Revision Arthroplasty with Femoral Bone Loss: Metal Augments
Key Takeaway
Looking for accurate information on Revision Arthroplasty with Femoral Bone Loss: Metal Augments? Revision total knee arthroplasty with femoral bone involves addressing bone defects, common in revision surgery, using modular femoral metal augments. These augments maximize bone-prosthesis contact, restoring the femorotibial joint line and posterior condylar offset. They are crucial for managing moderate to large bone loss in arthroplasty with femoral bone, improving prosthesis function and stability.
Comprehensive Introduction and Patho-Epidemiology
The landscape of adult reconstruction is experiencing a paradigm shift driven by the exponential growth in revision total knee arthroplasty (rTKA). Current epidemiological models project that the number of revision TKA procedures performed will continue to increase at an annual rate of 19.3%, placing an unprecedented burden on healthcare systems globally. This surge is largely attributable to the expanding indications for primary TKA in younger, more active demographics, coupled with the inevitable survivorship limitations of current bearing surfaces and fixation interfaces. As the volume of primary arthroplasties escalates, so too does the complexity of the revision burden, demanding a highly sophisticated understanding of reconstructive principles from the arthroplasty surgeon.

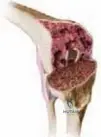
While femoral bone defects are relatively uncommon in primary TKA—typically reserved for severe dysplasias or post-traumatic deformities—they represent a ubiquitous and formidable challenge in the revision setting. The pathogenesis of femoral bone loss is multifactorial and dictates the reconstructive strategy. In unoperated knees, bone loss can be initiated by previous osteochondral defects, avascular necrosis, severe valgus or varus deformity, posttraumatic arthritis, and Charcot arthropathy. However, in the revision scenario, osteolysis secondary to particulate wear debris (predominantly polyethylene) and iatrogenic bone loss secondary to the extraction of well-fixed components or cement mantles are the most common etiologies. The biological cascade leading to periprosthetic osteolysis is primarily driven by a macrophage-mediated inflammatory response to particulate wear debris. In older generations of conventional polyethylene, submicron particles generated at the articular surface migrate into the effective joint space, infiltrating the bone-implant or bone-cement interface.

Macrophages phagocytize these particles and, unable to digest them, release a cascade of pro-inflammatory cytokines, including Tumor Necrosis Factor-alpha (TNF-α), Interleukin-1 (IL-1), and Interleukin-6 (IL-6). These cytokines stimulate the Receptor Activator of Nuclear factor Kappa-B Ligand (RANKL) pathway, which promotes osteoclastogenesis and subsequent focal bone resorption. On the femoral side, this osteolysis frequently manifests as expansile, cavitary defects within the distal metaphysis and posterior condyles. Furthermore, stress shielding induced by rigid femoral components can lead to adaptive bone remodeling and progressive cortical thinning according to Wolff’s Law, compounding the structural deficiency encountered during revision surgery.

Beyond biological osteolysis, the mechanical extraction of the primary femoral component inevitably results in some degree of iatrogenic bone loss. Well-fixed cemented components require meticulous disruption of the implant-cement and cement-bone interfaces. The use of aggressive extraction techniques, such as standard osteotomes or excessive mallet force, can easily precipitate avulsion of the medial or lateral epicondyles—a catastrophic complication that compromises collateral ligament origins and fundamentally alters the reconstructive algorithm toward constrained or hinged devices. Consequently, the contemporary approach to component extraction relies on flexible osteotomes, pencil burrs, and ultrasonic cement removal tools to preserve the maximum volume of viable metaphyseal bone stock.

To address these defects, modular femoral augments have become an indispensable tool in the arthroplasty surgeon's armamentarium. They are particularly efficacious for moderate-sized, uncontained bony defects, allowing the surgeon to maximize bone–prosthesis contact while accurately restoring the joint line and posterior condylar offset. Recent advancements in prosthesis design and the introduction of highly porous biomaterials (such as trabecular metal and 3D-printed titanium) have further expanded the versatility of metal augments, enabling stable reconstruction even in the presence of increasingly larger metaphyseal defects that previously would have necessitated structural allografting.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of distal femoral anatomy and knee biomechanics is requisite for successful revision arthroplasty. The primary objective in managing femoral bone loss is not merely "filling the defect," but rather the precise anatomic restoration of the femorotibial joint line and the posterior condylar offset. Significant alterations in either parameter will precipitously degrade the kinematics, stability, and longevity of the revision prosthesis. The distal femur is characterized by its complex metaphyseal flare and the critical ligamentous origins of the medial collateral ligament (MCL) and lateral collateral ligament (LCL) on the respective epicondyles, which must be meticulously preserved and anatomically referenced during reconstruction.

Topographically, the native joint line typically lies approximately 25 mm distal to the medial epicondyle and 25 to 30 mm distal to the lateral epicondyle, or roughly 10 mm proximal to the inferior pole of the patella. The posterior femoral condyles exhibit an average offset of 25.8 mm from the posterior cortex of the femoral diaphysis. In the setting of revision surgery, the distal and posterior femoral condyles are the most frequent sites of volumetric bone loss due to the combination of osteolysis and the geometric realities of primary implant extraction. The loss of distal femoral bone invariably tempts the unwary surgeon to seat the revision femoral component too proximally, leading to a cascade of biomechanical failures.

Failure to restore the distal femoral joint line typically results in joint line elevation. Biomechanically, an elevated joint line fundamentally alters the isometry of the collateral ligaments. Because the collateral ligaments originate on the epicondyles (which remain static) and insert on the tibia and fibula, moving the joint line proximally creates relative laxity in mid-flexion. This mid-flexion instability is a hallmark of poorly executed revision TKA. Furthermore, joint line elevation necessitates the use of thicker tibial polyethylene inserts to achieve extension stability. This compensatory maneuver paradoxically tightens the flexion gap, restricts postoperative range of motion, and induces patella baja (or pseudo-patella baja), which alters patellofemoral tracking and increases retropatellar contact forces, leading to anterior knee pain and accelerated wear.

Conversely, failure to restore the posterior condylar offset diminishes the moment arm of the extensor mechanism and limits maximum flexion due to early mechanical impingement of the posterior tibial margin against the femoral diaphysis. The posterior condylar offset is critical for maintaining the tension of the posterior capsule and optimizing the rollback mechanism of the femur on the tibia. Utilizing posterior metal augments allows the surgeon to build out the posterior condyles to their native dimensions, thereby restoring the flexion gap volume, optimizing the extensor mechanism mechanical advantage, and preventing early impingement, which is paramount for achieving high-flexion outcomes in the revision setting.
Exhaustive Indications and Contraindications
The decision to utilize modular metal augments in revision TKA is predicated on a meticulous assessment of the bone defect morphology, size, and containment, typically categorized using the Anderson Orthopaedic Research Institute (AORI) classification system. Metal augments are the gold standard for AORI Type IIa (metaphyseal damage involving one condyle) and Type IIb (metaphyseal damage involving both condyles) defects where the remaining metaphyseal bone is structurally sound enough to support the augment and the diaphyseal stem can achieve rigid fixation. They are specifically indicated for uncontained defects ranging from 5 mm to 15 mm in depth, where particulate bone grafting would lack structural integrity and structural allografts would introduce unnecessary biological complexity and risk of non-union or disease transmission.

Modular augments offer several distinct advantages over alternative reconstruction methods. They provide immediate, rigid structural support, allowing for precise gap balancing and joint line restoration. Their modularity permits intraoperative customization; surgeons can independently address distal and posterior defects, mixing and matching augment thicknesses (e.g., 5 mm, 10 mm, 15 mm) to perfectly tension the flexion and extension gaps. Furthermore, the advent of highly porous titanium and tantalum augments has revolutionized the biological interface, facilitating robust osteointegration and potentially reducing the reliance on polymethylmethacrylate (PMMA) cement for long-term stability, thereby mitigating the risk of future cement-associated osteolysis.
Despite their versatility, metal augments are not a panacea and possess distinct contraindications. They are contraindicated in AORI Type III defects, which are characterized by massive, uncontained metaphyseal bone loss that compromises the collateral ligament origins and precludes stable seating of the augment. In such catastrophic bone loss scenarios, the remaining bone shell is insufficient to support the compressive and shear forces transmitted through the augment, leading to inevitable subsidence and catastrophic failure. These defects necessitate more aggressive reconstructive strategies, such as metaphyseal cones, diaphyseal engaging sleeves, structural allograft-prosthesis composites, or distal femoral replacement (megaprosthesis).

Additionally, the use of metal augments must be carefully considered in the setting of active periprosthetic joint infection (PJI). While some surgeons may utilize them during the second stage of a two-stage exchange arthroplasty once the infection is eradicated, their use in single-stage revisions for active infection is highly controversial due to the increased surface area for bacterial biofilm formation, particularly with highly porous metals. Severe osteopenia or irradiated bone also presents a relative contraindication, as the host bone may lack the mechanical strength to support the augment, increasing the risk of periprosthetic fracture or early loosening.
Summary of Indications and Contraindications
| Clinical Scenario / Defect Characteristic | Indications for Metal Augments | Contraindications for Metal Augments |
|---|---|---|
| AORI Defect Classification | Type I (minor), Type IIa, Type IIb | Type III (massive uncontained loss) |
| Defect Depth / Size | 5 mm to 15 mm uncontained defects | > 15-20 mm (Consider cones/sleeves) |
| Host Bone Quality | Adequate metaphyseal rim support | Severe osteoporosis, irradiated bone |
| Ligamentous Integrity | Intact epicondyles and collateral origins | Avulsed epicondyles (Requires hinge/DFR) |
| Infectious Status | Aseptic revision, 2nd stage reimplantation | Active, uncontrolled PJI (1st stage) |
| Biological Considerations | Need for immediate structural stability | Need for biological bone stock restoration |
Pre-Operative Planning, Templating, and Patient Positioning
Exhaustive pre-operative planning is the cornerstone of successful revision total knee arthroplasty, particularly when addressing significant femoral bone loss. The diagnostic workup must unequivocally rule out periprosthetic joint infection through serum inflammatory markers (ESR, CRP) and synovial fluid analysis (cell count, differential, alpha-defensin, and culture) prior to addressing the mechanical failure. Once asepsis is confirmed, high-quality, orthogonal radiographic imaging is mandatory. This includes weight-bearing anteroposterior (AP), lateral, skyline patellar, and full-length standing hip-to-ankle radiographs to assess the overall mechanical axis and identify any extra-articular deformities that may influence the reconstructive axis.

Digital templating is a critical phase of the pre-operative workflow. Utilizing specialized orthopedic software with magnification calibration (typically via a 25 mm spherical marker placed at the level of the joint), the surgeon must estimate the size of the required femoral component, the anticipated length and diameter of the diaphyseal stem, and the probable size and location of the metal augments. The joint line must be meticulously templated from static landmarks, such as the adductor tubercle, the medial epicondyle, and the fibular head. Advanced imaging, specifically computed tomography (CT) with metal artifact reduction sequence (MARS), is increasingly utilized to generate three-dimensional models of the bone defects, allowing for highly accurate volumetric assessment and pre-operative sizing of augments, cones, or sleeves.
Patient positioning and operating room setup must be optimized to facilitate extensile exposures and intraoperative fluoroscopy. The patient is typically positioned supine on a radiolucent operating table, allowing for unobstructed intraoperative C-arm imaging, which is vital for confirming stem trajectory and augment seating. A proximal thigh tourniquet is applied, though its inflation may be delayed or omitted depending on the patient's vascular status and the anticipated duration of the procedure. The entire limb is prepped and draped free to allow for full manipulation and dynamic assessment of kinematics and stability throughout the reconstructive process.
The surgical armamentarium must be fully stocked and readily available. This includes the complete revision arthroplasty system, a wide array of modular metal augments (distal, posterior, and combined), metaphyseal cones and sleeves (as backup for underestimated defects), diaphyseal stems of various lengths and diameters (both straight and bowed), and specialized extraction equipment. The surgeon must mentally rehearse the surgical sequence, anticipating potential intraoperative challenges, such as the need for a quadriceps snip or tibial tubercle osteotomy to achieve adequate exposure without compromising the extensor mechanism.
Step-by-Step Surgical Approach and Fixation Technique
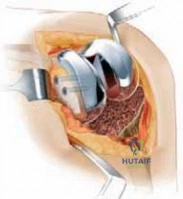
The surgical approach for revision TKA with femoral bone loss demands an extensile exposure that provides circumferential access to the distal femur without jeopardizing the extensor mechanism. A standard medial parapatellar arthrotomy is typically utilized, often incorporating the previous surgical incision. If exposure is compromised by severe arthrofibrosis or patella baja, the surgeon must seamlessly transition to an extensile maneuver, such as a quadriceps snip or a formal tibial tubercle osteotomy (TTO). The TTO is particularly advantageous when managing massive femoral defects, as it allows for complete eversion of the extensor mechanism and unimpeded access to the diaphyseal canal.

Following meticulous component extraction and radical debridement of all particulate debris, pseudocapsule, and osteolytic membranes, the true extent of the femoral bone loss is unmasked. The reconstructive sequence generally dictates establishing the tibial platform first, as this provides a stable, orthogonal reference plane for subsequent gap balancing. Attention is then directed to the femur. The femoral diaphyseal canal is sequentially reamed to establish the anatomical axis and determine the appropriate stem diameter and length for diaphyseal fixation. Diaphyseal engagement is critical; the stem must bypass the metaphyseal defect and achieve rigid cortical contact over a distance of at least two cortical diameters to effectively offload the compromised metaphysis and the modular augments.

With the trial stem engaged in the diaphysis, the femoral trial component is applied, and the flexion and extension gaps are meticulously assessed. It is during this trialing phase that the precise requirement for metal augments is determined. If the extension gap is loose but the flexion gap is stable, distal femoral augments are indicated to translate the joint line distally and tighten the extension gap. Conversely, if the flexion gap is loose, posterior condylar augments are required to increase the anteroposterior dimension of the femur, tightening the flexion gap and restoring the posterior offset. Often, combined distal and posterior augments are necessary to achieve a harmonious, rectangular gap in both flexion and extension.

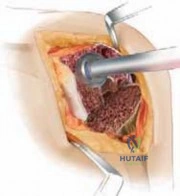
Preparation of the host bone to receive the augments requires exacting precision. The sclerotic bone bed must be freshened to bleeding cancellous bone to facilitate cement interdigitation or biological ingrowth (if using highly porous, cementless augments). This is achieved using specialized milling systems or oscillating saws guided by the trial component. The goal is to create a perfectly flat, bleeding surface that maximizes contact area with the augment. Any residual gaps between the augment and the host bone will concentrate stress and precipitate early mechanical failure.

The final assembly and implantation of the construct must be executed flawlessly. The modular augments are securely fastened to the definitive femoral component using the manufacturer's proprietary locking mechanisms (typically screws or Morse tapers), ensuring absolute torque specifications are met to prevent micromotion and fretting corrosion. Depending on the surgeon's philosophy and the specific implant design, the augments may be cemented to the host bone (hybrid fixation) or implanted without cement (press-fit) if utilizing highly porous biomaterials designed for osteointegration. Regardless of the augment fixation strategy, the diaphyseal stem is typically implanted cementless to achieve rigid, long-term biological fixation, while the articular surface is secured with a modern, highly cross-linked polyethylene bearing.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and advanced implant designs, revision TKA with metal augments is a formidable undertaking associated with a distinct complication profile. The success of the reconstruction hinges on the delicate balance between rigid mechanical fixation and the biological capacity of the compromised host bone. When this balance is disrupted, complications ensue, necessitating complex salvage strategies.

Aseptic loosening remains a primary mode of failure, particularly at the bone-augment interface. If the host bone is inadequately prepared or if the diaphyseal stem fails to achieve rigid initial fixation, micromotion at the metaphyseal level will prevent osteointegration of porous augments or fracture the cement mantle of cemented augments. This leads to progressive radiolucent lines, subsidence of the femoral component, and recurrent instability. Furthermore, the modular junctions between the augments and the baseplate are susceptible to fretting corrosion and mechanical dissociation, particularly if the locking screws are inadequately torqued or if the patient engages in high-impact activities.

Periprosthetic joint infection (PJI) is a devastating complication, with incidence rates in revision TKA significantly higher than in primary procedures. The extensive soft tissue dissection, prolonged operative times, and the presence of massive, modular implants with numerous interfaces create an environment highly conducive to bacterial colonization and biofilm formation. Management of PJI in the setting of massive metal augments almost universally requires a two-stage exchange arthroplasty, involving the challenging extraction of the well-fixed diaphyseal stems and augments, radical debridement, placement of an articulating antibiotic spacer, and prolonged systemic antimicrobial therapy prior to reimplantation.

Periprosthetic fractures can occur intraoperatively during the preparation of the sclerotic bone or postoperatively due to stress risers created by the rigid diaphyseal stems transitioning to osteopenic bone. Intraoperative fractures of the epicondyles are particularly disastrous, as they compromise collateral ligament stability. Salvage management for severe complications or progressive bone loss that renders modular augments insufficient (transitioning to an AORI Type III defect) involves escalating the reconstructive ladder. This includes the utilization of highly porous metaphyseal cones or diaphyseal engaging sleeves to bypass the deficient metaphysis entirely, or, in the most extreme cases of catastrophic bone loss or ligamentous incompetence, the deployment of a distal femoral replacement (megaprosthesis) with a rotating hinge mechanism.
Complications and Salvage Strategies
| Complication | Estimated Incidence | Pathomechanism | Salvage / Management Strategy |
|---|---|---|---|
| Aseptic Loosening | 4% - 8% | Failure of stem fixation, micromotion at augment interface, cement mantle fracture. | Revision to longer/thicker diaphyseal stem; upgrade to metaphyseal cones or sleeves. |
| Periprosthetic Infection | 3% - 7% | Biofilm formation on modular interfaces; compromised soft tissue envelope. | Two-stage exchange arthroplasty; aggressive debridement; antibiotic spacers. |
| Augment Dissociation | < 1% | Inadequate torque of locking screws; high-impact cyclic loading; fretting corrosion. | Component revision; replacement of locking mechanisms; potential transition to monolithic implant. |
| Periprosthetic Fracture | 2% - 5% | Stress shielding at stem tip; intraoperative aggressive reaming; osteopenia. | Open reduction internal fixation (ORIF) with locking plates; revision to longer stem bypassing fracture. |
| Joint Line Elevation | 10% - 15% | Underestimation of distal bone loss; inadequate use of distal augments. | Revision of femoral component with thicker distal augments; patellar resurfacing/realignment. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following revision TKA with femoral metal augments is a highly customized, phased protocol that must carefully balance the competing demands of early mobilization to prevent arthrofibrosis and the protection of the complex bone-implant interfaces to ensure long-term fixation. The specific protocol is heavily influenced by the method of diaphyseal fixation (cemented vs. cementless), the quality of the host bone, and the integrity of the extensor mechanism (particularly if a tibial tubercle osteotomy or quadriceps snip was utilized).

Phase 1: Immediate Post-Operative Phase (Weeks 0-2)
The primary goals during this acute phase are the management of pain and edema, the initiation of deep vein thrombosis (DVT) prophylaxis, and the early restoration of passive and active-assisted range of motion (ROM). If rigid diaphyseal press-fit fixation was achieved and the extensor mechanism is intact, patients are typically permitted weight-bearing as tolerated (WBAT) with an assistive device. However, if bone quality is poor, or if a structural allograft was incorporated alongside the augments, protected weight-bearing (toe-touch or partial) may be mandated for 6 weeks. Continuous passive motion (CPM) machines may be utilized, and early patellar mobilization is critical to prevent infrapatellar contractures.
Phase 2: Early Rehabilitation Phase (Weeks 2-6)
As soft tissue healing progresses, the focus shifts toward active ROM, progressive strengthening of the quadriceps and hamstrings, and gait normalization. Closed kinetic chain exercises, such as mini-squats and leg presses, are introduced cautiously to minimize shear forces across the joint line. Aquatic therapy can be highly beneficial during this phase, providing a buoyant environment that reduces joint loading while allowing for aggressive ROM and strengthening. If an extensile exposure (e.g., TTO) was utilized, active terminal extension exercises may be restricted or delayed until radiographic evidence of initial bony healing is observed.

Phase 3: Advanced Rehabilitation Phase (Weeks 6-12)
By week 6, assuming uncomplicated healing and stable clinical and radiographic follow-up, weight-bearing restrictions are typically lifted. The rehabilitation program intensifies, focusing on proprioception, balance training, and functional strengthening. Stationary cycling with progressive resistance is a cornerstone of this phase, promoting both cardiovascular endurance and dynamic joint mobility. The physical therapist will heavily emphasize eccentric quadriceps control to ensure stability during descending stairs and deceleration activities.
Phase 4: Return to Function (Months 3-6+)
The final phase of rehabilitation is tailored to the patient's specific lifestyle and functional goals. While high-impact activities (e.g., running, jumping) are universally discouraged following revision arthroplasty to protect the modular interfaces from cyclic fatigue failure, patients are encouraged to return to low-impact recreational activities such as swimming, cycling, and golf. Long-term clinical and radiographic surveillance is mandatory, with annual or biennial evaluations to monitor for asymptomatic osteolysis, augment subsidence, or polyethylene wear.
Summary of Landmark Literature and Clinical Guidelines
The evolution of revision total knee arthroplasty and the management of femoral bone loss has been guided by several landmark studies and evolving clinical guidelines. A foundational pillar of this literature is the work by Engh and Ammeen, who developed the Anderson Orthopaedic Research Institute (AORI) classification system. This classification provided the first standardized, reproducible framework for quantifying metaphyseal bone loss and directly correlating defect morphology with appropriate reconstructive strategies, firmly establishing the role of metal augments for Type II defects.

The critical importance of joint line restoration was elegantly demonstrated in biomechanical and clinical studies by Patel et al. and Figgie et al. These authors quantified the kinematic penalties of joint line elevation, demonstrating that proximal translation of the joint line by more than 8 mm significantly alters collateral ligament isometry, leading to mid-flexion instability, reduced functional outcome scores, and accelerated failure rates. This literature underscores the absolute necessity of utilizing distal femoral augments to meticulously restore the native joint line topography.