Patellar Fracture ORIF: An Intraoperative Masterclass in Tension Band Wiring

Key Takeaway
Welcome, fellows, to a deep dive into patellar fracture ORIF. Today, we'll meticulously explore the anatomy, preoperative planning, and step-by-step intraoperative execution of tension band wiring. We'll cover crucial surgical techniques, potential pitfalls, and comprehensive postoperative care, ensuring you master this essential procedure for restoring knee extensor mechanism integrity and articular congruence.
Patellar Fracture ORIF: An Intraoperative Masterclass in Tension Band Wiring
Comprehensive Introduction and Patho-Epidemiology
Good morning, fellows. Let us scrub in and prepare for today’s case. Today, we are tackling a displaced patellar fracture, a ubiquitous yet highly unforgiving injury that, if not managed with meticulous surgical precision, can severely and permanently compromise knee function. Our primary objective is unequivocal: to restore the absolute integrity of the extensor mechanism and achieve an anatomically congruent articular surface. This is not merely an exercise in osteosynthesis; it is a critical restoration of the intricate biomechanics of the knee joint. Patellar fractures account for approximately 1% of all skeletal injuries, presenting a bimodal epidemiological distribution. We typically observe these injuries in young males following high-energy trauma, such as motor vehicle collisions or sports injuries, and in elderly individuals, predominantly females, secondary to low-energy falls on a flexed knee.
The pathogenesis of patellar fractures is dictated by the mechanism of injury, which broadly categorizes into direct, indirect, or combined forces. Direct trauma, such as a dashboard injury in a high-speed collision, imparts a massive compressive load directly onto the anterior aspect of the patella. This typically results in highly comminuted or stellate fracture patterns, often accompanied by severe chondral damage and significant soft tissue compromise. Conversely, indirect injuries occur when the quadriceps muscle contracts violently against a rapidly flexing knee—a classic eccentric load. The tensile forces generated easily exceed the ultimate tensile strength of the bone, resulting in a transverse fracture pattern. In these indirect scenarios, the medial and lateral retinacula are frequently torn, leading to dramatic fracture displacement and a profound inability to actively extend the knee.



Understanding the patho-epidemiology is paramount for preoperative planning. High-energy direct trauma must raise our clinical index of suspicion for associated injuries, including ipsilateral femoral shaft fractures, posterior hip dislocations, and severe osteochondral sheer injuries of the femoral trochlea. Furthermore, the soft tissue envelope overlying the patella is exceptionally thin. Direct impaction not only shatters the bone but routinely devitalizes the overlying dermis and subcutaneous bursa, drastically increasing the risk of postoperative wound necrosis and deep infection. As orthopedic surgeons, we must approach the soft tissues with the same reverence as the osseous structures.
The clinical presentation is typically unambiguous. Patients present with an acutely swollen, exquisitely tender anterior knee. A palpable defect is frequently present in displaced transverse fractures. However, the most critical element of the physical examination is the assessment of the extensor mechanism. A complete inability to perform a straight leg raise or actively extend the knee against gravity is the hallmark of a functionally disruptive patellar fracture and serves as an absolute indication for surgical intervention. Aspiration of the hemarthrosis, yielding fat lobules, confirms an intra-articular fracture, though this is usually readily apparent on standard orthogonal radiographs.
Detailed Surgical Anatomy and Biomechanics
To master patellar osteosynthesis, one must possess an encyclopedic understanding of its surgical anatomy and biomechanical function. The patella is the largest sesamoid bone in the human body, embedded entirely within the complex tendinous expansion of the quadriceps femoris. Its primary biomechanical role is to act as a dynamic spacer, displacing the quadriceps tendon anteriorly away from the mechanical axis of the femur. This anterior displacement significantly lengthens the moment arm of the extensor mechanism, amplifying the mechanical advantage of the quadriceps by up to 30%. Without the patella, the quadriceps would be forced to generate exponentially higher forces to achieve terminal extension, rapidly leading to muscular fatigue and joint degeneration.




The vascular anatomy of the patella is complex and clinically highly relevant. Blood supply is derived from a rich extraosseous anastomotic ring known as the peripatellar plexus, primarily fed by the supreme, medial superior, medial inferior, lateral superior, lateral inferior, and anterior tibial recurrent genicular arteries. The intraosseous blood supply enters predominantly at the inferior pole and travels in a distal-to-proximal direction. Consequently, transverse fractures, particularly those involving the proximal pole, disrupt this intraosseous flow, placing the superior fragment at a substantial risk for avascular necrosis (AVN). Meticulous surgical dissection that preserves the anterior soft tissue envelope is critical to maintaining whatever extraosseous supply remains intact.
The posterior articular surface of the patella is the thickest articular cartilage in the human body, reaching up to 6 millimeters in depth. It is divided by a vertical ridge into a larger lateral facet and a smaller medial facet. A secondary vertical ridge further subdivides the medial border to create the "odd facet," which only engages the medial femoral condyle in deep flexion (beyond 135 degrees). The biomechanical forces transmitted across this joint are staggering; patellofemoral joint reaction forces can reach up to seven times body weight during deep squatting or stair descent. Any residual articular step-off greater than 2 millimeters drastically alters contact pressures, virtually guaranteeing the rapid onset of severe, debilitating post-traumatic patellofemoral osteoarthritis.
The extensor retinaculum, formed by the aponeurotic expansions of the vastus medialis and vastus lateralis, plays a dual role. Biomechanically, it acts as a secondary extensor; an intact retinaculum may permit active knee extension even in the presence of a completely displaced transverse patellar fracture. Anatomically, it provides crucial medial and lateral stability to the patella. During our surgical approach, the extent of retinacular tearing dictates the degree of fracture displacement. Repairing these retinacular tears is not an afterthought; it is an absolutely mandatory step in restoring the complete functional integrity of the extensor mechanism and preventing postoperative patellar subluxation.
Exhaustive Indications and Contraindications
The decision algorithm for operative versus nonoperative management of patellar fractures is governed by strict, well-established biomechanical and clinical criteria. Nonoperative management is exclusively reserved for fractures that demonstrate an intact extensor mechanism (the patient can independently perform a straight leg raise) and exhibit minimal displacement. Specifically, we tolerate no more than 2 millimeters of articular step-off and less than 3 millimeters of absolute fragment separation. Patients meeting these stringent criteria can be managed in a hinged knee brace locked in extension, with progressive, heavily monitored weight-bearing and range of motion protocols.




Operative intervention, conversely, is indicated for the vast majority of patellar fractures encountered in the acute trauma setting. The primary indications include any disruption of the extensor mechanism, articular displacement exceeding 2 millimeters, fragment separation exceeding 3 millimeters, and all open fractures. Furthermore, fractures with significant comminution that threaten the congruity of the patellofemoral joint require meticulous open reduction and internal fixation (ORIF). The overarching goal of surgery is twofold: absolute anatomic reduction of the articular cartilage to mitigate post-traumatic arthritis, and the creation of a biomechanically stable construct that permits early, aggressive postoperative range of motion.
Contraindications to surgical intervention are rare but must be carefully considered. Absolute contraindications include the presence of an active, untreated infection in the overlying soft tissues (e.g., severe cellulitis or an infected prepatellar bursitis) or a patient whose medical comorbidities render them unfit for anesthesia. Relative contraindications involve severely non-ambulatory patients with profound baseline dementia or paralysis, where the risks of surgery and hardware complications outweigh the functional benefits of restoring the extensor mechanism. In such salvage scenarios, nonoperative management or delayed partial patellectomy may be considered.
Clinical Decision Matrix for Patellar Fractures
| Parameter | Non-Operative Management | Operative Management (ORIF) |
|---|---|---|
| Extensor Mechanism | Intact (Positive Straight Leg Raise) | Disrupted (Inability to extend knee) |
| Articular Step-off | < 2 mm | > 2 mm |
| Fragment Separation | < 3 mm | > 3 mm |
| Fracture Pattern | Non-displaced transverse, vertical | Displaced transverse, stellate, comminuted |
| Soft Tissue Status | Closed, minimal swelling | Open fractures, severe retinacular tearing |
| Patient Baseline | Ambulatory or non-ambulatory | Ambulatory, functional demand present |
When evaluating a patient, we must also consider the specific fracture morphology. While transverse fractures are the classic indication for anterior tension band wiring, vertical fractures may be better served by independent lag screw fixation. Highly comminuted stellate fractures often require a combination of techniques, including cerclage wiring, cannulated screws with tension bands, or modern low-profile mesh plating systems. The surgeon must enter the operating theater with a versatile armamentarium and a comprehensive preoperative plan.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful patellar osteosynthesis. High-quality orthogonal radiographs—specifically, an anteroposterior (AP), true lateral, and a Merchant or skyline view—are non-negotiable. The lateral view is paramount for assessing the degree of fragment separation and the level of the fracture line (proximal pole, mid-substance, or distal pole). The skyline view is critical for evaluating vertical fracture lines and the congruity of the patellofemoral articulation. In cases of severe, high-energy comminution, a non-contrast computed tomography (CT) scan with 3D reconstructions is highly recommended to map out the articular fragments and plan the trajectory of interfragmentary screws.





Patient positioning must facilitate unhindered access to the anterior knee and allow for seamless intraoperative fluoroscopy. The patient is placed supine on a fully radiolucent operating table. A small bump is placed under the ipsilateral hip to internally rotate the leg slightly, bringing the patella to a true anterior-facing zenith. A non-sterile tourniquet is applied to the proximal thigh. Crucial Surgical Pearl: The tourniquet must be applied and inflated only after the knee has been flexed to 90 degrees or more. If the tourniquet is inflated while the knee is in full extension, it will tether the quadriceps muscle belly, effectively preventing the proximal migration necessary to mobilize the superior patellar fragment, rendering reduction exponentially more difficult.
Prophylactic intravenous antibiotics (typically a first-generation cephalosporin) must be administered within 60 minutes prior to skin incision. In the setting of trauma, the administration of tranexamic acid (TXA) should be considered to minimize perioperative blood loss and reduce the risk of postoperative hematoma formation, which can compromise wound healing. The entire limb is prepped and draped free, allowing the surgeon to manipulate the knee through a full range of motion during the procedure to assess the stability of the fixation construct and the tracking of the patella within the femoral trochlea.
Prior to incision, an Examination Under Anesthesia (EUA) is mandatory. The trauma that caused the patellar fracture may have also resulted in occult ligamentous injuries. A thorough assessment of the anterior cruciate ligament (Lachman test), posterior cruciate ligament (posterior drawer), and collateral ligaments (varus/valgus stress) must be documented. Identifying concomitant injuries alters the postoperative rehabilitation protocol and ensures comprehensive management of the traumatized extremity.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to the patella requires a delicate balance between achieving adequate exposure and preserving the tenuous anterior soft tissue envelope. We utilize a midline longitudinal incision, centered directly over the patella, extending from the distal aspect of the quadriceps tendon to the tibial tubercle. While transverse incisions offer a theoretically superior cosmetic outcome, they severely limit extensile exposure, restrict access to the retinacular tears, and complicate future surgical interventions, such as total knee arthroplasty. The longitudinal incision is the undisputed workhorse for patellar trauma.





Dissection is carried sharply down through the subcutaneous tissue to the prepatellar bursa. Full-thickness fasciocutaneous flaps are developed medially and laterally. It is imperative to avoid creating thin skin flaps, as this will inevitably lead to marginal necrosis. Upon entering the fracture site, the surgeon will encounter a dense fracture hematoma. This must be thoroughly evacuated using copious pulsatile lavage and a curette. The fracture edges are meticulously debrided of interposed periosteum, clotted blood, and loose osteochondral fragments that are too small to incorporate into the fixation construct. The joint is thoroughly irrigated, and the femoral trochlea is inspected for associated osteochondral shear injuries.
Reduction of the fracture is achieved by extending the knee to relax the quadriceps and utilizing a combination of pointed reduction forceps (Weber clamps). The clamps are placed at the medial and lateral poles of the patella to compress the transverse fracture. The reduction must be assessed not only on the anterior cortical surface but, more importantly, by directly palpating the posterior articular surface through the medial and lateral retinacular tears. Anatomic congruity of the articular cartilage is the absolute priority. Once provisional reduction is achieved and confirmed via fluoroscopy, we proceed with the tension band wiring technique.







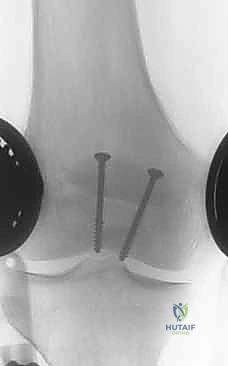
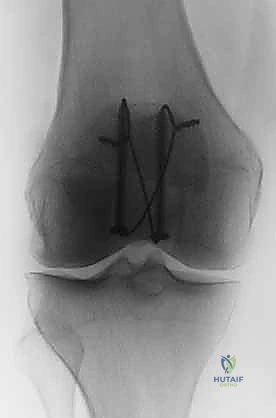
The biomechanical genius of the tension band principle, as described by Pauwels, relies on converting the tensile forces generated by the quadriceps during knee flexion into dynamic compressive forces across the articular surface. To achieve this, two 1.6 mm or 2.0 mm Kirschner wires (K-wires) are driven longitudinally from proximal to distal. They must be perfectly parallel and positioned approximately 5 millimeters deep to the anterior cortex. If placed too posteriorly, they will not effectively act as a tension band; if placed too anteriorly, they risk cutting out of the bone. An 18-gauge stainless steel wire is then passed behind the proximal and distal tips of the K-wires in a figure-of-eight configuration over the anterior surface of the patella.
The wire is tensioned using a double-twist technique to ensure symmetric, uniform compression across the fracture site. The twists are cut short, bent meticulously, and buried deep within the quadriceps and patellar tendon insertions to minimize postoperative hardware prominence. Finally, the K-wires are cut, bent into small hooks, and impacted into the superior pole of the patella to prevent proximal migration. The medial and lateral retinacular tears are then meticulously repaired using heavy, non-absorbable sutures (e.g., #2 FiberWire or Ethibond). The knee is flexed to 90 degrees to confirm stable fixation, absence of fracture gapping, and smooth patellofemoral tracking.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, patellar fracture ORIF is fraught with potential postoperative complications. The most ubiquitous complication is symptomatic hardware prominence. The anterior subcutaneous border of the patella offers virtually no soft tissue padding. Consequently, up to 30% to 50% of patients will experience significant irritation from the K-wire tips or the figure-of-eight wire knots, particularly when kneeling. This frequently necessitates a secondary surgical procedure for hardware removal once radiographic union is confirmed, typically 6 to 12 months postoperatively. Surgeons must prioritize burying hardware deep into the tendinous insertions during the index procedure to mitigate this risk.



Loss of fixation and fracture displacement is a catastrophic complication that occurs in approximately 5% to 10% of cases. This is typically the result of technical errors—such as placing the K-wires too anteriorly, utilizing inadequate wire tension, or failing to repair the retinaculum—combined with patient non-compliance regarding postoperative weight-bearing and flexion restrictions. When catastrophic failure occurs, revision ORIF is technically demanding due to compromised bone stock and altered anatomy. In severe cases of comminution where revision osteosynthesis is impossible, a partial or total patellectomy must be considered as a salvage procedure.
Infection, both superficial and deep, is a devastating complication, particularly prevalent in open fractures or cases with severe soft tissue crushing. The incidence of deep infection ranges from 2% to 5%. Given the intra-articular nature of the fracture, a deep infection rapidly evolves into septic arthritis, threatening the articular cartilage of the entire knee joint. Management requires emergent surgical debridement, copious irrigation, and prolonged intravenous antibiotic therapy. Hardware should be retained if it provides absolute stability; however, loose hardware must be removed.
Incidence of Patellar ORIF Complications
| Complication | Estimated Incidence | Primary Etiology | Salvage / Management Strategy |
|---|---|---|---|
| Symptomatic Hardware | 30% - 50% | Subcutaneous prominence | Hardware removal post-union (6-12 months) |
| Loss of Fixation | 5% - 10% | Technical error, non-compliance | Revision ORIF, Partial Patellectomy |
| Arthrofibrosis/Stiffness | 10% - 20% | Prolonged immobilization | Aggressive PT, Manipulation Under Anesthesia |
| Deep Infection | 2% - 5% | Soft tissue compromise, open injury | Emergent I&D, IV antibiotics, hardware retention if stable |
| Nonunion | 1% - 3% | Poor blood supply, inadequate fixation | Bone grafting, revision fixation |
Post-traumatic osteoarthritis is the long-term nemesis of patellar fractures. Even with perfect anatomic reduction, the initial impact causes irreversible death to chondrocytes (chondronecrosis). Any residual articular step-off greater than 2 millimeters exponentially accelerates this degenerative process. Patients must be counseled preoperatively that while surgery aims to restore mechanics, it cannot reverse the initial cartilaginous injury. Long-term management of post-traumatic patellofemoral arthritis may eventually necessitate patellofemoral arthroplasty or total knee arthroplasty.
Phased Post-Operative Rehabilitation Protocols
The success of patellar ORIF is inextricably linked to the execution of a rigid, phased postoperative rehabilitation protocol. The mechanical stability achieved in the operating room dictates the aggressiveness of the therapy. Assuming a robust tension band construct, our protocol is divided into four distinct phases. Phase I (0 to 2 weeks) focuses on wound healing, edema control, and the prevention of quadriceps inhibition. The patient is placed in a hinged knee brace locked in full extension. Weight-bearing as tolerated (WBAT) is permitted with the brace locked in extension. Patients are instructed to perform frequent ankle pumps, isometric quadriceps sets, and straight leg raises to maintain muscle tone without loading the fracture site dynamically.



Phase II (2 to 6 weeks) initiates controlled, progressive range of motion. The brace is unlocked to allow passive and active-assisted flexion. We typically advance flexion in increments: 0 to 30 degrees for the first few days, progressing to 0 to 60 degrees by week 4, and aiming for 0 to 90 degrees by week 6. Active extension is strictly prohibited during this phase, as the concentric contraction of the quadriceps places maximum tensile stress on the healing fracture. Weight-bearing remains restricted to extension. The physical therapist plays a critical role in mobilizing the patella to prevent peripatellar scarring and subsequent arthrofibrosis.
Phase III (6 to 12 weeks) marks the transition to active extension and weaning from the brace. Radiographic evidence of bridging callus is typically evident by week 6. The brace is gradually unlocked for ambulation, and patients transition to a standard functional knee sleeve. Strengthening exercises shift from isometric to isotonic. Closed kinetic chain exercises, such as mini-squats and leg presses (limited to 0-45 degrees initially), are introduced to rebuild quadriceps strength and endurance safely. Proprioceptive training and stationary cycling are also incorporated to enhance joint mobility and neuromuscular control.
Phase IV (12 weeks and beyond) is the return to full function and sport-specific activities. By this stage, the fracture should be clinically and radiographically united. Patients are cleared for full, unrestricted range of motion and aggressive strengthening, including open kinetic chain exercises and plyometrics. However, patients must be educated that maximal medical improvement, particularly regarding the complete resolution of quadriceps atrophy and the regaining of terminal flexion, may take up to 12 to 18 months. Persistent deficits in deep flexion are common and represent the most frequent functional limitation following this injury.
Summary of Landmark Literature and Clinical Guidelines
The evolution of patellar fracture management is deeply rooted in biomechanical research and rigorous clinical trials. The foundational principles of the tension band wire were established by the AO Foundation (Arbeitsgemeinschaft für Osteosynthesefragen). Their biomechanical studies conclusively demonstrated that an anteriorly placed tension band wire effectively neutralizes the distractive forces of the extensor mechanism, converting them into compressive forces at the articular surface during knee flexion. This principle remains the gold standard against which all novel fixation techniques are measured.

