute first-time dislocation with bony avulsion of MPFL from femur; Elite athlete requiring immediate stability. | Chronic, recurrent instability; Mid-substance MPFL tears (poor tissue quality). | Severe trochlear dysplasia; TT-TG > 20mm. |
| MPFL Reconstruction | Recurrent instability; Failed conservative management; Normal bony anatomy (TT-TG < 20mm). | Severe, uncorrected bony malalignment (e.g., TT-TG > 25mm without concurrent TTO). | Open physes (if using transosseous femoral tunnels that cross the physis). |
| Tibial Tubercle Osteotomy (TTO) | TT-TG distance > 20mm; Severe patella alta (Caton-Deschamps > 1.2); Distal/lateral patellar chondral lesions. | Open proximal tibial physis (Risk of genu recurvatum); Isolated medial facet arthrosis. | Active infection; Severe systemic medical comorbidities. |
| Trochleoplasty | Severe symptomatic trochlear dysplasia (Dejour Type B or D) with supratrochlear spur and recurrent instability. | Open physes; Advanced patellofemoral osteoarthritis; Thin trochlear cartilage (<3mm). | Inexperienced surgeon (highly technically demanding procedure). |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for patellofemoral surgery is an exhaustive process that relies heavily on precise radiographic measurements and a highly detailed physical examination. The clinical examination must assess the overall mechanical axis of the lower extremity, checking for excessive genu valgum or femoral anteversion, which can exacerbate lateral patellar tracking. The "J-sign" (abnormal lateral translation of the patella during terminal extension) should be documented. The patellar apprehension test and the moving patellar apprehension test are critical for confirming the diagnosis and assessing the degree of soft-tissue laxity. Furthermore, the surgeon must evaluate the patient for generalized ligamentous laxity using the Beighton score, as hypermobile patients frequently experience higher failure rates with isolated soft-tissue reconstructions and may require augmented or combined procedures.
Imaging is the cornerstone of surgical templating. A standard knee series must include weight-bearing anteroposterior (AP), true lateral (flexed to 30 degrees), and axial (Merchant or Sunrise) views. The true lateral radiograph is indispensable for calculating patellar height using the Caton-Deschamps or Insall-Salvati indices. It is also the primary modality for evaluating trochlear dysplasia, looking for the "crossing sign" (where the line of the trochlear groove crosses the anterior border of the lateral condyle), the presence of a supratrochlear spur, and the "double contour sign" indicative of a hypoplastic medial facet. Axial views provide a static assessment of patellar tilt and lateral subluxation.
Advanced cross-sectional imaging is mandatory for surgical decision-making. Computed Tomography (CT) is the gold standard for measuring the Tibial Tubercle-Trochlear Groove (TT-TG) distance. The surgeon superimposes axial cuts through the deepest portion of the trochlear groove and the most anterior portion of the tibial tubercle. A TT-TG distance of less than 15 mm is considered normal, 15 to 20 mm is borderline, and greater than 20 mm is pathognomonic for severe lateralization, dictating the necessity of a Tibial Tubercle Osteotomy (TTO). Magnetic Resonance Imaging (MRI) is essential for evaluating the integrity of the MPFL, identifying the exact location of the tear (femoral avulsion vs. mid-substance vs. patellar avulsion), and assessing the extent of acute osteochondral injuries or chronic chondromalacia that may require concurrent cartilage restoration procedures.
Patient positioning and operating room setup must be meticulously executed to ensure optimal visualization and dynamic assessment during the procedure. The patient is positioned supine on a standard radiolucent operating table. A well-padded tourniquet is applied high on the proximal thigh. The operative leg is prepped and draped free to allow a full, unencumbered 0 to 120-degree range of motion. A lateral post or a specialized leg holder can be utilized for the arthroscopic portion of the case, but it must be easily removable or adjustable so that it does not artificially alter the tracking of the patella during the open realignment and tensioning phases. Fluoroscopy must be readily available and positioned to allow for perfect true lateral imaging of the knee, which is absolutely critical for identifying Schöttle's point during MPFL reconstruction.
Step-by-Step Surgical Approach and Fixation Technique
During all operative procedures for recurrent dislocation or subluxation of the patella, a thorough arthroscopic inspection of the articular surfaces and intraarticular structures is mandatory. This diagnostic step dictates the final surgical strategy, allowing the surgeon to address concurrent meniscal pathology, remove loose bodies, and directly visualize the tracking of the patella from the superior portal before and after the planned reconstruction.
Medial Patellofemoral Ligament (MPFL) Reconstruction
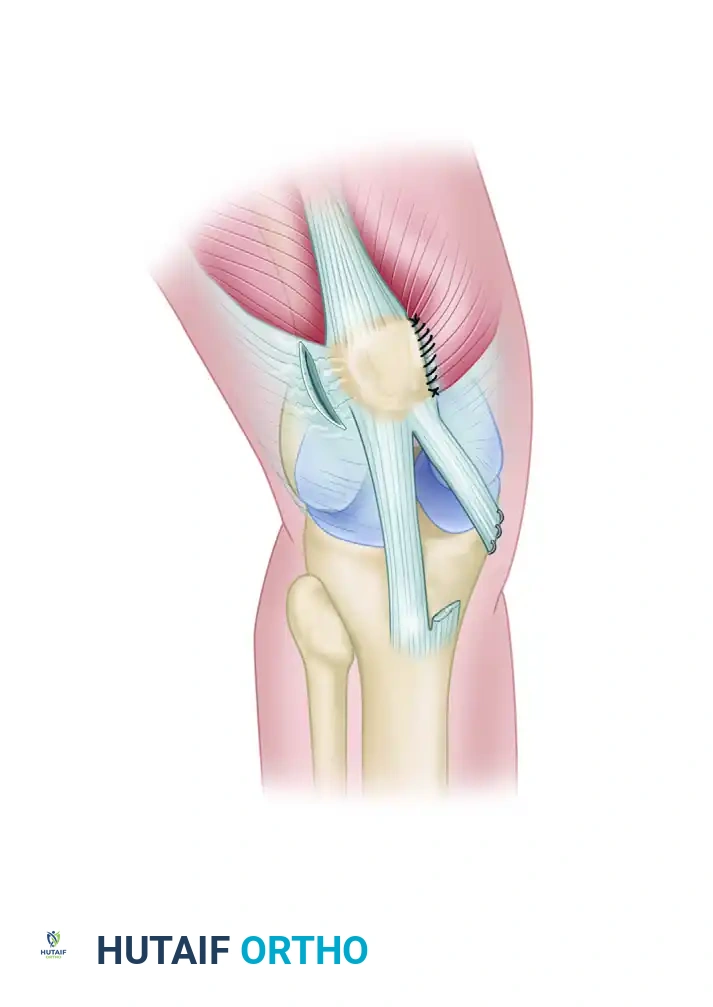
MPFL reconstruction has emerged as the gold standard for recurrent patellofemoral instability in the absence of severe bony malalignment. The procedure begins with the harvesting of a soft-tissue graft, most commonly the gracilis or semitendinosus autograft, though allografts are frequently utilized to decrease donor site morbidity. The patellar insertion is addressed first. A small longitudinal incision is made over the superomedial border of the patella. The graft is fixed to the upper half of the medial patellar facet using either two small biocomposite suture anchors or via a transosseous tunnel technique, ensuring the graft is positioned deep to the VMO fascia to replicate native anatomy.
The critical step is the accurate identification of the femoral footprint. Using fluoroscopy, a true lateral image of the knee is obtained, ensuring perfect overlap of the posterior femoral condyles. Schöttle's point is identified: 1 mm anterior to the posterior cortex extension line, 2.5 mm distal to the posterior origin of the medial femoral condyle, and proximal to the level of the posterior point of Blumensaat's line. A guide pin is placed at this exact location, and the graft is looped around it. The knee is then taken through a full range of motion. The graft must be isometric or slightly slack in deep flexion; if the graft tightens excessively in flexion, the femoral point is too anterior and must be repositioned. Once the optimal isometric point is confirmed, a blind tunnel is reamed, the graft is passed into the tunnel, and fixed with a bioabsorbable interference screw with the knee held at 30 degrees of flexion to restore the native check-rein function of the ligament.
Proximal and Distal Soft Tissue Realignment (The "Three-in-One" Procedure)
For patients with recurrent instability without severe underlying bony malalignment (e.g., normal TT-TG distance), soft tissue realignment procedures are historically utilized. The classic "Three-in-One" procedure combines lateral decompression with medial tightening and distal soft-tissue vector realignment. While largely superseded by anatomical MPFL reconstruction in modern practice, it remains a valuable technique in specific pediatric populations or as an augmentative procedure.
The surgical steps of the Three-in-One Procedure involve meticulous soft tissue balancing. First, a Lateral Release is performed. The lateral retinaculum is released from the inferior pole of the patella to the superior extent of the vastus lateralis to decompress the lateral facet and allow the patella to centralize. Extreme care must be taken to preserve the superior lateral geniculate artery to prevent catastrophic patellar avascular necrosis. Second, a Vastus Medialis Muscle Advancement is executed. The VMO is mobilized and advanced distally and laterally over the patella, suturing it under tension to increase its dynamic medializing force during terminal extension. Finally, the Transfer of the Medial Third of the Patellar Tendon is performed. The medial third of the patellar tendon is sharply detached from the tibial tubercle, routed medially, and sutured to the medial collateral ligament (MCL) or the medial tibia using two metal or biocomposite suture anchors. This alters the distal pull vector, tethering the patella against lateral subluxation without violating the proximal tibial physis.
Distal Realignment: Tibial Tubercle Osteotomy (TTO)
When the primary pathology is an abnormal lateralization of the tibial tubercle (TT-TG > 20 mm) or severe patella alta, a bony distal realignment is required. The Fulkerson anteromedialization osteotomy is the workhorse procedure for this indication. An anterior longitudinal incision is made lateral to the tibial crest. The anterior compartment musculature is elevated off the lateral tibia. Using an oscillating saw, an oblique osteotomy is performed starting proximal to the patellar tendon insertion and exiting distally on the anterior tibial crest.
The angle of the osteotomy cut dictates the ratio of anteriorization to medialization. A steeper cut (e.g., 60 degrees relative to the coronal plane) provides more medialization and less anteriorization, while a shallower cut (e.g., 45 degrees) provides greater anteriorization, which is highly beneficial for unloading symptomatic distal and lateral patellar chondral lesions. The osteotomized tubercle pedicle, with the patellar tendon attached, is translated medially (typically 10 to 15 mm) and anteriorly. It is temporarily held with K-wires while patellar tracking is arthroscopically confirmed. Once tracking is perfectly centralized, the osteotomy is rigidly fixed using two fully threaded 4.5 mm cortical screws placed in lag fashion from anterior to posterior, engaging the posterior tibial cortex for maximum pull-out strength.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, patellofemoral stabilization procedures carry a distinct profile of potential complications. The most devastating complication is the recurrence of instability, which can occur due to failure to address underlying bony malalignment, improper graft tensioning, or traumatic rupture of the reconstruction. Arthrofibrosis and profound loss of knee flexion represent another major category of complications, almost exclusively resulting from iatrogenic over-tensioning of the MPFL graft or prolonged postoperative immobilization. If the MPFL graft is fixed in extension or if the femoral tunnel is placed too anteriorly, the graft will act as a rigid tether, preventing the knee from flexing past 90 degrees and causing severe medial compartment pain.
Patellar fracture is a highly morbid complication specifically associated with procedures that violate the patellar cortex, such as transosseous MPFL reconstructions or aggressive medial reefing. The use of large drill holes or the placement of anchors too close to the articular margin creates stress risers that can propagate into catastrophic transverse or multi-part fractures during the early rehabilitation phase. Medial subluxation of the patella is a purely iatrogenic complication caused by excessive medialization of the tibial tubercle or gross over-tensioning of the medial soft tissues. This results in rapid, severe degeneration of the medial patellar facet and profound disability, as the patient experiences instability and pain during normal gait.
In the setting of Tibial Tubercle Osteotomies, unique bony complications arise. Delayed union or nonunion of the osteotomy site occurs in approximately 1-2% of cases, often necessitating bone grafting and revision internal fixation. Proximal tibial fracture can occur if the distal hinge of the osteotomy is cut too thin or if the screws are placed too close together, creating a stress riser in the metaphyseal bone. Deep Vein Thrombosis (DVT) and surgical site infections are inherent risks to any major lower extremity orthopedic procedure and must be managed with appropriate prophylaxis and aggressive early intervention.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Recurrent Instability | 5% - 15% | Unrecognized elevated TT-TG, severe trochlear dysplasia, graft failure. | Revision surgery: Address missed bony pathology (add TTO or Trochleoplasty), revision MPFL. |
| Arthrofibrosis / Stiffness | 3% - 10% | Over-tensioning of MPFL graft, anterior femoral tunnel placement, prolonged immobilization. | Aggressive PT, Arthroscopic lysis of adhesions, Manipulation under anesthesia (MUA), Graft release. |
| Patellar Fracture | 1% - 3% | Transosseous tunnels creating stress risers, aggressive lateral release compromising blood supply. | Open Reduction Internal Fixation (ORIF) with tension band wiring or cannulated screws. |
| Iatrogenic Medial Subluxation | < 2% | Excessive medialization during TTO, gross over-tensioning of medial soft tissues. | Revision TTO (lateralization), release of medial structures, MPFL reconstruction (if deficient). |
| TTO Nonunion / Delayed Union | 1% - 2% | Smoking, poor fixation construct, premature weight-bearing. | Revision ORIF with bone grafting (autograft or orthobiologics), extended non-weight bearing. |
Phased Post-Operative Rehabilitation Protocols
The ultimate clinical success of any patellofemoral stabilization procedure is heavily dependent on strict adherence to a highly structured, phased postoperative rehabilitation protocol. The delicate balance between protecting the surgical repair and restoring normal joint kinematics requires constant communication between the surgeon and the physical therapy team. The goals are to protect the healing soft tissues or osteotomy, restore normal patellofemoral tracking, reactivate the quadriceps musculature, and prevent the onset of arthrofibrosis.
Phase I: Maximum Protection and Early Motion (Weeks 0-4)
In the immediate postoperative period, the primary objective is the protection of the surgical construct while initiating early, controlled motion to nourish the articular cartilage and prevent capsular contracture. For isolated soft-tissue procedures (MPFL reconstruction), patients are typically allowed to weight-bear as tolerated (WBAT) in a hinged knee brace locked in full extension to prevent sudden buckling. For procedures involving a Tibial Tubercle Osteotomy, weight-bearing is restricted to partial (e.g., 50%) or touch-down weight-bearing with crutches to protect the osteotomy site until early radiographic consolidation is evident. Range of motion (ROM) is initiated immediately but is strictly controlled. For MPFL reconstructions, ROM is usually permitted from 0 to 90 degrees; flexing past 90 degrees in the early healing phase places excessive strain on the graft-bone interface. Immediate initiation of quadriceps sets, straight leg raises (performed strictly within the locked brace to avoid extensor lag), and core strengthening are mandatory to prevent profound muscle atrophy.
Phase II: Moderate Protection and ROM Restoration (Weeks 4-8)
As the patient enters the second month postoperatively, biological healing of the soft tissues and early callus formation at the osteotomy site allow for progression. The hinged knee brace is gradually unlocked to allow functional motion during ambulation and is eventually discontinued entirely once the patient demonstrates excellent quadriceps control and the complete absence of an extensor lag during a straight leg raise. Range of motion is progressed with the goal of achieving full, symmetrical flexion and extension by the end of week 8. Strengthening exercises transition from isometric to closed kinetic chain (CKC) activities. CKC exercises, such as mini-squats, wall slides, and leg presses (limited to 0-60 degrees initially), are highly preferred over open kinetic chain exercises. Open kinetic chain extension (especially from 30 to 0 degrees) places maximum shear force on the patellofemoral joint and can stretch the medial repair. Focus is heavily placed on VMO activation and gluteal/hip abductor strengthening to control femoral internal rotation, which is a major dynamic contributor to lateral patellar maltracking.
Phase III: Advanced Strengthening and Return to Play (Weeks 8-16+)
The final phase of rehabilitation focuses on functional restoration, proprioception, and sport-specific training. Patients progress to advanced strengthening, including unilateral leg presses, step-downs, and proprioceptive drills on unstable surfaces. Plyometric training and agility drills are introduced gradually, monitoring closely for any signs of patellofemoral pain, effusion, or apprehension. Return to competitive sports is a criteria-based decision, not strictly a time-based one. Typically, return to play is permitted between 4 to 6 months postoperatively, contingent upon the patient achieving a completely pain-free full range of motion, the absolute absence of apprehension during dynamic testing, and the restoration of 90% or greater limb symmetry index (LSI) on functional hop testing and isokinetic quadriceps strength evaluations.
Summary of Landmark Literature and Clinical Guidelines
The evolution of patellofemoral surgery is deeply rooted in several landmark biomechanical and clinical studies that have fundamentally reshaped our understanding of the joint. Historically, the treatment of patellar instability was highly empirical, leading to high failure rates and the abandonment of numerous procedures. The modern era of patellofemoral surgery was arguably initiated by the seminal work of Dejour et al. in the late 1980s and 1990s. Dejour’s comprehensive analysis of strict lateral radiographs and CT scans in patients with patellar dislocation identified four major anatomical risk factors: trochlear dysplasia, patella alta, excessive TT-TG distance, and patellar tilt. His classification of trochlear dysplasia remains the international standard and forms the basis for indications regarding trochleoplasty procedures.
The understanding of the medial soft-tissue restraints was revolutionized by biomechanical studies in the early 2000s, most notably by Amis, Senavongse, and Nomura, who definitively quantified the MPFL as the primary restraint to lateral patellar translation. This biomechanical revelation shifted the surgical focus away from non-anatomic procedures (like the Roux-Goldthwait or isolated lateral releases) toward anatomic MPFL reconstruction. The clinical application of this knowledge was perfected by Schöttle et al., whose 2006 radiographic study mapped the exact femoral insertion of the MPFL. "Schöttle's point" is now universally utilized intraoperatively via fluoroscopy to ensure anatomic graft placement, dramatically reducing the historical complication rates of graft over-tensioning and resulting arthrofibrosis.
Regarding distal realignment, Fulkerson's introduction of the anteromedialization osteotomy in 1983 provided a powerful tool for addressing both lateral vector malalignment and concurrent distal/lateral chondral disease. Fulkerson’s biomechanical rationale—that anteriorization unloads the damaged facets while medialization corrects the tracking—has been validated by decades of clinical outcomes, making the TTO the standard of care for patients with a TT-TG distance exceeding 20 mm.
Currently, consensus guidelines from major orthopaedic societies, including the American Academy of Orthopaedic Surgeons (AAOS) and the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS), advocate for the à la carte approach detailed in this chapter. The consensus strongly supports non-operative management for the majority of first-time dislocators, reserving acute surgery for those with osteochondral fractures. For chronic instability, anatomic MPFL reconstruction is universally recognized as the gold standard for isolated soft-tissue failure, while bony realignment procedures are strictly reserved for patients with quantified anatomical abnormalities, emphasizing the critical importance of individualized, pathology-specific surgical intervention.
