Recurrent Patellar Dislocation: Pathoanatomy, Biomechanics, and Surgical Management
Key Takeaway
Recurrent patellar dislocation is a complex orthopedic condition driven by both dynamic and static stabilizing failures. Successful management requires a thorough understanding of patellofemoral biomechanics, including the Q-angle, medial patellofemoral ligament (MPFL) integrity, and trochlear morphology. This guide provides an evidence-based approach to evaluating patellar instability, detailing surgical interventions such as MPFL reconstruction and tibial tubercle osteotomy to restore normal extensor mechanism tracking.
Comprehensive Introduction and Patho-Epidemiology
Recurrent dislocation of the patella represents a formidable and highly complex challenge in orthopedic surgery, demanding a nuanced, multi-dimensional understanding of the extensor mechanism's intricate biomechanics. While transient patellofemoral instability can occasionally follow a violent, high-energy initial traumatic dislocation in a structurally normal knee, recurrent instability occurs far more frequently in knees harboring one or more underlying anatomical abnormalities. These structural aberrations—ranging from trochlear dysplasia and patella alta to excessive lateral vector forces—predispose the patellofemoral joint to subluxation or frank dislocation under minimal physiological loads. In these predisposed knees, minor torsional trauma or even simple pivoting maneuvers during activities of daily living are sufficient to precipitate an initial dislocation, setting off a cascade of progressive ligamentous incompetence and cartilaginous degradation.
The epidemiology of patellofemoral instability reveals a distinct predilection for the young, active population, with the highest incidence occurring in adolescents and young adults in their second decade of life. The incidence of primary patellar dislocation in the general population is estimated at 5.8 per 100,000, but this figure skyrockets to 29 per 100,000 in the 10 to 17-year-old demographic. Female patients frequently demonstrate a higher incidence, largely attributed to generalized ligamentous laxity, increased pelvic width resulting in a higher Q-angle, and a greater prevalence of underlying dysplastic features. Following a first-time dislocation, the natural history is deeply concerning; conservative management yields recurrence rates ranging from 15% to 44%. However, once a patient experiences a second dislocation, the statistical probability of subsequent recurrent episodes exceeds 70%, definitively transitioning the pathology from an acute injury to a chronic, habitual instability syndrome.
The patho-epidemiology of recurrent instability is intimately tied to the progressive failure of both static and dynamic restraints. The initial dislocation event almost universally results in the rupture or severe plastic deformation of the medial patellofemoral ligament (MPFL), typically at its femoral origin. If this essential check-rein heals in an elongated, non-isometric position, the patella loses its primary restraint against lateral translation in early flexion. The underlying pathological condition invariably causes an abnormal excursion of the extensor mechanism over the lateral femoral condyle. Consequently, successful management—whether conservative or operative—mandates a comprehensive, granular evaluation of the anatomical factors dictating patellar tracking. Failure to recognize and address the specific pathoanatomical drivers of instability will inevitably lead to surgical failure, recurrent dislocation, and the accelerated onset of severe patellofemoral osteoarthritis.
Furthermore, the economic and psychosocial impact of recurrent patellar dislocation cannot be overstated. Patients often develop profound kinesiophobia, severely limiting their participation in sports and recreational activities. The apprehension associated with impending dislocation alters gait mechanics and proprioceptive feedback, leading to secondary muscular atrophy and generalized lower extremity dysfunction. Therefore, the contemporary orthopedic approach to recurrent patellofemoral instability has shifted away from generalized, non-specific soft-tissue procedures toward a highly individualized, "a la carte" surgical strategy designed to precisely correct the specific anatomical deficits present in each individual patient.
Detailed Surgical Anatomy and Biomechanics
The stability of the patellofemoral joint relies on an intricate, highly calibrated interplay between dynamic muscular forces, static ligamentous restraints, and complex osseous morphology. The extensor mechanism is not merely a simple hinge; it is a dynamic, multi-vector pulley system. Anatomical studies have meticulously delineated the contributions of the various portions of the quadriceps muscle to knee extension and patellar tracking. The muscular vectors are not uniform; rather, they exert multidirectional forces that must remain in strict equilibrium. The Vastus Lateralis (VL) pulls laterally relative to the frontal plane of the femur at an angle of 7 to 10 degrees, representing the primary deforming force in instability. Conversely, the Vastus Medialis Longus (VML) pulls at a 15 to 18-degree medial angle, while the Vastus Medialis Obliquus (VMO) represents the distal, more horizontal fibers, pulling at a critical 50 to 55 degrees medially. The primary function of the VMO is not knee extension, but rather to dynamically stabilize the patella against the lateral pull of the VL. VMO dysplasia or chronic atrophy is a ubiquitous finding in recurrent patellar instability, exacerbating the lateralization vector.
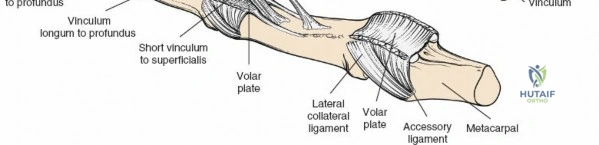
Static factors serve as the primary stabilizers of the patella, particularly in the early degrees of knee flexion (0 to 30 degrees) before the patella fully engages the physical constraint of the trochlear groove. Osseous morphology plays a paramount role; the shape of the patella (classified by Wiberg) and the depth and geometry of the femoral sulcus (trochlea) dictate the inherent bony stability. A normal trochlea provides a deep, constraining groove, whereas trochlear dysplasia—characterized by a shallow, flat, or even convex articular surface—removes this critical osseous barrier. Patellar height is equally critical; patella alta (an abnormally superiorly positioned patella) delays the engagement of the patella into the trochlea during flexion, leaving it entirely reliant on soft-tissue restraints during the most vulnerable arc of motion.
The medial capsuloligamentous complex is the most critical static soft-tissue restraint. The medial knee anatomy is conceptualized in three distinct layers as described by Warren and Marshall. Layer 1 comprises the deep crural fascia. Layer 2 contains the superficial medial collateral ligament (sMCL) and the medial patellofemoral ligament (MPFL). Layer 3 consists of the deep medial capsule. The MPFL is the undisputed primary restraint to lateral patellar translation. Biomechanical studies unequivocally demonstrate that the MPFL provides 50% to 60% of the restraining force against lateral patellar displacement from 0 to 30 degrees of knee flexion. It is an extrasynovial structure, originating from a highly specific footprint nestled in the saddle between the medial epicondyle and the adductor tubercle, and inserting broadly onto the proximal half of the medial patellar border.
Understanding the biomechanical vectors that exacerbate lateral force is paramount for surgical decision-making. The Q-angle (Quadriceps Angle), formed by the intersection of the line of pull of the quadriceps and the patellar tendon, imparts an inherent lateral force vector to the patellofemoral joint as the knee extends. Pathological elevation of the Q-angle exponentially increases the lateral subluxation force on the patella. Drivers of an increased Q-angle include genu valgum, increased femoral anteversion, external tibial torsion, and a laterally positioned tibial tuberosity. The combination of femoral anteversion, genu valgum, and external tibial torsion is classically referred to as "Miserable Malalignment Syndrome." In these patients, the distal attachment of the extensor mechanism is severely lateralized relative to the trochlear groove, a relationship quantified by the Tibial Tubercle-Trochlear Groove (TT-TG) distance. Normalizing these aberrant vectors is the cornerstone of biomechanical restoration in the recurrent dislocator.
Exhaustive Indications and Contraindications
The decision-making algorithm for the surgical management of recurrent patellar dislocation is highly complex and must be tailored to the patient's specific pathoanatomy. Operative intervention is definitively indicated for recurrent instability that has failed a comprehensive, supervised course of conservative rehabilitation. Furthermore, surgical intervention is indicated in the acute setting if there is a displaced osteochondral fracture (typically originating from the medial patellar facet or the lateral femoral condyle as the patella relocates) or a massive structural avulsion of the MPFL that compromises the medial restraints. The modern surgical philosophy dictates an "a la carte" approach, addressing each specific anatomical abnormality identified during the preoperative evaluation. Isolated lateral retinacular release, historically performed for instability, is now considered obsolete and strictly contraindicated for episodic instability without concurrent medial reconstruction, as it predictably exacerbates instability and leads to iatrogenic medial patellar subluxation.
Medial Patellofemoral Ligament (MPFL) reconstruction is the absolute workhorse procedure for restoring medial restraint and is indicated in nearly all cases of recurrent lateral patellar instability. Because MPFL incompetence is the primary driver of recurrent dislocation, reconstructing this ligament is mandatory. However, an isolated MPFL reconstruction is only indicated when the underlying osseous alignment is within acceptable physiological limits. If significant bony malalignment exists, the reconstructed soft-tissue graft will inevitably stretch out and fail over time. Therefore, recognizing the indications for concomitant osseous procedures is critical for long-term success.
Tibial Tubercle Osteotomy (TTO) is indicated when the extensor mechanism vector is pathologically lateralized or when severe patella alta prevents early trochlear engagement. Specifically, an anteromedialization osteotomy (Fulkerson procedure) is indicated when the Tibial Tubercle-Trochlear Groove (TT-TG) distance exceeds 20 mm, or when the Tibial Tubercle-Posterior Cruciate Ligament (TT-PCL) distance is greater than 24 mm. TTO is also indicated for patella alta, defined by a Caton-Deschamps index greater than 1.2, where a distalization vector is added to the osteotomy. Trochleoplasty, a highly specialized and technically demanding procedure, is indicated for severe Dejour Type B, C, or D trochlear dysplasia (characterized by a flat or convex trochlear vault) where soft tissue and distal bony procedures are deemed insufficient to provide stability. Derotational osteotomies of the femur or tibia are reserved for extreme cases of "Miserable Malalignment Syndrome" with femoral anteversion exceeding 30 degrees or severe external tibial torsion.
Contraindications to these procedures must be strictly respected. Skeletal immaturity is an absolute contraindication to any procedure that violates the proximal tibial physis, such as a traditional TTO; in pediatric patients, soft-tissue-only procedures like MPFL reconstruction using physeal-sparing techniques or a Roux-Goldthwait procedure are indicated. Severe, bone-on-bone patellofemoral osteoarthritis is a relative contraindication to joint-preserving instability surgery; in older patients with end-stage arthropathy and instability, patellofemoral arthroplasty or total knee arthroplasty may be the more appropriate definitive intervention.
| Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Isolated MPFL Reconstruction | Recurrent instability, Normal alignment (TT-TG < 20mm), Normal patellar height. | Isolated lateral release, Medial instability, Severe bony malalignment. | Moderate trochlear dysplasia, Mild patellofemoral arthritis. |
| Tibial Tubercle Osteotomy (TTO) | TT-TG > 20mm, Patella Alta (Caton-Deschamps > 1.2), Distal/Lateral PF chondrosis. | Open proximal tibial physis (skeletal immaturity), Active joint infection. | Advanced diffuse PF osteoarthritis, Heavy smoking (non-union risk). |
| Trochleoplasty | Severe Dejour Type B, C, D dysplasia, Convex trochlear vault, Recurrent instability despite TTO/MPFL. | Open distal femoral physis, Diffuse severe patellofemoral arthritis. | Mild dysplasia (Type A), Surgeon inexperience (high complication rate). |
| Derotational Osteotomy | Femoral anteversion > 30°, Severe external tibial torsion, Miserable Malalignment Syndrome. | Skeletal immaturity, Acceptable rotational profile. | Mild rotational malalignment, Poor bone quality. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the foundation of successful patellofemoral stabilization. The process begins with a meticulous physical examination designed to assess both dynamic tracking and static laxity. The examiner must evaluate the "J-Sign," wherein the patella abruptly deviates laterally in the final 10 to 15 degrees of extension, indicating a profound loss of trochlear constraint and MPFL laxity. The Patellar Apprehension Test is performed by applying a laterally directed force to the patella at 20 to 30 degrees of flexion; a positive test elicits severe guarding and patient apprehension. The Lateral Glide Test quantifies medial restraint incompetence; displacement of the patella laterally by more than 2.5 quadrants (relative to the total patellar width) indicates gross MPFL failure. Additionally, the clinician must assess rotational profiles, including the dial test for tibial torsion and prone internal/external rotation for femoral anteversion.
Diagnostic imaging protocols must be exhaustive. Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the site and extent of MPFL injury, assessing for osteochondral fractures, and evaluating cartilage integrity. However, a complete radiographic workup is equally mandatory. Standard radiographs must include an Anteroposterior (AP) view, a True Lateral view (taken at exactly 30 degrees of flexion to accurately assess patella alta via the Insall-Salvati or Caton-Deschamps ratio and to identify trochlear dysplasia via the crossing sign, supratrochlear spur, and double contour sign), and Merchant or Sunrise views to assess dynamic subluxation. Computed Tomography (CT) is essential for calculating the Tibial Tubercle-Trochlear Groove (TT-TG) distance. A TT-TG distance greater than 20 mm is highly pathological. Modern templating also frequently utilizes the TT-PCL distance to eliminate the variable of knee flexion angle during the scan.
Pre-operative templating is particularly critical when a Tibial Tubercle Osteotomy is planned. The surgeon must calculate the exact angle of the osteotomy cut required to achieve the desired ratio of anteriorization (which unloads the patellofemoral joint) to medialization (which corrects the Q-angle). For example, a 45-degree oblique cut will provide equal amounts of anteriorization and medialization, whereas a steeper 60-degree cut will provide more anteriorization than medialization. For MPFL reconstruction, templating involves identifying Schöttle's point on the pre-operative lateral radiograph to anticipate the femoral tunnel trajectory and ensure it does not intersect the intercondylar notch or the posterior femoral cortex.
Patient positioning in the operating room must facilitate both arthroscopic evaluation and open reconstructive procedures. The patient is typically placed supine on the operating table. A high-thigh tourniquet is applied but generally not inflated unless specific visualization issues arise, as tourniquet inflation can tether the quadriceps mechanism and artificially alter patellar tracking during intra-operative assessment. A lateral post or a specialized leg holder is utilized to allow full, unencumbered range of motion from 0 to 120 degrees of flexion. Examination Under Anesthesia (EUA) is performed prior to prepping and draping to confirm the degree of lateral laxity and to establish a baseline for comparison after the reconstruction is complete. A sterile bump may be placed under the knee to maintain 30 degrees of flexion during graft tensioning.
Step-by-Step Surgical Approach and Fixation Technique
Surgical intervention typically begins with a diagnostic arthroscopy. This step is crucial for evaluating the integrity of the patellofemoral articular cartilage, identifying and removing any loose bodies resulting from osteochondral fractures, and dynamically assessing patellar tracking. The arthroscope is introduced through standard anterolateral and anteromedial portals. The surgeon observes the patella as it engages the trochlea during knee flexion. In the recurrent dislocator, the patella will often remain subluxated laterally even at 30 to 40 degrees of flexion. Once the intra-articular pathology is addressed, the open reconstructive phase commences.
For an MPFL Reconstruction, graft selection is the first step. Autografts (typically gracilis or semitendinosus) are most commonly utilized due to their robust biomechanical properties and excellent incorporation rates. Allografts may be considered in revision settings or to minimize donor-site morbidity, though they carry a slightly higher risk of elongation. The graft is harvested, whipstitched at both ends, and sized. The most critical step in MPFL reconstruction is identifying the isometric femoral attachment. Non-anatomic femoral placement is the leading cause of graft failure, postoperative stiffness, and chronic pain. Utilizing strict lateral fluoroscopy, Schöttle's point is identified: 1 mm anterior to the posterior cortical line of the femoral diaphysis, 2.5 mm distal to the posterior origin of the medial femoral condyle, and proximal to the level of the posterior articular margin (Blumensaat’s line). A guide pin is placed at this point, and isometry is checked by looping a suture around the pin and the patella, ensuring less than 2 mm of length change during full range of motion.
Patellar fixation requires meticulous technique. The native MPFL inserts broadly onto the proximal half of the medial patellar border. The graft is typically secured using two suture anchors or via transosseous tunnels in the proximal and middle thirds of the medial patella. A critical surgical pitfall is placing patellar anchors too anteriorly or drilling tunnels too deeply, which creates a massive stress riser that can lead to a catastrophic transverse patellar fracture during postoperative rehabilitation. The graft is passed through layer 2 of the medial knee, deep to the vastus medialis obliquus fascia, ensuring an extrasynovial trajectory. The biomechanics of graft tensioning are paramount. The graft must act as a check-rein, not a medializing force. Tensioning should be performed at exactly 30 degrees of knee flexion. The patella should be able to be displaced laterally by 1 to 2 quadrants with a firm, distinct endpoint. Over-tensioning will lead to severe medial patellofemoral cartilage overload, unremitting pain, and a profound loss of knee flexion.
If a Tibial Tubercle Osteotomy (Fulkerson Anteromedialization) is indicated, a longitudinal incision is made lateral to the tibial crest. The anterior compartment musculature is carefully elevated off the lateral tibia. An oblique osteotomy is performed from anteromedial to posterolateral using an oscillating saw, ensuring the cut exits proximal to the patellar tendon insertion. The tubercle is then translated medially (typically 10 to 15 mm) to normalize the TT-TG distance to approximately 10 to 12 mm, and anteriorly to decompress the joint. The osteotomy is rigidly fixed using two or three 4.5 mm cortical lag screws placed from anterior to posterior, ensuring bicortical purchase. In cases of severe Dejour Type B, C, or D trochlear dysplasia, a sulcus-deepening trochleoplasty may be performed. This involves elevating the articular cartilage of the trochlea as a delicate osteochondral flap, burring a new, anatomically correct V-shaped sulcus in the underlying subchondral bone, and securing the cartilage down into the new groove utilizing resorbable sutures or anchors.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the surgical management of recurrent patellar dislocation carries a distinct complication profile. The surgeon must be acutely aware of these potential pitfalls and possess the technical armamentarium to manage them effectively. Complications can be broadly categorized into structural failures, iatrogenic biomechanical errors, and biological healing issues. The overall complication rate for MPFL reconstruction ranges from 16% to 26%, with the vast majority of these stemming from technical errors rather than biological graft failure. Understanding the etiology of these complications is the first step in prevention.
Patellar fractures are among the most devastating complications following MPFL reconstruction, with an incidence of 1% to 3%. These fractures are almost exclusively iatrogenic, resulting from the creation of stress risers in the patella. Drilling transverse tunnels that are too large in diameter, placing tunnels too close to the anterior cortex, or inserting interference screws that expand the bone excessively can compromise the structural integrity of the patella. When a transverse patellar fracture occurs, it typically requires immediate open reduction and internal fixation (ORIF) with a tension band construct or cannulated screws, significantly delaying rehabilitation and compromising the final outcome.
Recurrent instability remains a significant concern, occurring in 2% to 5% of isolated MPFL reconstructions. The primary driver of recurrent instability is non-anatomic femoral tunnel placement. If the femoral footprint is placed too far anteriorly, the graft will be lax in extension (when the patella is most vulnerable) and excessively tight in flexion. Furthermore, recurrent instability frequently occurs when a surgeon performs an isolated MPFL reconstruction in a patient who actually required a concomitant Tibial Tubercle Osteotomy. Failure to recognize a TT-TG distance greater than 20 mm guarantees that the reconstructed soft-tissue graft will be subjected to overwhelming lateral vector forces, leading to inevitable plastic deformation and eventual rupture. Salvage management in these cases requires a comprehensive revision surgery, often involving a TTO combined with a revision MPFL reconstruction using allograft.
Arthrofibrosis and medial compartment overload represent the opposite end of the complication spectrum, resulting from iatrogenic over-tensioning of the MPFL graft. If the graft is tensioned in full extension or pulled too tightly, it creates a non-physiologic tether that forcefully compresses the medial patellar facet against the medial femoral condyle. This "kissing lesion" phenomenon causes severe, unremitting anterior knee pain and a profound loss of knee flexion. The patient will present with a stiff, painful knee that fails to progress in physical therapy. If recognized early, aggressive physical therapy and dynamic splinting may be attempted. However, refractory cases require arthroscopic release of the medial structures, and occasionally, formal lengthening or release of the MPFL graft.
| Complication | Estimated Incidence | Primary Etiology | Salvage Management / Treatment |
|---|---|---|---|
| Patellar Fracture | 1% - 3% | Deep tunnels, anterior anchor placement, oversized hardware creating stress risers. | ORIF (Tension band wiring or cannulated screws), brace immobilization. |
| Recurrent Instability | 2% - 5% | Non-anatomic femoral tunnel (too anterior), missed osseous malalignment (high TT-TG). | Revision MPFL reconstruction + concomitant TTO or Trochleoplasty. |
| Post-operative Stiffness / Arthrofibrosis | 5% - 10% | Over-tensioning the graft, tensioning in full extension, prolonged immobilization. | Aggressive PT, Arthroscopic lysis of adhesions, possible graft lengthening. |
| Medial Patellofemoral Overload | 3% - 6% | Over-tensioning, creating a medializing force rather than a check-rein. | Arthroscopic release, NSAIDs, revision with graft loosening. |
| TTO Non-union / Delayed Union | 1% - 2% | Poor fixation, smoking, excessive thermal necrosis during osteotomy cut. | Bone grafting, revision internal fixation, prolonged non-weight bearing. |
Phased Post-Operative Rehabilitation Protocols
Successful outcomes in patellofemoral stabilization surgery depend just as heavily on a structured, scientifically phased rehabilitation program as they do on the surgical execution itself. The rehabilitation protocol must carefully balance the biological requirement to protect the healing surgical reconstruction with the mechanical necessity of restoring range of motion and muscular strength. A premature return to aggressive activity can stretch out the MPFL graft or displace a tibial tubercle osteotomy, while overly conservative immobilization will predictably lead to debilitating arthrofibrosis. The protocol is divided into four distinct phases, guided by biological healing timelines and objective functional criteria.
Phase 1 represents the Protection Phase (Weeks 0-2). Immediately post-operatively, the patient is placed in a hinged knee brace locked in full extension. Weight-bearing status depends on the procedure; isolated MPFL reconstructions are typically allowed Weight-Bearing As Tolerated (WBAT) in the locked brace, whereas concomitant TTOs may require partial weight-bearing to protect the osteotomy fixation. The primary goals of this phase are edema control, pain management, and the re-establishment of quadriceps control. Isometric quadriceps sets and straight-leg raises (SLR) are initiated immediately. Crucially, the SLR must be performed without an extension lag; if a lag is present, it indicates profound quadriceps inhibition, and the brace must remain locked. Gentle patellar mobilization is performed to prevent capsular adhesions.
Phase 2 focuses on Early Range of Motion (Weeks 2-6). The hinged brace is unlocked to allow passive and active-assisted Range of Motion (ROM). The biological goal is to provide controlled mechanical stress to the healing graft, promoting collagen alignment along lines of tension without causing plastic deformation. The ROM goals are strictly defined: 0 to 90 degrees of flexion by week 4, progressing to 120 degrees by week 6. Closed-chain kinetic exercises, such as mini-squats and leg presses within a pain-free, protected arc (typically 0 to 45 degrees), are initiated. Open-chain knee extension exercises are strictly avoided during this phase, as they generate maximal shear forces across the patellofemoral joint and place extreme stress on the MPFL graft and TTO site.
Phase 3 is the Strengthening Phase (Weeks 6-12). The hinged brace is discontinued once the patient demonstrates normal, symmetrical gait mechanics and can perform a straight-leg raise without an extension lag. Radiographic evidence of early consolidation is required if a TTO was performed. Rehabilitation shifts toward progressive resistance training, focusing heavily on VMO hypertrophy, gluteal strengthening, and core stability. The "core-to-floor" mechanical linkage is critical; weak hip abductors and external rotators allow the femur to internally rotate beneath the patella, exacerbating functional valgus and lateral patellar tracking. Proprioceptive training using balance boards and unstable surfaces is integrated to restore neuromuscular control.
Phase 4 is the Return to Play Phase (Months 4-6 and beyond). The focus transitions to plyometrics, agility drills, and sport-specific training. The patient must demonstrate confidence in the limb during dynamic, multi-planar movements. Clearance for a return to competitive sports is not time-based; it is strictly criteria-based. The patient must achieve full, painless range of motion, no clinical evidence of effusion, and greater than 90% limb symmetry index (LSI) on functional hop testing (single hop, triple hop, crossover hop). Isokinetic strength testing should demonstrate quadriceps and hamstring strength within 10% of the contralateral, uninjured limb. Premature return to sport before these criteria are met significantly increases the risk of both graft failure and contralateral limb injury.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of recurrent patellar dislocation has undergone a profound evolution over the past three decades, driven by landmark biomechanical studies and paradigm-shifting clinical research. Historically, the treatment of choice was the isolated lateral retinacular release. However, long-term outcome studies definitively proved that this procedure was not only ineffective in restoring stability but frequently resulted in iatrogenic medial subluxation and accelerated osteoarthritis. The modern era of patellofemoral surgery began with the recognition of the MPFL as the primary medial restraint, fundamentally altering the surgical approach.
The identification of the precise anatomical footprint of the MPFL was a watershed moment in orthopedic literature. The seminal work by Schöttle et al. established the radiographic landmarks for the femoral origin of the MPFL. "Schöttle's point" has become the universally accepted standard for femoral tunnel placement, drastically reducing the incidence of non-anatomic reconstructions and subsequent graft failures. Biomechanical studies by Amis and colleagues further refined our understanding, demonstrating the anisotropic properties of the MPFL and its specific contribution to lateral restraint across the entire arc of knee flexion, proving that it acts as a check-rein in early flexion rather than a continuous dynamic stabilizer.
In the realm of osseous malalignment, the contributions of the Lyon school, particularly the work of Henri Dejour and David Dejour, have been foundational. They systematically categorized trochlear dysplasia into four distinct types (A, B, C, and D) based on true lateral radiographs and axial CT imaging. Their research established the threshold of 20 mm for the TT-TG distance as the definitive indication for a tibial tubercle osteotomy, a metric that remains the gold standard in pre-operative templating today. Furthermore, the development of the anter
