Anteromedial Tibial Tubercle Transfer: A Masterclass in Patellofemoral Rebalancing
Key Takeaway
This masterclass details anteromedial tibial tubercle transfer, a powerful procedure for patellofemoral instability and arthritis. We cover comprehensive anatomy, meticulous preoperative planning, and a granular, step-by-step intraoperative execution. Learn precise osteotomy, fixation, and critical techniques to unload the patellofemoral joint, ensuring long-term stability and pain relief. Pearls, pitfalls, and postoperative management are extensively discussed to optimize patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Alright, colleagues and fellows, gather around. Today, we are embarking on a detailed exploration of a complex case involving severe patellofemoral instability coupled with progressive unicompartmental arthritis. Our surgical intervention of choice is the anteromedial tibial tubercle transfer (AMZ), famously pioneered by Dr. John Fulkerson. This is an extraordinarily versatile and powerful procedure, often misunderstood in its biomechanical nuances, yet incredibly effective when meticulously indicated and flawlessly executed. It is imperative to understand that we are not merely moving a block of bone; we are fundamentally rebalancing the entire extensor mechanism, altering contact stress vectors, and restoring the delicate, complex biomechanics of the patellofemoral joint.
The core philosophical and biomechanical concept underlying this procedure is compensation. The patellofemoral joint relies on a fragile interplay of static bony architecture and dynamic soft-tissue restraints. When multiple structural and alignment factors—such as trochlear dysplasia, patella alta, or excessive lateralization of the tibial tubercle—conspire to cause patellar instability or focal chondral overload, a meticulously planned repositioning of the tibial tubercle can mechanically compensate for those underlying anatomical deficiencies. By shifting the force vectors, we provide lasting relief from debilitating pain and instability, often successfully delaying or entirely avoiding the need for more complex, morbid joint resurfacing procedures like patellofemoral arthroplasty down the line.
Epidemiologically, patellofemoral disorders represent one of the most common presentations in orthopedic sports medicine clinics, with a notable preponderance in the young, active female population. This demographic skew is largely attributed to broader pelvic anatomy, resulting in increased Q-angles and functional valgus during dynamic loading. However, the structural anomalies that necessitate a bony transfer—specifically an elevated Tibial Tubercle-Trochlear Groove (TT-TG) distance—are ubiquitous across both sexes in the setting of recurrent dislocations. Chronic lateral tracking inevitably transitions from an episodic instability issue to a chronic degenerative condition, culminating in isolated lateral facet and distal patellar arthrosis.
Understanding the natural history of patellofemoral dysplasia is critical for the orthopedic surgeon. Non-operative management, while the mandatory first line of defense, frequently fails in the presence of gross structural malalignment. Physical therapy can hypertrophy the vastus medialis obliquus (VMO) to enhance dynamic medial pull, but no amount of rehabilitation can medialise a structurally lateralized tibial tubercle or deepen a dysplastic trochlea. When the threshold of structural failure is crossed, characterized by recurrent subluxations, frank dislocations, or the onset of "excessive lateral pressure syndrome," surgical intervention via an anteromedial tibial tubercle transfer becomes the definitive, joint-preserving solution.
Detailed Surgical Anatomy and Biomechanics
Let us begin by rigorously refreshing our understanding of the anterior knee's surgical anatomy and biomechanics. A profound, three-dimensional comprehension of these structures is critical for every single step we take in the operating theater, from the initial incision to the final trajectory of our fixation screws.
Patellofemoral Articulation and Kinematics
The patella, the largest sesamoid bone in the human body, functions primarily as a biomechanical fulcrum to increase the moment arm of the quadriceps muscle group. It articulates within the femoral trochlea, a complex groove with highly specific topographical variations. Normally, as the knee transitions from terminal extension into early flexion, the distal aspect of the patella enters the trochlea from a slightly lateralized and superior position. This entry, or "engagement," should be prompt and smooth, typically occurring within the first 10 to 15 degrees of knee flexion.
As knee flexion progresses, the kinematic contact point on the patellar articular surface shifts proximally. In full, deep flexion, the compressive load is borne almost entirely on the proximal aspect of the patella, with a gradual, predictable transfer of load along the patellar articular cartilage with each successive degree of flexion. This migrating contact area is crucial for distributing the massive compressive forces generated during activities like stair climbing or squatting, which can exceed seven times body weight.
The trochlea itself deepens anatomically with increasing knee flexion, significantly enhancing bony patellar containment. Consequently, the point of greatest vulnerability and instability is predictably in early flexion (0 to 30 degrees), where the trochlea is at its shallowest and the patella relies most heavily on soft-tissue restraints. Any delay in patellar engagement due to patella alta, or any lateralization vector pulling the patella out of this shallow groove, drastically increases the risk of dislocation.
The Extensor Mechanism and Retinacular Structures
The patella is intimately enveloped by a highly complex, multi-layered soft tissue envelope comprising tendinous and retinacular structures, all of which must be evaluated during our surgical planning.
Distally, the patellar tendon connects the inferior pole of the patella to the tibial tubercle. This structure is incredibly robust, yet its vector is entirely dependent on the anatomical position of the tibial tubercle. Proximally, the quadriceps tendon is a massive, multi-layered structure connecting the patella to the four distinct muscles of the quadriceps group. The vastus lateralis (VL) tendon component exerts a significant lateral and proximal pull on the superolateral aspect of the patella, which must be counterbalanced by medial structures.
The Medial Patellofemoral Ligament (MPFL) is the primary static medial stabilizer of the patella, particularly in early flexion (0-30 degrees), contributing over 50% of the resistance to lateral patellar translation. Extending from the proximal half of the medial patella to the saddle region between the adductor tubercle and the medial epicondyle (Schöttle's point), it is almost universally torn, attenuated, or plastically deformed in cases of frank patellar dislocation. Conversely, the lateral retinaculum, which extends to the iliotibial band and features epicondylopatellar and patellotibial components, often becomes pathologically contracted in chronic lateral tracking scenarios, acting as a tether that prevents centralization.
Bony Landmarks and Malalignment Indices
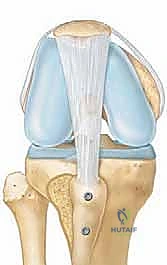
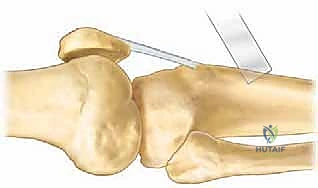
In our preoperative and intraoperative assessments, we rely heavily on objective, quantifiable malalignment indices, most notably the tibial tuberosity to trochlear groove (TT-TG) index. This measurement, derived from superimposed axial computed tomography (CT) or magnetic resonance imaging (MRI) slices, precisely quantifies the lateralization of the tibial tubercle relative to the deepest point of the central trochlear groove.
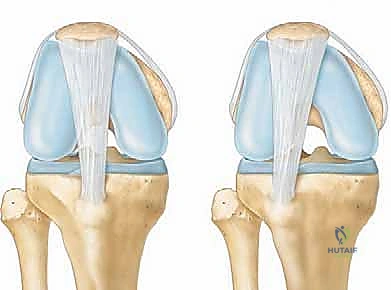
FIG 1 • The relation of the tibial tubercle (TT) to the central trochlear groove (TG)—the TT-TG relationship— pertains to patella instability. A. Normal TT-TG relationship, in which the tibial tubercle and trochlear groove are lined up. B. Lateralized tibial tubercle.
A normal TT-TG distance is generally considered to be less than 15 mm. A measurement between 15 mm and 20 mm is considered borderline and must be correlated with clinical symptoms, while a TT-TG index exceeding 20 mm is universally recognized as pathologically abnormal and serves as a strong, primary indicator for surgical bony correction. A high TT-TG signifies that the distal anchor of the extensor mechanism is pulling the patella laterally out of the groove with every quadriceps contraction. Similarly, a high clinical Q-angle (typically >20 degrees in females, >15 degrees in males) points to a macroscopic imbalance in the extensor mechanism, though the TT-TG is a far more reliable, radiographically reproducible metric.
Pathogenesis of Patellofemoral Disorders
The clinical manifestations of patellofemoral disorders almost always stem from a synergistic combination of anterior knee dysplasia, structural malalignment, and cumulative micro-trauma. Chronic lateral tracking of the patella, driven by an elevated TT-TG or an incompetent MPFL, leads to asymmetric joint overload and exponentially increased point loading, particularly on the lateral facet of the patella and the lateral trochlear ridge.
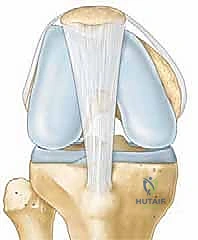
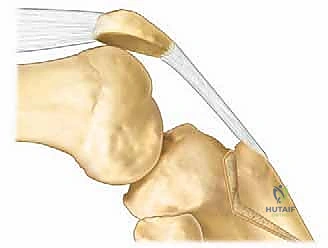
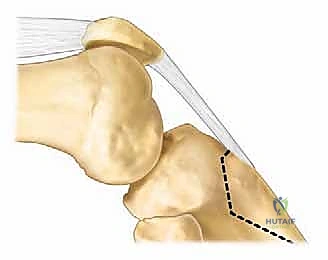
FIG 2 • A. Normal trochlear groove.
This chronic, repetitive overload eventually precipitates subchondral sclerosis and articular cartilage breakdown, a pathological cascade that Ficat famously termed the "excessive lateral pressure syndrome." Over time, a chronically lateralized extensor mechanism can lead to developmental, macroscopic flattening of the lateral trochlea and the patella itself, creating a vicious cycle that perpetuates further instability and accelerates arthritic degeneration.
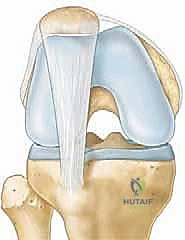
FIG 2 • B. With prolonged lateral patella tracking, the lateral trochlea becomes flattened, further aggravating lateral patella instability and stretching the medial patella support structure.
Furthermore, a traumatic dislocation event typically tears the MPFL. Even if this ligament heals non-operatively, it frequently heals in an elongated, functionally incompetent state, permanently reducing the threshold for subsequent dislocations. In cases of blunt trauma to the flexed knee, the injury often localizes to the proximal patella, with deep, aching pain originating from the contused subchondral bone, as the overlying articular cartilage is entirely aneural.
Neurovascular Considerations
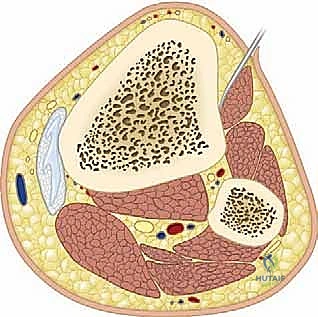
As we approach the proximal tibia and the tibial tubercle, we must remain acutely vigilant regarding the regional neurovascular anatomy. The most immediate threat during our surgical approach is the infrapatellar branch of the saphenous nerve (IPBSN). This purely sensory nerve typically crosses the surgical field anteromedially, coursing from medial to lateral, often 2 to 3 cm distal to the inferior pole of the patella. It is highly variable in its arborization but is extremely susceptible to iatrogenic transection or traction injury during the initial incision and subcutaneous dissection. Injury to the IPBSN can lead to a highly symptomatic, recalcitrant neuroma or a bothersome area of chronic numbness over the anterior knee, leading to significant patient dissatisfaction despite a mechanically successful surgery.
Deeper and more central lies the anterior tibial artery and vein complex. While these structures are protected by the interosseous membrane and the posterior musculature, extreme caution must be exercised when passing drills, placing retractors, or driving bicortical fixation screws through the posterior cortex of the tibia. Over-penetration of the posterior cortex with a drill bit can result in catastrophic vascular injury. Additionally, while the superficial peroneal nerve is typically located further laterally, excessive lateral subperiosteal dissection or overly aggressive lateral retractor placement should be strictly avoided to prevent neuropraxia.
Exhaustive Indications and Contraindications
Patient selection is the absolute bedrock of a successful outcome in tibial tubercle osteotomies. Performing this procedure on the wrong patient, or for the wrong reasons, will inevitably lead to failure, continued pain, or iatrogenic complications. The anteromedial transfer is specifically designed to address structural alignment imbalances and articular overload that have culminated in instability, pain, or both.
The decision to proceed with surgery must be based on a comprehensive synthesis of the patient's history, physical examination, and advanced imaging metrics. We must confirm that the patient's symptoms are directly attributable to the mechanical malalignment we intend to correct.
| Category | Specific Criteria | Clinical Rationale |
|---|---|---|
| Indications | TT-TG Distance > 20 mm | Pathologic lateralization of the extensor mechanism vector, necessitating bony medialization. |
| Recurrent Patellar Instability | Failure of soft tissue restraints (e.g., MPFL) secondary to overwhelming bony malalignment. | |
| Distal/Lateral Patellofemoral Arthrosis | Focal chondral disease that can be mechanically unloaded by anteriorizing (elevating) and medializing the tubercle. | |
| Failed Soft Tissue Reconstruction | Previous MPFL reconstruction failure due to unrecognized or unaddressed bony malalignment (high TT-TG). | |
| Patella Alta (Caton-Deschamps > 1.2) | Can be addressed concurrently by distalizing the tubercle during the transfer, improving early trochlear engagement. | |
| Contraindications | Proximal/Medial Patellofemoral Arthrosis | Anteromedial transfer will increase contact pressures on the medial facet, exacerbating symptoms in this specific compartment. |
| Open Physes (Skeletal Immaturity) | Absolute contraindication. Osteotomy risks catastrophic growth arrest, recurvatum deformity, or premature physeal closure. | |
| Active Knee Joint Infection | Standard absolute contraindication for elective orthopedic hardware implantation. | |
| Severe Inflammatory Arthropathy | Rheumatoid arthritis or similar conditions where soft tissue integrity and bone quality are severely compromised. | |
| Inability to Comply with Rehab | The procedure requires strict postoperative weight-bearing and ROM restrictions to prevent catastrophic osteotomy failure. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough, obsessive preoperative planning is what separates a master surgeon from a technician. In the context of an anteromedial tibial tubercle transfer, precise templating dictates the exact geometry of our osteotomy, ensuring we achieve the desired biomechanical outcome without creating new iatrogenic pathologies.
Imaging Modalities and Diagnostic Studies
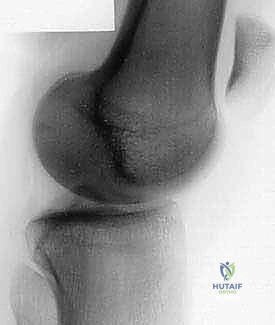
Our surgical planning relies heavily on a standardized, high-quality imaging protocol. Standardized office radiographs are our first line of investigation. A true lateral view, taken standing at precisely 30 degrees of knee flexion with the posterior femoral condyles perfectly superimposed, is mandatory. This view provides crucial information regarding trochlear depth, the presence of a supratrochlear spur, and the assessment of patellar height (alta or baja) using the Caton-Deschamps or Insall-Salvati ratios.

Pre-operative imaging demonstrating lateral patellar tilt and early arthritic changes.
The axial view (Merchant or Laurin view), taken with the knee flexed exactly to 30 degrees, is critical for assessing dynamic patellar tilt and lateral subluxation. Many patients present with standard 90-degree flexion skyline views, which are essentially useless for diagnosing early flexion instability, as the patella is already deeply seated in the trochlea at that angle.
A Computed Tomography (CT) scan is absolutely indispensable for accurately measuring the TT-TG index and assessing trochlear dysplasia (Dejour classification). The CT protocol should dynamically assess how the patella enters the trochlea, ideally obtaining mid-patella transverse images at 0, 15, 30, and 45 degrees of flexion. Magnetic Resonance Imaging (MRI) is less useful for pure bony alignment but is the gold standard for evaluating the integrity of the articular cartilage (grading chondromalacia), assessing the MPFL, and identifying subchondral bone marrow edema patterns indicative of focal overload.
Surgical Templating and Biomechanical Goals
The primary goal of the anteromedial transfer is to accomplish two critical biomechanical objectives simultaneously. First, Medialization: By shifting the tubercle medially, we rebalance the patella into the central trochlear groove, decreasing the lateral vector force and unloading the lateral facet. Second, Anteriorization: By elevating the tubercle anteriorly, we increase the moment arm of the extensor mechanism, thereby decreasing the overall joint reaction force and specifically unloading the distal and lateral articular surfaces of the patella, which are frequently degenerated in these patients.
Pre-operative templating and marking of the planned osteotomy.
We must template the exact amount of medialization and anteriorization required. The beauty of the Fulkerson osteotomy lies in its geometry: the angle or slope of the osteotomy cut in the axial plane dictates the proportional ratio of anteriorization to medialization. A steep cut (e.g., 60 degrees relative to the coronal plane) will result in massive anteriorization with minimal medialization. A shallower cut (e.g., 30 degrees) will yield significant medialization with modest anteriorization. Our typical goal is to normalize the TT-TG index to approximately 9 to 12 mm, while achieving 10 to 15 mm of anterior elevation to adequately unload the degenerated facets.
Patient Positioning and Operating Room Setup
Proper patient positioning is critical for intraoperative fluoroscopy and dynamic assessment. The patient is placed in the supine position on a standard operating table. A pneumatic tourniquet is applied high on the proximal thigh to ensure a bloodless field, though it is often inflated only after exsanguination if visualization becomes compromised.
We utilize a standard leg holder or a lateral post to allow for full, unencumbered knee flexion and extension intraoperatively. This is vital for assessing patellar tracking after provisional fixation. The foot of the bed is dropped to allow the knee to hang at 90 degrees of flexion when needed. The fluoroscopy C-arm must be positioned on the contralateral side, draped sterilely, and its trajectory confirmed prior to prepping to ensure we can obtain perfect true lateral and axial patellofemoral views without needing to awkwardly reposition the patient mid-surgery.
Step-by-Step Surgical Approach and Fixation Technique
Let us now transition to the surgical execution. Meticulous soft tissue handling, precise bone cuts, and rigid internal fixation are the hallmarks of a successful anteromedial tibial tubercle transfer.
Incision and Initial Dissection
We begin with a longitudinal anteromedial incision, approximately 8 to 10 cm in length, centered precisely over the tibial tubercle. I prefer to initiate the incision just distal to the patellar apex and extend it distally, slightly medial to the tibial crest. This trajectory provides excellent, expansile exposure for the osteotomy and allows for a concurrent lateral retinacular release or MPFL reconstruction if dictated by our preoperative plan.

Initial surgical exposure demonstrating the patellar tendon and tibial tubercle.
Upon incising the skin and subcutaneous tissue, we must immediately shift our focus to identifying and protecting the infrapatellar branch of the saphenous nerve (IPBSN). Using careful blunt dissection with Metzenbaum scissors, we sweep the subcutaneous fat to locate the nerve branches. Once identified, the nerve is gently mobilized and retracted, typically medially, away from the planned osteotomy site.
We then incise the deep fascia longitudinally, just medial to the patellar tendon, exposing the tendon itself and the underlying anterior periosteum of the proximal tibia. We must clearly define the medial and lateral borders of the patellar tendon insertion onto the tubercle. A Cobb elevator is used to meticulously elevate the anterior compartment musculature off the lateral aspect of the tibia, creating a safe zone for our saw blade and retractors.
Defining the Osteotomy and Preparing the Tubercle
With the anatomy clearly defined, we proceed to mark the osteotomy. The dimensions of the bone block are critical: it must be robust enough to withstand the pull of the quadriceps and accept internal fixation without fracturing. Typically, we aim for a block that is 1.5 to 2 cm wide, 4 to 6 cm long, and at least 1 cm thick at its proximal aspect, tapering distally.
We use an electrocautery or a sterile marking pen to outline the planned cuts. The proximal cut is initiated just proximal to the patellar tendon insertion, ensuring the entire footprint is captured within the bone block. The medial cut runs parallel to the sagittal plane of the tibia, while the lateral cut is angled slightly to converge with the medial cut distally. Crucially, we aim to keep the distal periosteal attachment of the bone block intact. This "distal hinge" preserves the tenuous blood supply to the tubercle, drastically enhancing the rate of bony union, and acts as a mechanical tether to prevent catastrophic proximal migration of the tubercle under quadriceps tension.
Executing the Anteromedial Transfer
Before introducing the saw, we place wide, protective retractors (such as Z-retractors or Hohmanns) subperiosteally on the lateral aspect of the tibia to definitively protect the anterior tibial neurovascular bundle from the oscillating blade.
Executing the precise, angled osteotomy using an oscillating saw.
Using a sharp, wide oscillating saw blade, we begin the osteotomy. The angle of the saw blade relative to the anterior cortex of the tibia is the most critical step of the procedure, as this slope dictates the magnitude of our anteromedial vector. For a standard Fulkerson transfer, the saw blade is typically angled from anteromedial to posterolateral. Copious cold saline irrigation is continuously applied to the blade by the assistant to prevent thermal necrosis of the bone, which can lead to delayed union or nonunion.
We complete the proximal, medial, and lateral cuts with the saw, but we stop short of completing the distal cut. We then transition to broad, sharp osteotomes. The osteotomes are gently advanced to complete the deep portion of the cut and to carefully pry the bone block anteriorly and medially, pivoting on the intact distal periosteal hinge.
Shifting the tibial tubercle bone block anteromedially.
Once the block is mobilized, we shift it along the sloped osteotomy bed to our pre-templated position. The block will naturally translate anteriorly and medially. We provisionally hold the block in its new, corrected position using two heavy, smooth Kirschner wires (K-wires) driven from anterior to posterior.
Rigid Internal Fixation and Intraoperative Assessment
With the tubercle provisionally pinned, we must dynamically assess patellar tracking. The tourniquet is deflated if it was used, and the knee is taken through a full, slow range of motion from 0 to 120 degrees of flexion. We directly observe the patella entering the trochlea. It should engage centrally and smoothly without any lateral subluxation or excessive tilt. If tracking remains suboptimal, the K-wires are removed, the block is repositioned, and the tracking is reassessed until perfect biomechanics are achieved.
Preparation for rigid internal fixation of the transferred tubercle.
Once satisfied, we proceed with rigid internal fixation. We typically utilize two 4.5 mm fully threaded cortical screws, or partially threaded cancellous screws if the bone is particularly soft. The screws are placed using standard lag technique to achieve dynamic compression across the osteotomy site. The proximal screw is placed first, directed slightly proximally and laterally to engage the dense posterior cortical bone of the tibia. The distal screw is placed parallel to the first. Washers are routinely used to prevent the screw heads from burying into the anterior cortex of the transferred block, which can cause a stress riser and subsequent fracture.
Final rigid internal fixation achieved with two lag screws and washers.
After final tightening, fluoroscopy is utilized to confirm perfect hardware placement. We must ensure the screws are of appropriate length—achieving bicortical purchase without excessive posterior protrusion that could endanger the neurovascular structures. The osteotomy site is thoroughly irrigated, and the deep fascia, subcutaneous tissue, and skin are meticulously closed in layers.
Post-operative AP radiograph confirming medialization and hardware placement.
Post-operative Lateral radiograph confirming anteriorization and bicortical screw purchase.
Complications, Incidence Rates, and Salvage Management
While the anteromedial tibial tubercle transfer is highly effective, it is a technically demanding procedure associated with a specific, well-documented complication profile. Recognizing these potential pitfalls and knowing how to manage them is paramount for the operating surgeon. The most devastating complication is a fracture of the proximal tibia, which typically occurs if the osteotomy cut is made too deeply (violating the posterior cortex) or if the proximal cut creates a sharp stress riser.
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| Proximal Tibia Fracture | 1% - 3% | Prevention: Avoid undercutting the proximal tibia; taper the distal cut; avoid over-tightening screws in osteopenic bone. Salvage: Open reduction and internal fixation (ORIF) with a lateral locking plate; prolonged non-weight bearing. |
| Delayed Union / Nonunion | 2% - 5% | Prevention: Copious irrigation during sawing to prevent thermal necrosis; preserve distal periosteal hinge; rigid lag screw fixation. Salvage: Bone grafting (autograft or allograft) and revision internal fixation; use of bone stimulators. |
| Symptomatic Hardware | 10% - 20% | Prevention: Countersink screw heads slightly if possible; avoid excessively prominent washers; place incision slightly off-axis from hardware |
