Masterclass in Operative Orthopaedics: Muscle and Tendon Ruptures
Key Takeaway
Muscle and tendon ruptures frequently result from eccentric overload, particularly in two-joint muscles with high proportions of type II fast-twitch fibers. The Achilles tendon is highly susceptible due to a hypovascular watershed zone 2 to 6 cm proximal to its calcaneal insertion. Surgical repair is indicated for active patients to minimize rerupture rates. This guide details the biomechanics, clinical evaluation, open and minimally invasive surgical techniques, and evidence-based postoperative rehabilitation protocols for optimal functional recovery.
RUPTURE OF MUSCLES AND TENDONS: PATHOPHYSIOLOGY AND BIOMECHANICS
Injuries to the muscle-tendon unit represent a significant proportion of the pathology managed by orthopaedic surgeons. Understanding the biomechanical failure of these structures is paramount for accurate diagnosis and effective surgical reconstruction. According to Gilcreest, the most frequent cause of partial or complete rupture of a muscle or tendon is the eccentric overload of the muscle-tendon unit.
Mechanisms of Injury and Muscle Strain
Muscle strain is strictly defined as an indirect injury to a muscle, producing tension overload in a passive muscle or, more commonly, eccentric overload in an actively contracting muscle. Other mechanisms of injury include a direct blow by a sharp edge on an actively contracted muscle, or open lacerations.
McMaster first demonstrated that a normal, healthy muscle-tendon unit consistently fails at the musculotendinous junction when strained to failure. Subsequent experimental data provided by Almenkinders, Garrett, and Seaber showed that under passive overload or eccentric overload at varying rates of strain, failure invariably occurs at the distal myotendinous junction.
Biomechanics Pearl: Electrically stimulated muscle producing an eccentric contraction absorbs twice as much energy before failure in stretch compared to a passively overloaded muscle.
Strains most commonly occur in:
* Muscles that cross two joints (e.g., hamstrings, rectus femoris, gastrocnemius).
* Muscles with a higher percentage of type II fast-twitch muscle fibers.
* The weaker muscle of an agonist-antagonist muscle group.
Fatigue is a critical contributing factor to muscle overload, rendering the muscle unable to absorb maximal eccentric force. Intrinsic tightness further exacerbates this risk. Initial management of muscle strains relies on cryotherapy, rest, and anti-inflammatory medication, progressing to gentle stretching and strengthening. Failure to regain full flexibility and normal strength significantly increases the risk of recurrent injury.
Principles of Muscle Laceration Repair
When a functionally important muscle is disrupted or lacerated—especially in a vigorous young patient or manual laborer—early surgical repair is indicated.
- Debridement: The torn ends must be meticulously debrided to appose healthy, viable muscle tissue.
- Suturing: Interrupted, nonabsorbable mattress sutures are placed circumferentially, incorporating the epimysium (muscle sheath) to provide structural hold.
- Reinforcement: The repair is reinforced with deep mattress sutures of fascia lata or large nonabsorbable tension sutures placed in line with the physiological tension vectors.
Garrett et al. demonstrated that following the repair of a lacerated muscle, dense connective tissue predominates at the repair site, with scattered areas of muscle regeneration. Distal muscle fibrils generally exhibit characteristics of denervation. After complete laceration, muscle power returns to approximately 50%, and contractility to 66% of an uninjured muscle. Incompletely severed muscles demonstrate significantly better functional return.
Tendon Rupture Dynamics and Systemic Risk Factors
Tendon ruptures occur more frequently in middle-aged and elderly populations. Intrinsic weakness resulting from repetitive microtrauma and incomplete healing in "watershed" areas of precarious vascularity predisposes certain tendons to rupture—most notably the supraspinatus, biceps brachii, and Achilles tendons.
Systemic conditions that compromise collagen integrity and weaken tendons include:
* Rheumatoid arthritis and Systemic Lupus Erythematosus (SLE)
* Hyperparathyroidism and Renal failure
* Hyperbetalipoproteinemia (xanthoma)
* Hemangioendothelioma
* Systemic or local corticosteroid administration (a major iatrogenic risk factor)

ACHILLES TENDON INJURIES: COMPREHENSIVE MANAGEMENT
Etiology and Pathophysiology
Achilles tendon injuries are highly prevalent among middle-aged athletes ("weekend warriors"). Tendinitis, tendinosis, and peritendinitis account for up to 11% of lower extremity complaints in runners, and Achilles tendon ruptures are estimated to be the third most frequent tendon rupture overall.
The classic mechanisms of Achilles tendon rupture include:
1. Pushing off with the weight-bearing forefoot while extending the knee (e.g., sprinting, jumping).
2. Sudden, unexpected dorsiflexion of the ankle (e.g., slipping into a hole).
3. Violent dorsiflexion of a plantar-flexed foot (e.g., falling from a height).
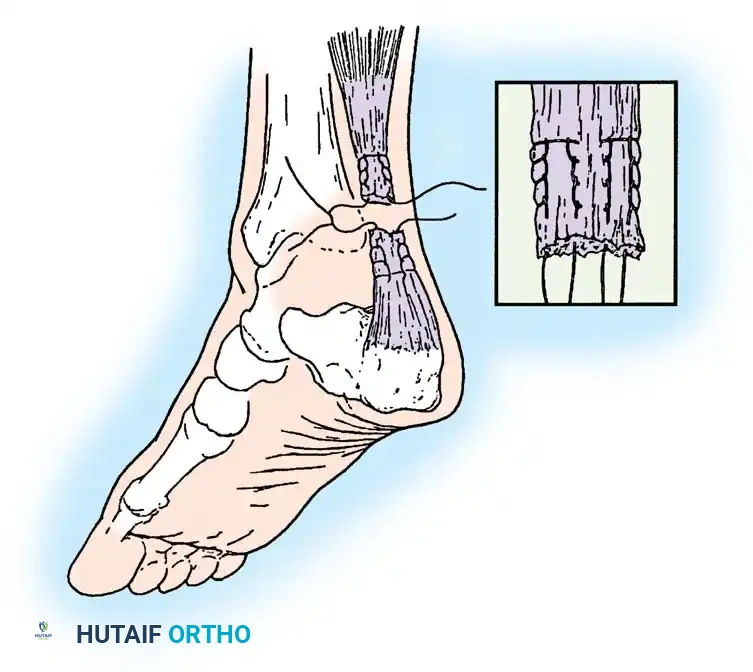
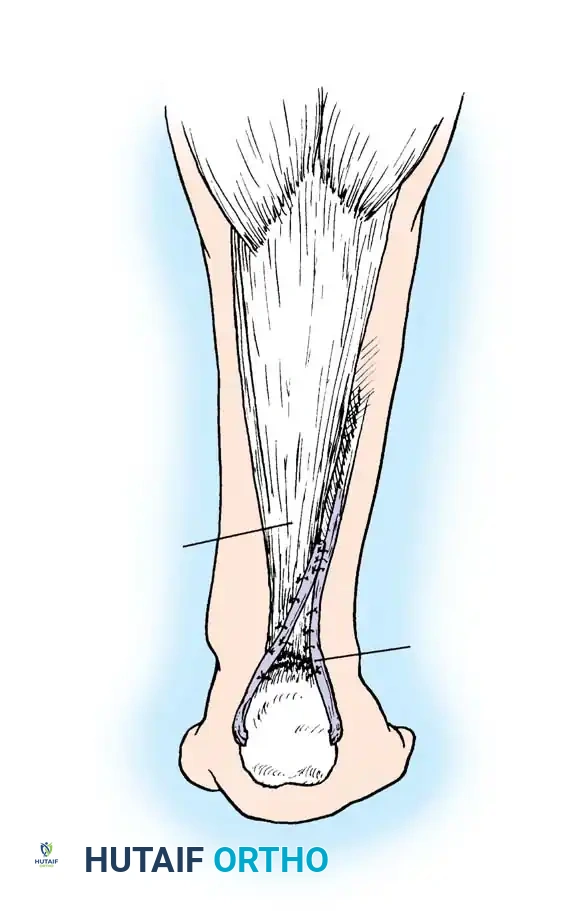
The Watershed Zone: Angiographic studies demonstrate a relatively hypovascular zone 2 to 6 cm proximal to the tendon's insertion into the calcaneus. The primary blood supply arrives via the anterior mesentery of the mesotendon, which diminishes with age.
Age-dependent changes in collagen cross-linking increase stiffness and reduce viscoelasticity. Repetitive microtrauma outpaces the tendon's reparative capacity in this hypovascular zone, leading to degenerative attrition. A final mechanical eccentric overload completes the rupture.
Clinical Evaluation and Diagnosis
Diagnosis of an acute Achilles tendon rupture is primarily clinical. Imaging (ultrasound or MRI) is usually reserved for equivocal cases or chronic presentations.
- Palpable Defect: A distinct gap is usually palpable 2 to 6 cm proximal to the calcaneal insertion.
- Loss of Function: The patient exhibits an inability to perform a single-leg toe-raise on the affected side.
- Thompson "Squeeze" Test: With the patient prone, squeezing the calf muscle just distal to its maximal girth should normally elicit passive plantar flexion. The test is positive for complete rupture if plantar flexion is absent.
- O’Brien Needle Test: A 25-gauge needle is inserted percutaneously into the midline of the proximal tendon. If the tendon is intact, passive range of motion of the foot will cause the needle hub to tilt.
Evidence-Based Treatment Controversies: Operative vs. Nonoperative
The literature regarding the optimal management of Achilles tendon ruptures remains highly debated.
Historically, Lea and Smith, as well as Nistor, advocated for conservative treatment, citing similar outcomes in range of motion and strength. However, Inglis, Sculco, Beskin, and Jacobs strongly recommended surgical repair in athletic individuals due to a significantly lower rerupture rate (2% to 3% operative vs. 10% to 30% nonoperative).
Recent meta-analyses provide clearer guidance:
* Kocher et al.: Rerupture probability was 12% (nonoperative) vs. 2% (operative). However, moderate complications (e.g., infection) were higher in the operative group (7.5% vs. 0.3%).
* Bhandari et al. & Khan et al.: Confirmed lower rerupture risks with surgery but higher complication rates. Khan noted fewer complications with percutaneous repair and functional bracing compared to traditional casting.
* Amendola et al.: Reported rerupture rates of 21% (nonoperative) vs. 2% (operative).
* Pajala et al.: In 409 operative patients, deep infection occurred in 2.2%. Risk factors included older age, corticosteroid use, and delayed treatment.
Surgical Warning: While operative treatment maximizes strength and minimizes rerupture, meticulous soft-tissue handling is mandatory to prevent devastating wound complications and deep infections.

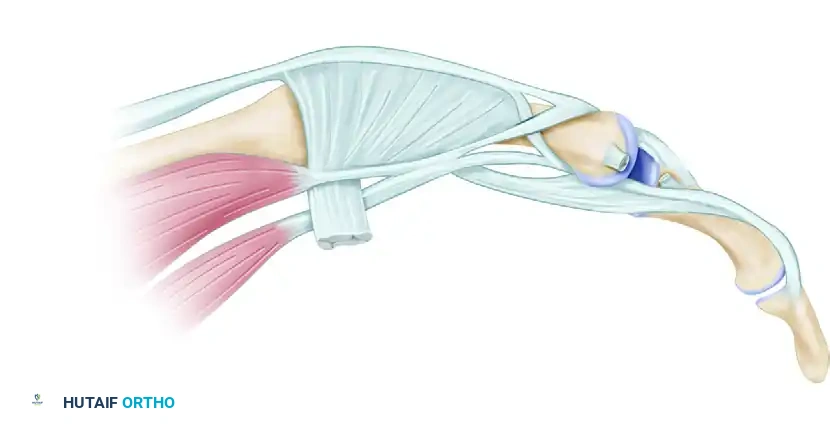
SURGICAL ANATOMY AND PREOPERATIVE PLANNING
Positioning and Preparation
The patient is placed in the prone position. Bilateral lower extremities should be prepped and draped to allow intraoperative comparison of resting equinus tension. A thigh tourniquet is applied.
OPEN SURGICAL REPAIR OF ACHILLES TENDON RUPTURE (TECHNIQUE 46-6)
The open technique allows for direct visualization, debridement of degenerative tissue, and robust end-to-end anastomosis, often augmented with local tissue.
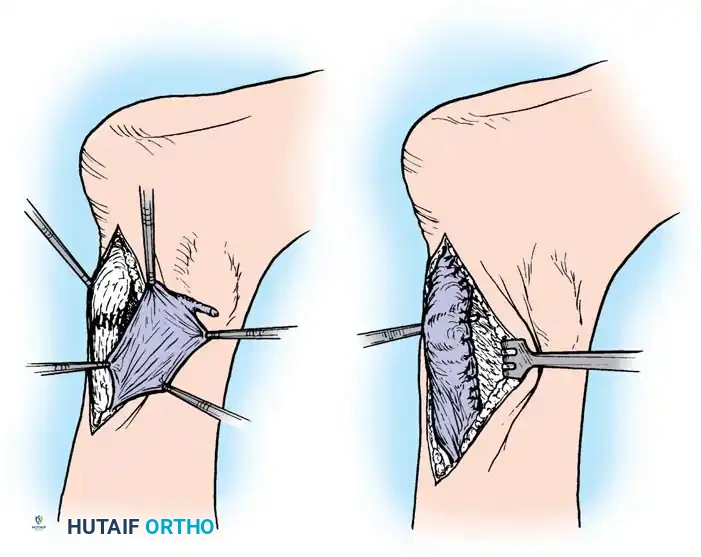
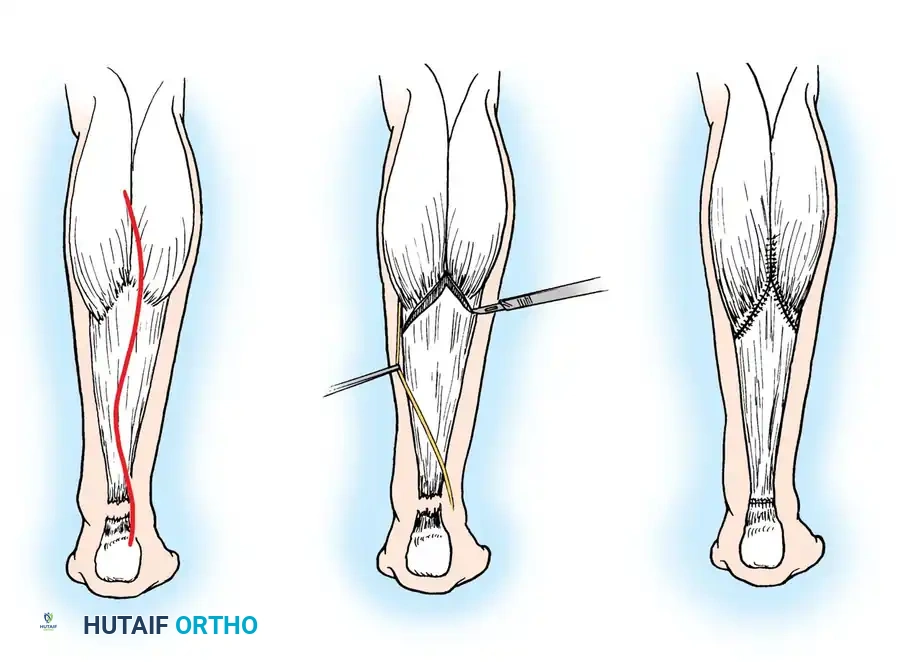
Step 1: Surgical Approach and Dissection
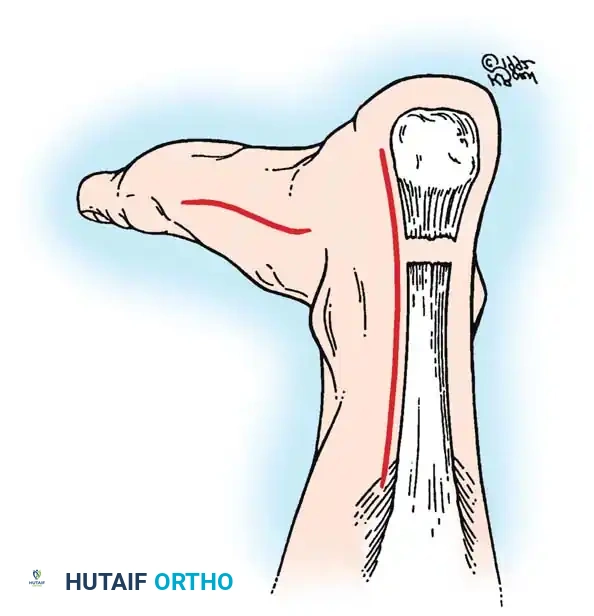
- Make a posteromedial longitudinal incision, 10 to 15 cm in length.
- Crucial Detail: Place the incision approximately 1 cm medial to the palpable medial border of the tendon. End it just proximal to where the shoe counter strikes the heel. A midline incision must be avoided to prevent postoperative shoe irritation and delayed wound healing.
- Carry the incision sharply through the skin and subcutaneous tissues directly down to the paratenon (tendon sheath).
- Reflect the paratenon together with the subcutaneous tissue as a single full-thickness flap. Minimize subcutaneous undermining to preserve the fragile vascular supply to the skin edges.
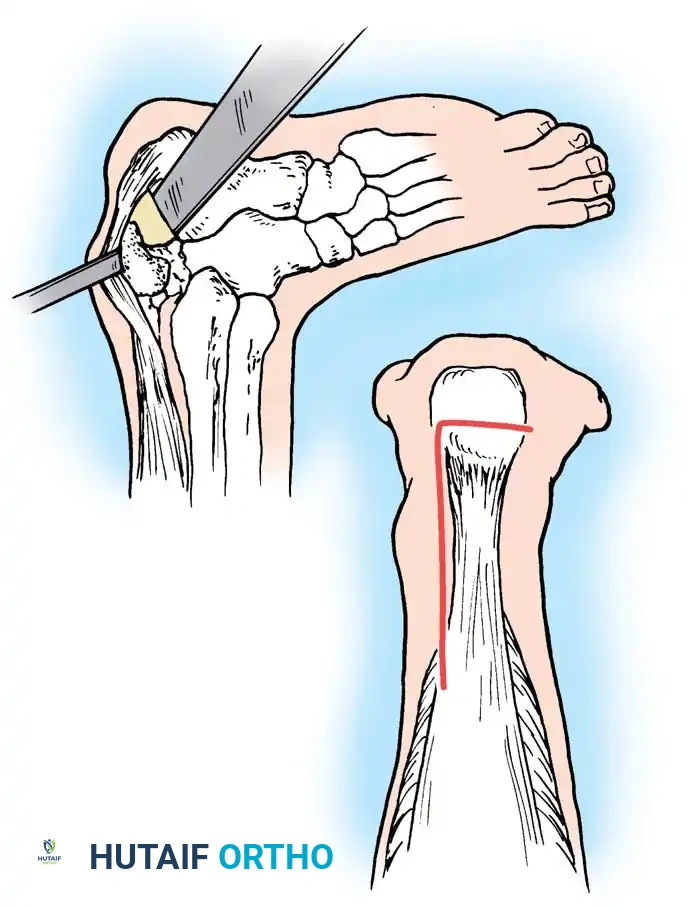
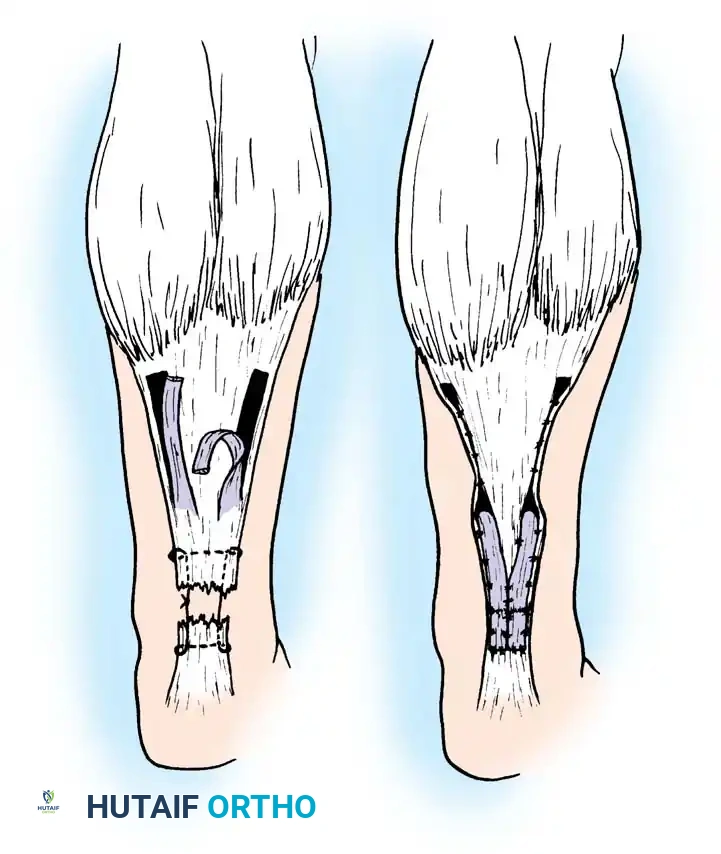
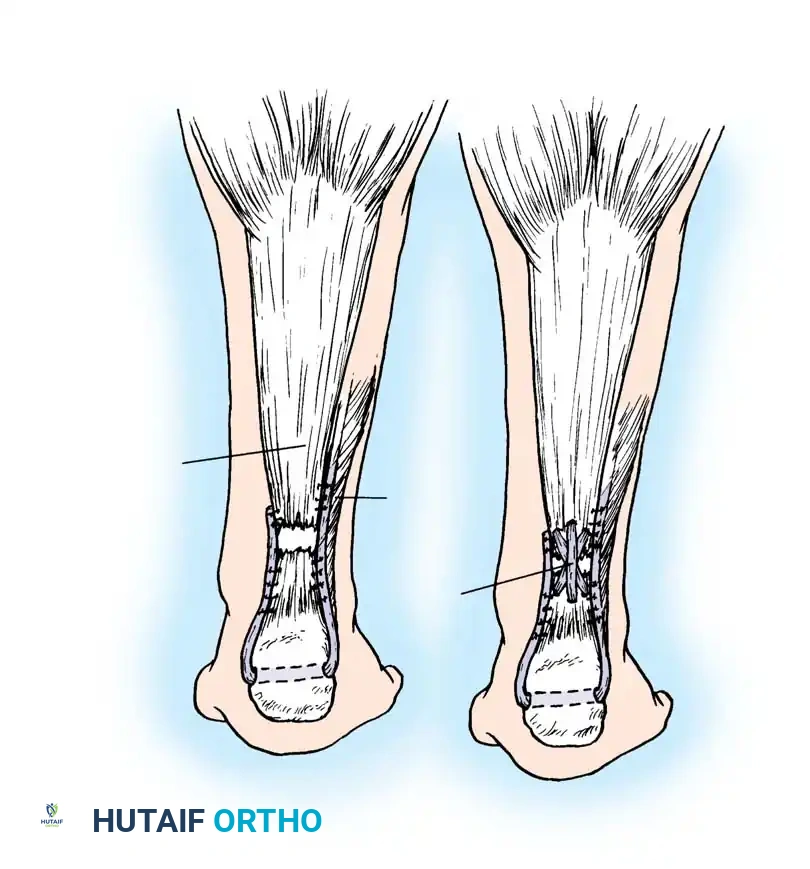
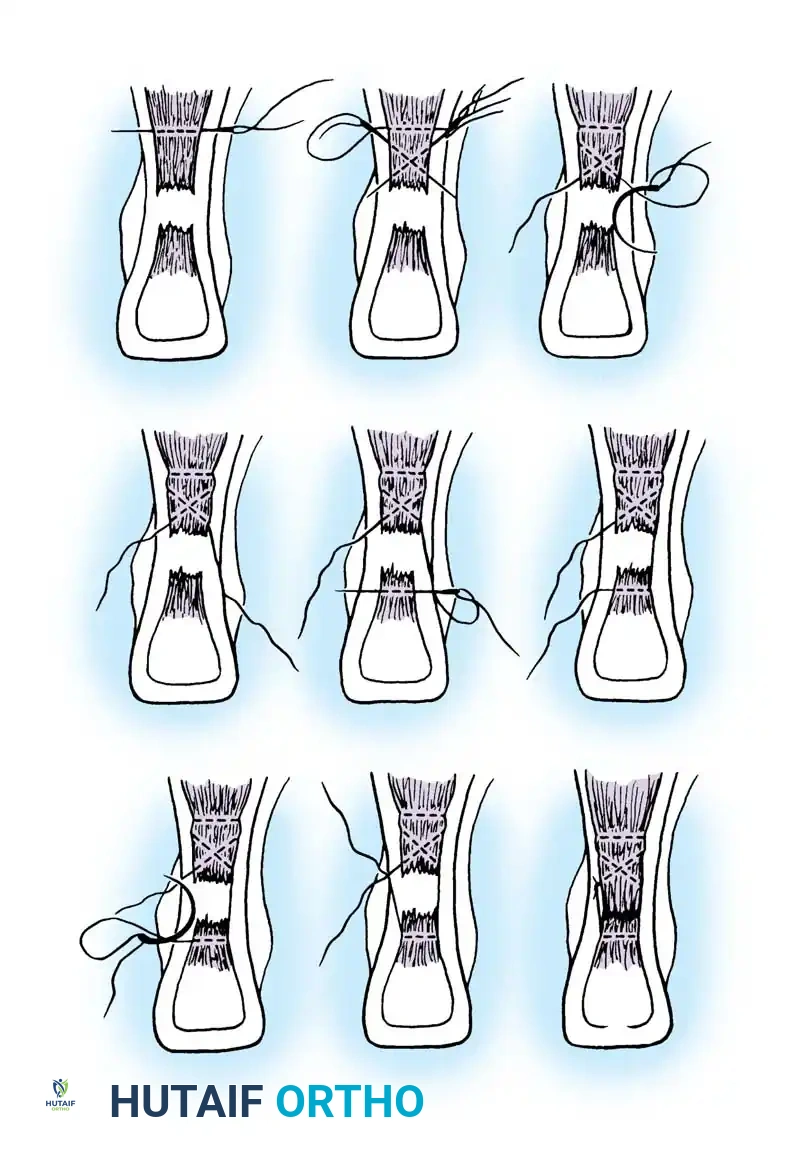
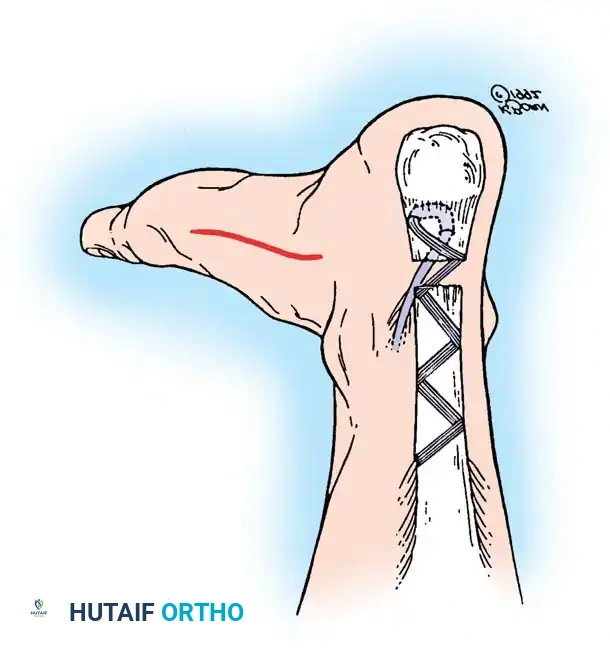
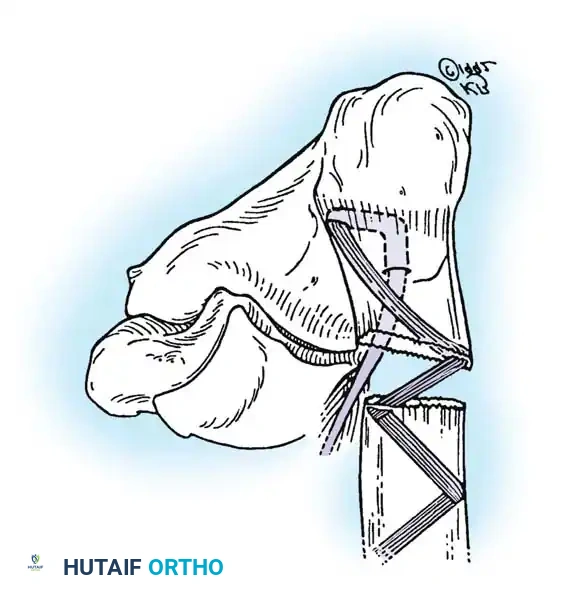
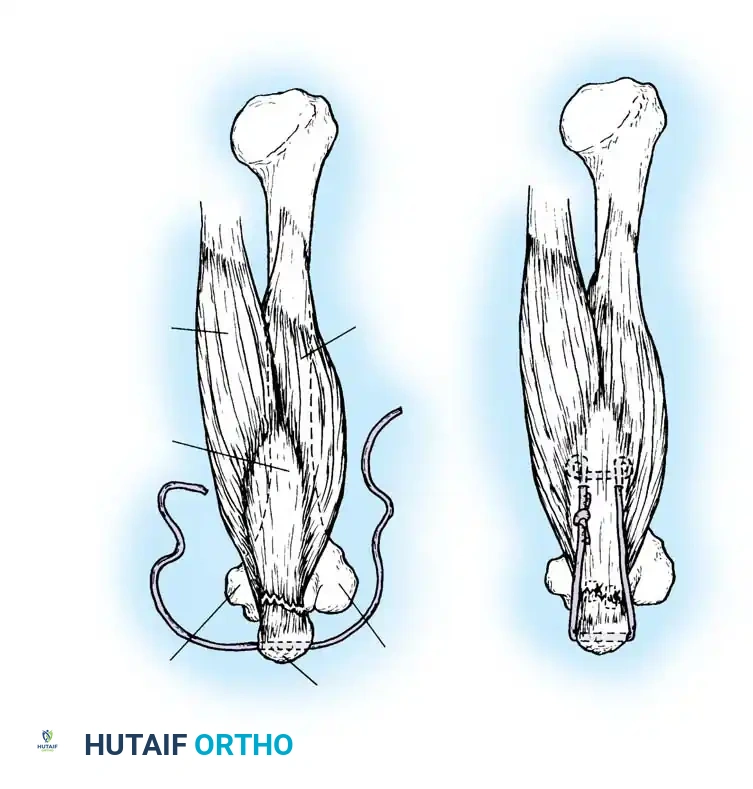
Step 2: Tendon Approximation and Core Suturing
- Debride the "mop-end" frayed edges of the ruptured tendon until healthy, parallel collagen bundles are visualized.
- Approximate the ruptured ends using a heavy, No. 5 nonabsorbable tension suture (e.g., Ethibond or FiberWire).
- Utilize a modified Kessler, Krackow, or Bunnell locking stitch configuration. Pass the suture through the proximal and distal stumps approximately 2.5 cm from the rupture site.
- To set the correct resting tension: Plantar flex the ankle to 0 to 5 degrees of equinus and flex the knee to 15 degrees. Tie the core tension suture securely. Compare the resting tension to the contralateral draped limb.
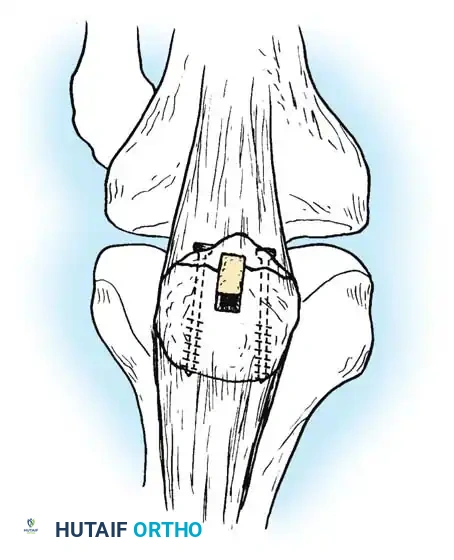
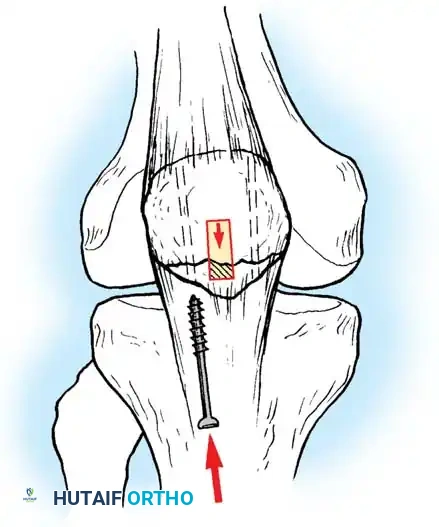
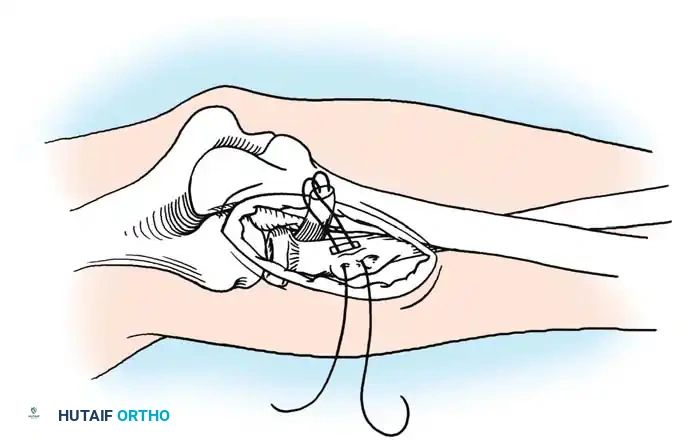
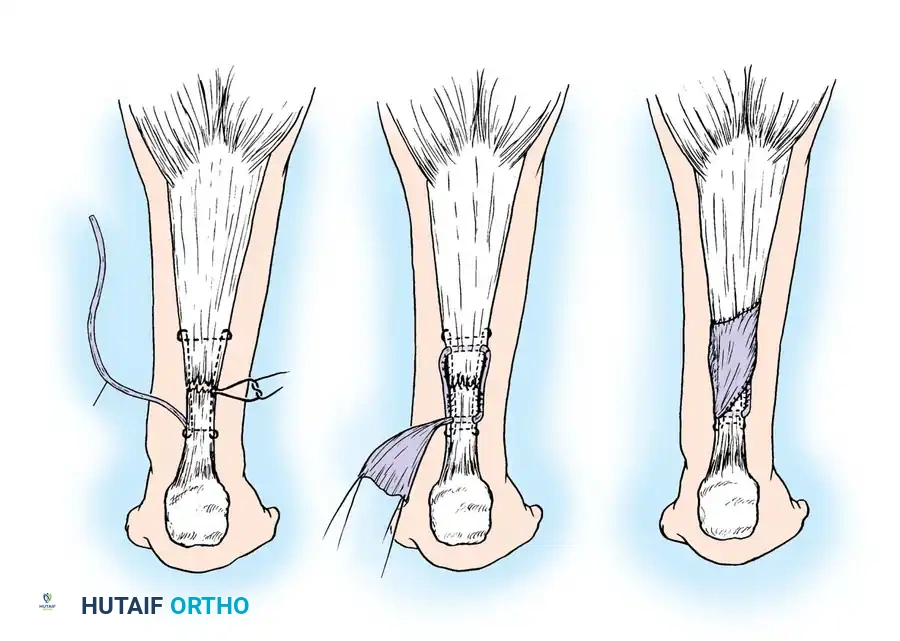
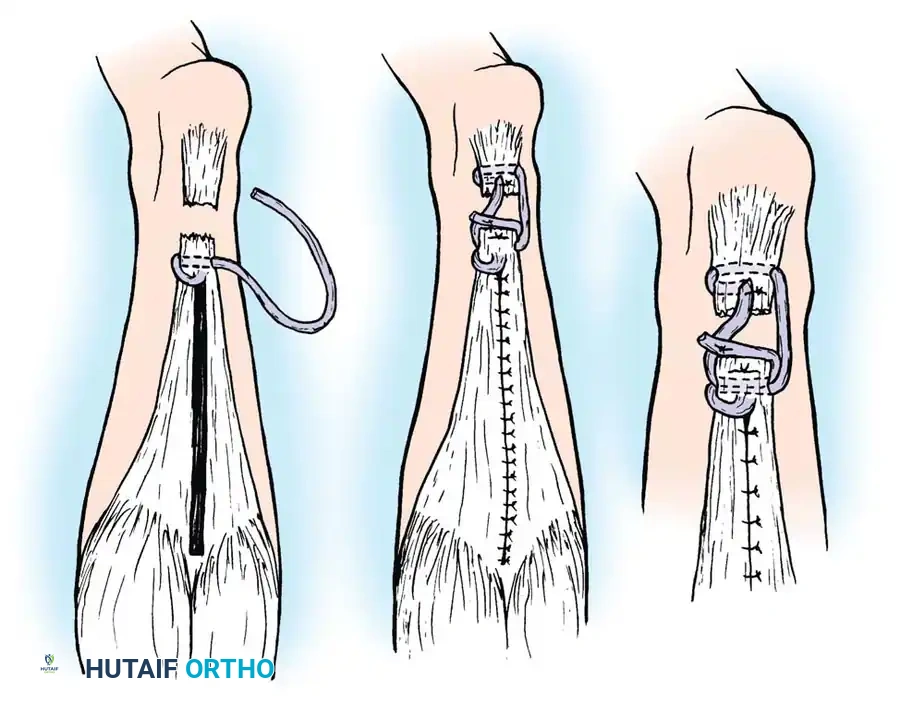
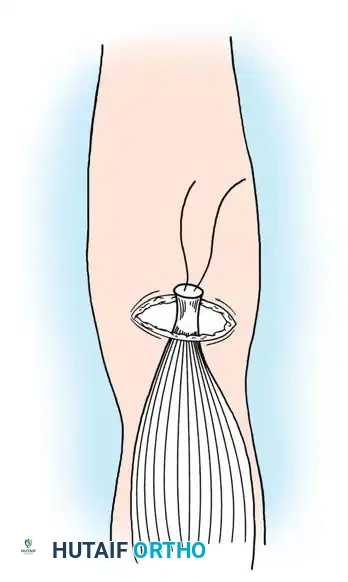
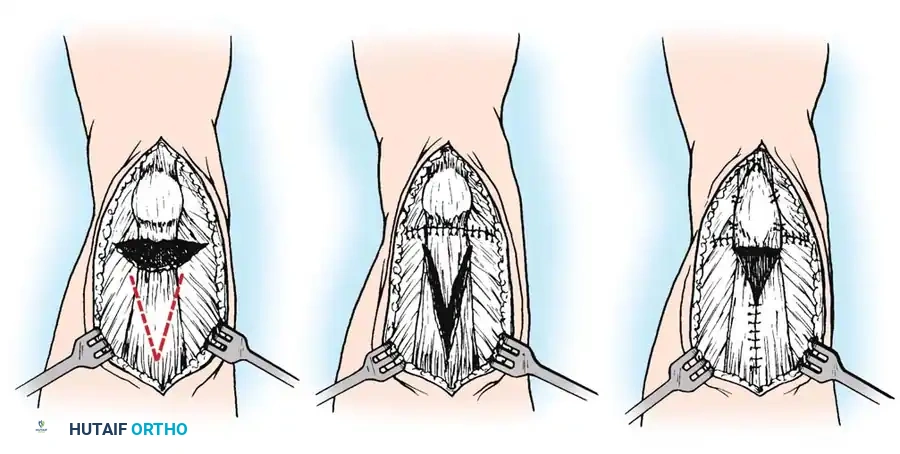
Step 3: Plantaris Tendon Augmentation (Lynn Technique)
Augmentation is highly recommended for degenerative tears or delayed presentations.
- Identify the plantaris tendon medially. Use a tendon stripper to harvest it, releasing it proximally while leaving its distal calcaneal insertion intact.
- Place the harvested plantaris tendon in a moist sponge.
- Repair the frayed epitenon edges of the Achilles rupture with multiple 2-0 absorbable sutures anteriorly and posteriorly to smooth the repair site.
- Thread the free proximal end of the plantaris tendon onto a large fascial needle.
- Pass the plantaris tendon circumferentially—first through the posterior aspect, then through the anterior aspect of the Achilles tendon, approximately 2 cm proximal and distal to the rupture site.
- Fan out the distal portion of the plantaris tendon over the repair site and tack it down with multiple 2-0 absorbable sutures to reinforce the construct.

Step 4: Closure and Immobilization
- Meticulously close the paratenon (fascial sheath) over the repair using 2-0 absorbable sutures. This step is vital to prevent tendon adhesion to the skin and to restore the gliding mechanism.
- Close the subcutaneous tissue and skin with interrupted sutures or staples.
- Apply a sterile, non-adherent dressing.
- Immobilize the extremity in a short leg cast or rigid splint with the foot in gravity equinus (approximately 20-30 degrees of plantar flexion) to remove tension from the repair.
MINIMALLY INVASIVE AND PERCUTANEOUS TECHNIQUES
To mitigate the high wound complication rates associated with open repair, percutaneous and minimally invasive techniques have gained significant traction.
Cretnik et al. compared 105 open repairs with 132 percutaneous repairs, finding comparable functional results but a significantly lower complication rate in the percutaneous group. Lansdaal et al. evaluated a minimally invasive protocol followed by early full weight-bearing, reporting a 92% satisfaction rate and only a 5.5% complication rate.
Key Principles of Percutaneous Repair:
* Small stab incisions are made adjacent to the tendon.
* Specialized jigs (e.g., PARS system or Achillon) are passed deep to the paratenon.
* Sutures are passed transversely through the tendon substance blindly or under ultrasound/endoscopic guidance.
* The sutures are retrieved through a central mini-incision and tied, apposing the tendon ends.
* Risk: The sural nerve is at risk during lateral suture passage. The nerve crosses the lateral border of the Achilles tendon approximately 10 cm proximal to the calcaneal insertion.
POSTOPERATIVE REHABILITATION PROTOCOL
The optimal rehabilitation protocol remains as controversial as the surgical indication itself. However, modern evidence strongly supports early functional rehabilitation over prolonged cast immobilization. Kangas et al. demonstrated that early ankle motion in a functional brace yields excellent results without increasing rerupture rates.
Phase I: Maximum Protection (Weeks 0-2)
- The patient is strictly non-weight-bearing.
- The limb is immobilized in a short leg cast or rigid splint in gravity equinus.
- At 2 weeks, the cast is removed, the wound is inspected, and sutures/staples are removed.
Phase II: Controlled Mobilization (Weeks 2-6)
- Weeks 2-4: The patient is transitioned to a removable functional brace (e.g., CAM boot) with heel wedges to maintain plantar flexion. Partial weight-bearing with crutches is initiated.
- Weeks 4-6: Heel wedges are sequentially removed (usually one per week) to gradually bring the foot to a plantigrade position.
- Gentle active range-of-motion (ROM) exercises (plantar flexion and dorsiflexion to neutral) are begun for 20 minutes twice a day. Passive stretching is strictly prohibited.


📚 Medical References
- , Clin Orthop Relat Res 458:188, 2007.
- Coleman BD, Khan KM, Kiss ZS, et al: Open and arthroscopic patellar tenotomy for chronic patellar tendinopathy: a retrospective outcome study, Victorian Institute of Sport Tendon Study Group, Am J Sports Med 28:183, 2000.
- Cook JL, Khan KM, Harcourt PR, et al: Patellar tendon ultrasonography in asymptomatic active athletes reveals hypoechoic regions: a study of 320 tendons, Victorian Institute of Sport Tendon Study Group, Clin J Sports Med 8:73, 1998.
- Cretnik A, Kosanovic M, Smrkolj V: Percutaneous versus open repair of the ruptured Achilles tendon: a comparative study, Am J Sports Med 33:1369, 2005.
- D’Alessandro DF, Shields CL, Tibone JE, et al: Repair of the distal biceps tendon ruptures in athletes, Am J Sports Med 21:114, 1993.
- Dobbie RP: Avulsion of the lower biceps brachii tendon: analysis of 51 previously unreported cases, Am J Surg 51:662, 1941.
- Ecker ML, Lotke PA, Glazer RM: Late reconstruction of the patellar tendon, J Bone Joint Surg 61A:884, 1979.
- Falchook FS, Zlatkin MB, Erbacher GE, et al: Rupture of the distal biceps tendon: evaluation with MR imaging, Radiology 190:659, 1994.
- Falconiero RP, Pallis MP: Chronic rupture of a patellar tendon: a technique for reconstruction with Achilles allograft, Arthroscopy 12:623, 1996.
- Ferretti A, Conteduca F, Camerucci E, et al:
You Might Also Like