Mastering Revision THA: Fluted Stems for Femoral Bone Loss
Key Takeaway
Join us for an immersive masterclass on revision total hip arthroplasty utilizing fluted femoral stems. We'll meticulously cover comprehensive surgical anatomy, critical preoperative planning, and granular intraoperative execution for addressing femoral bone loss. Learn precise techniques for reaming, implant placement, and managing complex defects, alongside essential pearls, pitfalls, and detailed postoperative protocols. This guide is designed for fellows to master challenging revision scenarios.
Comprehensive Introduction and Patho-Epidemiology
Fellows and colleagues, welcome to the definitive discourse on one of the most demanding yet intellectually and surgically rewarding frontiers in adult reconstruction: Revision Total Hip Arthroplasty (THA) utilizing fluted, tapered titanium stems for the management of severe femoral bone loss. This is not merely an operation of component exchange; it is a complex reconstructive salvage of a biomechanically compromised femur. The modern orthopedic surgeon must approach these cases not just as a mechanic swapping parts, but as a structural engineer tasked with rebuilding a foundation that has been critically undermined by osteolysis, stress shielding, or iatrogenic trauma. The fluted, tapered stem represents a paradigm shift in our armamentarium, offering reliable diaphyseal fixation when the proximal metaphysis is no longer capable of supporting an implant.
To master this technique, one must first possess a profound understanding of the pathogenesis of failure. The overwhelming majority of these cases stem from particulate-induced periprosthetic osteolysis. Historically, the normal wear of the acetabular liner—particularly conventional ultra-high-molecular-weight polyethylene (UHMWPE)—produced billions of submicron particles. As this debris accumulates within the effective joint space, it triggers a relentless, chronic inflammatory cascade. Macrophages engulf these particles but cannot digest them, leading to the release of pro-inflammatory cytokines such as TNF-alpha, IL-1, IL-6, and PGE2. This cytokine storm stimulates osteoclastic bone resorption and inhibits osteoblastic bone formation, ultimately destroying the critical bone-implant interface and resulting in aseptic loosening.
Unaddressed, a loose femoral implant subjected to cyclical loading follows a predictable and catastrophic natural history. The micromotion of the unstable stem acts as a mechanical abrasive, further eroding the endosteal cortex. Progressive cortical thinning ensues, frequently accompanied by angular deformation—most commonly varus collapse—as the proximal femur loses its structural integrity. This biomechanical downward spiral dramatically increases the risk of a periprosthetic fracture, which can occur spontaneously or with minimal trauma. In severe manifestations, the proximal bone deficiency around the lesser trochanter becomes so profound that metaphyseal-engaging stems are entirely obsolete.
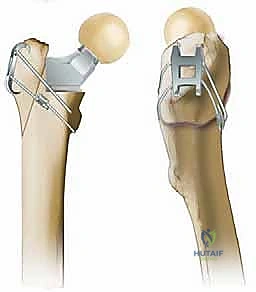
In these dire scenarios of Paprosky Type IIIA and IIIB bone loss, the fluted, tapered titanium stem becomes our reconstructive workhorse. Unlike cylindrical fully porous-coated stems, which rely on a tight diaphyseal scratch fit over a long distance, the fluted tapered stem achieves immediate axial stability through its conical geometry. As the stem is impacted, it generates compressive hoop stresses within the femoral diaphysis, wedging itself into stability. Simultaneously, the longitudinal flutes cut into the cortical bone, providing exceptional rotational stability. Manufactured from titanium alloy, these stems offer a modulus of elasticity closer to that of cortical bone compared to cobalt-chrome, thereby mitigating distal stress shielding while promoting robust proximal osteointegration.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, a profound, three-dimensional spatial awareness of the proximal femur, its muscular envelope, and adjacent neurovascular structures is absolutely paramount. In the revision setting, normal anatomic planes are frequently obliterated by dense, unyielding scar tissue, heterotopic ossification, and distorted osteology. The proximal femur—comprising the head, neck, greater trochanter, and lesser trochanter—is frequently the epicenter of massive cavitary and segmental defects. Our primary surgical target is the femoral diaphysis; therefore, the endosteal diameter, anterior bowing, and cortical integrity of the shaft must be meticulously evaluated to ensure it can withstand the hoop stresses generated by a tapered stem.

The soft tissue envelope dictates our exposure and ultimately provides the dynamic stability of the reconstructed hip. The iliotibial band (ITB) and tensor fascia lata (TFL) form our lateral window. Deep to this, the gluteal musculature requires fastidious management. The gluteus maximus inserts onto the posterolateral border of the proximal femur, forming the "gluteal sling." In complex revisions, particularly when correcting severe leg length discrepancies or performing an Extended Trochanteric Osteotomy (ETO), this insertion often necessitates partial release. The gluteus medius and minimus—the primary abductors—are frequently compromised by prior surgery, osteolysis, or trochanteric nonunion. Their preservation, mobilization, and secure reattachment are non-negotiable prerequisites for preventing postoperative instability and a debilitating Trendelenburg gait.

Neurovascular vigilance must be maintained throughout the procedure. The sciatic nerve is the most frequently injured neurologic structure during posterior revision approaches. In revision scenarios, it is often encased in dense perineural fibrosis, tethering it to the posterior capsule and short external rotators. It typically lies 1 to 2 cm posterior to the posterior rim of the acetabulum. Routine neurolysis is generally discouraged unless the nerve is directly in the operative field or severe deformity correction is planned; instead, careful retractor placement and maintaining the hip in extension and external rotation during posterior dissection minimizes tension. Anteriorly, the femoral artery and vein are at risk during aggressive anterior capsulectomy or if an errant retractor is placed over the anterior column.
Biomechanically, the success of the fluted stem relies on the principles originally elucidated by Wagner. The geometry is a 2-degree to 3-degree taper. This conical shape ensures that as the stem subsides microscopically under initial physiological loading, it becomes increasingly wedged into the diaphyseal cortex, achieving a state of "stable subsidence." The longitudinal flutes serve a dual purpose: they provide sharp longitudinal edges that bite into the endosteum to resist torsional forces, and they create channels that allow for the egress of marrow contents and reaming debris, thereby reducing the risk of intraoperative fat embolism. The modularity of modern designs allows the surgeon to independently establish rigid distal fixation before dialing in the proximal body to optimize version, offset, and leg length.
Exhaustive Indications and Contraindications
The decision to utilize a fluted, tapered stem is dictated by the precise quantification of femoral bone loss. We rely heavily on the Paprosky classification system, which evaluates the integrity of the metaphysis and diaphysis to guide implant selection. Fluted stems are the gold standard for Paprosky Type IIIA and Type IIIB defects. In Type IIIA, the metaphysis is severely damaged and non-supportive, but there is more than 4 cm of intact diaphyseal bone available for fixation at the isthmus. In Type IIIB, the diaphyseal bone is also compromised, leaving less than 4 cm of scratch fit available. Here, long, modular, fluted tapered stems are required to bypass the defect and achieve fixation in the distal third of the femur.

Beyond aseptic loosening with massive osteolysis, fluted stems are highly indicated in the management of complex periprosthetic femur fractures, specifically Vancouver Type B2 (fracture around a loose stem with adequate bone stock) and Type B3 (fracture around a loose stem with poor bone stock). The tapered geometry allows the stem to bypass the fracture site, providing an internal intramedullary strut that, when combined with cerclage cabling or structural allografts, creates a biomechanically stable construct conducive to fracture union. Furthermore, in cases of severe femoral malalignment or deformity resulting from prior trauma or osteotomies, the modularity of these stems allows for corrective osteotomies of the femur while maintaining independent control of the proximal joint mechanics.

Despite their versatility, fluted stems are not a panacea and possess strict contraindications. The absolute contraindication to any single-stage revision arthroplasty is active periprosthetic joint infection (PJI). In such cases, a two-stage exchange utilizing an antibiotic-loaded cement spacer is mandatory. Anatomically, a fluted stem is contraindicated when the femoral canal is excessively capacious or "stovepipe" in nature (Paprosky Type IV), where the distal diaphysis is so ectatic that a tapered stem cannot achieve cortical engagement without catastrophic subsidence. Similarly, if the required diaphyseal fixation extends into the distal femoral condyles, alternative reconstructive options such as tumor megaprostheses or allograft-prosthesis composites must be considered.
Indications and Contraindications Matrix
| Parameter | Indications for Fluted Tapered Stems | Absolute & Relative Contraindications |
|---|---|---|
| Bone Defect Classification | Paprosky Type IIIA, Type IIIB | Paprosky Type IV (Ectatic/Stovepipe canal without isthmus) |
| Periprosthetic Fracture | Vancouver Type B2, Vancouver Type B3 | Vancouver Type A (Trochanteric only), Vancouver Type C (Well below stem) |
| Infection Status | Aseptic loosening, Second-stage re-implantation | Active Periprosthetic Joint Infection (PJI) |
| Anatomical Considerations | Severe metaphyseal bone loss, Proximal deformity requiring ETO | Inadequate distal bone stock (< 2cm bypass available), Distal femoral non-union |
| Patient Factors | High functional demand requiring durable cementless fixation | Medically unstable for prolonged complex reconstruction |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a complex revision utilizing a fluted stem is largely predetermined in the preoperative planning phase. A meticulous clinical evaluation is the foundation. The character of the patient's pain must be dissected; "start-up" pain that localized to the thigh and resolves after ambulation is the hallmark of a loose femoral stem. Conversely, relentless pain at rest or night pain should immediately raise the index of suspicion for an indolent periprosthetic joint infection. A thorough physical examination must quantify leg length discrepancy (LLD), assess abductor competence via the Trendelenburg test, and evaluate the soft tissue envelope for prior incisions and skin quality.

Radiographic evaluation requires high-quality, properly scaled imaging. An AP pelvis, AP and cross-table lateral of the hip, and full-length AP and lateral views of the entire femur are mandatory. The full-length views are critical to assess the anterior bow of the femur, the endosteal diameter at the isthmus, and the total length of the femoral canal. We must identify the lowest extent of the osteolytic defect or fracture line. The fundamental biomechanical rule of revision stem fixation dictates that the new implant must bypass the most distal cortical defect by a minimum of two cortical diameters (typically 4 to 6 centimeters) to prevent stress risers and subsequent peri-prosthetic fractures.

Templating is an exacting science. Using digital templating software calibrated with a radiographic marker, we first establish the center of rotation on the acetabular side. Next, we address the femur. We template the distal stem size by matching the taper to the diaphyseal isthmus, ensuring the stem achieves cortical contact over a distance of at least 3 to 4 centimeters. We must carefully evaluate the anterior bow on the lateral radiograph; a straight, long stem inserted into a highly bowed femur will inevitably result in anterior cortical perforation. Once distal fixation is planned, we utilize the modular proximal bodies to template the restoration of offset, leg length, and version, referencing off the contralateral normal hip or established pelvic landmarks.

Patient positioning in the operating theater must facilitate extensive exposure and intraoperative fluoroscopy. The patient is typically placed in the lateral decubitus position and secured with rigid pelvic positioners to prevent shifting during aggressive reaming and impaction. The entire operative leg is draped free to allow for dynamic assessment of leg length, offset, and stability. Crucially, an image intensifier (C-arm) must be draped and readily available. Intraoperative fluoroscopy is indispensable for verifying guide wire placement, assessing reamer depth, confirming the bypass of cortical defects, and ensuring the final stem is seated without inducing occult diaphyseal fractures.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach must be extensile and adaptable. While a standard posterior approach is frequently utilized, the presence of severe proximal bone loss, retained cement, or a varus remodeled proximal femur often necessitates an Extended Trochanteric Osteotomy (ETO). The ETO is a powerful technique that provides unparalleled access to the femoral diaphysis, facilitates the safe extraction of well-fixed distal cement or broken stems, and allows for the correction of proximal deformity. The osteotomy is typically planned 12 to 15 centimeters distal to the tip of the greater trochanter, utilizing an oscillating saw and osteotomes while meticulously preserving the muscular pedicle (vastus lateralis and gluteus medius) to ensure viability and subsequent healing.

Once the femur is exposed and the failed components and all particulate debris/cement are meticulously debrided, diaphyseal preparation commences. This is the most critical technical step. We begin with a rigid reamer or a high-speed burr to clear the canal and establish a straight trajectory, bypassing any eccentric wear patterns. Sequential reaming is then performed. For fluted tapered stems, conical reamers are utilized to machine the diaphysis to match the exact geometry of the implant taper. The surgeon must rely on tactile feedback; reaming continues until continuous cortical "chatter" is felt, indicating that the reamer has engaged the endosteal cortex circumferentially. Prophylactic cerclage cables are frequently placed distal to the ETO or around areas of thinned cortex prior to final reaming and impaction to prevent hoop-stress induced fractures.
With the diaphysis prepared, the trial distal stem is inserted. It should seat firmly with manual pressure or light mallet taps. If the trial stem sinks below the planned depth, the canal has been over-reamed, and a larger diameter stem must be selected. Once distal stability is confirmed, the modular proximal trial body is assembled. This is where the true advantage of modularity shines. The surgeon can independently adjust the version of the proximal body (typically 10 to 15 degrees of anteversion) without altering the distal fixation. Trial reductions are performed to assess leg length, offset, and stability in extreme ranges of motion (flexion/internal rotation and extension/external rotation).

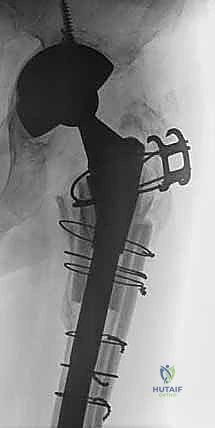
Final implantation requires meticulous attention to the modular junction. The taper of the definitive distal stem and the internal bore of the proximal body must be surgically clean and completely dry to prevent third-body wear, fretting, and cold-welding failure. The distal stem is impacted until the auditory pitch of the mallet strikes changes to a high-frequency resonance, indicating rigid seating. The proximal body is then applied at the predetermined version and impacted forcefully to engage the Morse taper. If an ETO was performed, the osteotomized fragment is reduced and secured around the new implant utilizing multiple cerclage cables, ensuring rigid fixation to promote osseous union.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, revision THA with fluted stems carries a significantly higher complication profile than primary arthroplasty. Intraoperative periprosthetic fracture is a constant threat, occurring in up to 10-15% of cases. The very mechanism that provides stability—compressive hoop stresses generated by the tapered geometry—can split a compromised diaphysis. Immediate recognition is vital. If a longitudinal split occurs during impaction, the stem must be assessed for stability. If stable, the fracture is managed with multiple cerclage cables. If unstable, a longer stem bypassing the fracture by two cortical diameters, supplemented with strut allografts and cabling, is mandated.
Postoperative subsidence is the most common early complication. A degree of "stable subsidence" (2-5 mm) is expected as the tapered stem settles into the viscoelastic bone under cyclical loading. However, progressive subsidence exceeding 10 mm or subsidence accompanied by varus tilt indicates failure of fixation. This usually results from undersizing the stem, inadequate reaming, or placing the stem in a Paprosky Type IV canal. Management of symptomatic, progressive subsidence requires re-revision to a larger diameter stem, a longer stem engaging more distal bone, or conversion to an impaction grafting technique or tumor prosthesis if diaphyseal bone is exhausted.

Instability and dislocation remain a major cause of failure, with rates ranging from 5% to 15%. This is primarily driven by the severe abductor deficiency and soft tissue compromise inherent to multiple revision surgeries. If an ETO fails to heal or the abductors are avulsed, the hip is at extreme risk. Management involves a stepwise approach: optimizing component position, utilizing large-diameter femoral heads, or upgrading to dual-mobility articulations. In cases of profound, irreparable abductor deficiency, a constrained acetabular liner may be the only viable salvage option to maintain the hip enlocated, albeit at the cost of reduced range of motion and higher long-term failure rates of the acetabular component.
Complications and Salvage Management Table
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Intraoperative Fracture | 5% - 15% | Excessive hoop stresses, Bowed femur mismatch, Osteopenic bone | Prophylactic cabling, Strut allografts, Longer bypass stem |
| Postoperative Subsidence | 10% - 20% | Undersized stem, Ectatic canal (Type IV), Inadequate cortical engagement | Observation if stable (<5mm); Re-revision to larger/longer stem if progressive |
| Dislocation / Instability | 5% - 15% | Abductor deficiency, ETO non-union, Component malposition | Dual-mobility constructs, Constrained liners, Abductor reconstruction |
| Modular Junction Failure | < 1% | Fretting corrosion, Contaminated taper, High BMI | Extraction and revision of components; requires pristine taper assembly |
| Infection (PJI) | 2% - 5% | Prolonged OR time, Massive soft tissue dissection, Prior surgeries | Two-stage revision with antibiotic spacer, Suppressive antibiotics |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a complex revision with a fluted stem must be highly individualized, striking a delicate balance between promoting early mobilization to prevent medical complications and protecting the precarious biomechanical construct to allow for osteointegration and fracture healing. The immediate postoperative phase (0 to 2 weeks) focuses on joint protection and DVT prophylaxis. Weight-bearing status is heavily dependent on the intraoperative assessment of stem stability and the presence of an ETO. If excellent diaphyseal scratch fit is achieved without an ETO, patients may be allowed toe-touch weight bearing (TTWB) or up to 50% partial weight bearing (PWB). If an ETO or structural allograft was utilized, strict TTWB is enforced to prevent shear forces from disrupting the osteotomy site.
During the intermediate phase (2 to 6 weeks), radiographic surveillance is critical. An AP pelvis and full-length femur radiograph are obtained at the 2-week and 6-week marks to assess for early subsidence, implant migration, or hardware failure. Physical therapy focuses on isometric strengthening of the quadriceps and gluteal musculature. Active abduction is strictly prohibited if an ETO or trochanteric repair was performed, to prevent avulsion of the repair. Patients are educated on strict posterior or anterior hip precautions, depending on the surgical approach utilized, to mitigate the high risk of early dislocation.
The advanced phase (6 to 12 weeks) marks the transition to functional recovery. Assuming radiographic evidence of ETO consolidation and stable implant positioning, weight-bearing is progressively advanced to full weight-bearing as tolerated. Assistive devices (walkers, then canes) are systematically weaned. Therapy shifts toward dynamic kinetic chain exercises, gait normalization, and active abductor strengthening against gravity and eventually resistance. Pool therapy can be highly beneficial during this phase to reduce joint reactive forces while allowing for extensive range of motion and muscle conditioning.
Long-term surveillance is a lifelong commitment for the revision THA patient. Patients are evaluated annually or biennially with clinical exams and radiographs. We meticulously scrutinize the bone-implant interface for signs of spot welds (indicating successful osteointegration), stress shielding (proximal bone resorption due to distal load transfer), or the reappearance of radiolucent lines and osteolysis. The modular titanium fluted stem has proven highly durable, but the orthopedic surgeon must remain vigilant for late complications, ensuring the longevity of this complex reconstruction.
Summary of Landmark Literature and Clinical Guidelines
The evolution and validation of the fluted tapered stem in revision THA are firmly rooted in decades of rigorous clinical research. Early literature was dominated by the monolithic Wagner stem. Landmark studies in the 1990s demonstrated that this 2-degree tapered, fluted titanium stem could successfully bypass massive proximal bone defects and achieve reliable diaphyseal fixation, boasting survivorship rates exceeding 90% at 10 years for aseptic loosening. However, these monolithic designs were plagued by a high incidence of postoperative dislocation, as the surgeon was forced to compromise proximal version and offset to achieve optimal distal diaphyseal fit.
The advent of modularity revolutionized this technique. Seminal papers by authors such as Sporer and Paprosky in the early 2000s highlighted the biomechanical and clinical advantages of modular fluted tapered stems. Their research demonstrated that by uncoupling distal fixation from proximal geometry, surgeons could independently optimize leg length, offset, and version, thereby dramatically reducing the dislocation rates associated with monolithic designs. Long-term follow-
