Acetabular Impaction Allografting: A Masterclass in Revision Total Hip Arthroplasty

Key Takeaway
Join our masterclass on acetabular impaction allografting for revision total hip arthroplasty. This immersive guide covers comprehensive surgical anatomy, meticulous preoperative planning, and granular, step-by-step intraoperative execution. We'll explore critical pearls, potential pitfalls, and strategies for managing postoperative rehabilitation and complications, ensuring optimal outcomes in complex acetabular bone loss cases.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to a critical and advanced session in the operating theater. Today, we confront one of the most demanding and complex challenges in adult joint reconstruction: the management of severe acetabular bone loss in the setting of revision total hip arthroplasty (THA). This is not merely a technical exercise in carpentry; it is a profound testament to our comprehensive understanding of pelvic biomechanics, osteoimmunology, bone biology, and meticulous surgical execution. Acetabular bone loss can arise from a myriad of etiologies—high-energy trauma, severe developmental dysplasia of the hip (DDH), oncologic resection, and periprosthetic joint infection (PJI). However, the most ubiquitous culprit we face is implant loosening secondary to particulate wear debris and the ensuing macrophage-mediated osteolysis.
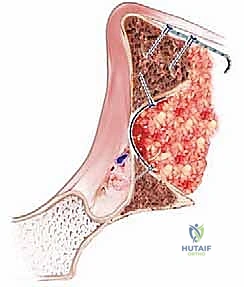
Traditional primary reconstruction methods, such as hemispherical uncemented components, often fall catastrophically short in restoring the structural integrity and biological potential of the acetabulum when faced with significant cavitary or segmental defects. Our strategy today, acetabular impaction allografting (AIA), offers a robust, biologically active solution. Pioneered by the Exeter group and further refined by Slooff and Ling, the principle is elegant yet mechanically powerful: we utilize tightly impacted, well-contained, morselized cancellous bone graft to restore native bone stock. This provides immediate mechanical stability for a cemented all-polyethylene implant and, crucially, promotes long-term bone remodeling and biological incorporation. This technique allows us to rebuild a functional neoacetabulum, re-establishing the native anatomic hip center and restoring normal hip abductor biomechanics.
The patho-epidemiology of periprosthetic osteolysis is a cascade of biological events that we must understand to truly appreciate the value of AIA. Particulate debris—traditionally polyethylene, but also metal or cement—is phagocytosed by macrophages, which then release a storm of pro-inflammatory cytokines, including TNF-alpha, IL-1, IL-6, and PGE2. This cascade upregulates RANKL expression, driving intense osteoclastic bone resorption. The result is a progressively expanding lytic lesion that compromises the supportive columns of the acetabulum. By the time the patient presents with mechanical failure and pain, the remaining host bone is often a sclerotic, devascularized shell. AIA directly addresses this by replacing the lytic void with an osteoconductive scaffold.
Let us briefly touch upon the biological underpinnings of impaction grafting. Animal studies, and indeed human biopsy specimens obtained years post-procedure, consistently demonstrate that impacted, morselized fresh-frozen allograft bone undergoes a remarkable process of incorporation known as creeping substitution. Histology reveals rapid revascularization of the graft bed, followed by osteoclastic resorption of the allograft and the simultaneous deposition of woven bone on the graft remnants by host osteoblasts. Over time, in accordance with Wolff's Law, this mixture of graft, new bone, and fibrin remodels into a new, functional trabecular structure, eventually resembling normal lamellar bone. However, we must acknowledge that localized areas of non-incorporated bone graft surrounded by fibrous tissue can persist, particularly if large, cartilaginous fragments are inadvertently included or if initial mechanical stability is not achieved.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of pelvic and acetabular anatomy is the bedrock of successful revision surgery. The acetabulum is formed by the confluence of the ilium, ischium, and pubis, structurally represented by the anterior and posterior columns—an inverted "Y" configuration that dictates load transfer from the axial skeleton to the lower extremity. The anterior column extends from the iliac crest to the pubic symphysis, while the massive posterior column extends from the sciatic notch to the ischial tuberosity. In severe osteolysis, the structural integrity of these columns is compromised. The medial wall, or cotyloid fossa, is naturally thin and highly susceptible to central migration of a failed implant, leading to protrusio acetabuli. During revision, identifying the true acetabular floor using the transverse acetabular ligament is critical for re-establishing the correct anatomical center of rotation (COR).
Neurovascular proximity makes acetabular revision fraught with peril. The sciatic nerve, exiting the greater sciatic notch and passing posterior to the short external rotators, is at constant risk during posterior exposure, retractor placement, and manipulation of the posterior column. Superiorly, the superior gluteal nerve and artery exit the pelvis just above the piriformis. Subperiosteal dissection along the superior dome and the placement of superior rim mesh must be executed with extreme caution to avoid catastrophic denervation of the gluteus medius and minimus, which would result in a permanent Trendelenburg gait. Medially, profound protrusio defects place the obturator nerve and external iliac vessels at risk during aggressive debridement or errant screw placement.
Biomechanically, the goal of any revision THA is the restoration of the native hip COR. A superiorly and laterally displaced hip center—often the path of least resistance in uncontained superior defects—dramatically shortens the abductor moment arm. This necessitates increased abductor muscle force to maintain pelvic level during the stance phase of gait, thereby exponentially increasing the joint reactive forces across the new implant and predisposing it to early accelerated wear and loosening. Acetabular impaction grafting allows the surgeon to physically build the bone back down to the anatomical COR, restoring the biomechanical advantage of the abductor musculature and normalizing joint reactive forces.
The biomechanics of the AIA construct itself are highly unique. The impacted morselized graft acts as a viscoelastic foundation. When a high-viscosity cement is pressurized into this graft, it interdigitates to a depth of 3 to 5 millimeters, creating a composite material of cement and cancellous bone. This composite distributes physiological loads evenly across the entire host bone bed, avoiding the stress shielding often seen with rigid, stiff metallic implants. The immediate stability of the cup relies entirely on the shear strength of the impacted graft and the radial compressive forces generated during impaction and cementation. If the graft is not aggressively impacted into a fully contained defect, the construct will fail mechanically before biological incorporation can occur.
Exhaustive Indications and Contraindications
Patient selection and defect classification are paramount. Acetabular impaction allografting is highly versatile but requires precise indications to ensure survivorship. We routinely utilize the Paprosky classification system to define the severity of bone loss and guide our reconstruction strategy. AIA is ideally suited for Paprosky Type II defects (distorted hemisphere but intact columns) and Paprosky Type IIIa defects (severe superior migration with intact inferior supportive structures). In these scenarios, the remaining host bone can provide the necessary containment and counter-pressure required for aggressive graft impaction.
When facing Paprosky Type IIIb defects (severe superior and medial migration with compromised columns) or true pelvic discontinuity, AIA alone is biomechanically insufficient. In these catastrophic failure modes, the impacted graft cannot provide initial structural stability. Therefore, AIA must be augmented with rigid internal fixation, typically utilizing an acetabular reconstruction cage (e.g., Burch-Schneider cage) or custom triflange components. The cage bridges the discontinuity and protects the graft from shear forces, allowing the impaction grafting to serve purely as a biological void filler to restore bone stock for future interventions, rather than as the primary structural support.
Contraindications to impaction grafting must be strictly observed. Active periprosthetic joint infection is an absolute contraindication; placing massive amounts of avascular allograft into an infected bed guarantees failure and systemic sepsis. Relative contraindications include severe pelvic irradiation, which obliterates the local microvasculature and host osteoprogenitor cells, rendering biological incorporation of the graft impossible. In such cases, cemented fixation into the irradiated bone or highly porous metal augments are preferred. Furthermore, severe systemic immunocompromise or profound malnutrition will severely blunt the creeping substitution process, leading to long-term graft resorption rather than incorporation.
Age and patient activity level also play a critical role in decision-making. While AIA is biologically appealing for younger patients because it restores bone stock for inevitable future revisions, the immediate mechanical limitations of the construct must be respected. Highly active, heavy patients may place excessive shear stress on the healing graft before incorporation is complete, leading to early catastrophic subsidence. In such demographics, the surgeon must weigh the biological benefits of AIA against the immediate rigid fixation offered by highly porous trabecular metal jumbo cups or custom implants.
| Parameter | Indications for Impaction Grafting | Contraindications for Impaction Grafting |
|---|---|---|
| Bone Defect Type | Paprosky Type II, Paprosky Type IIIa | Uncontained Paprosky IIIb (without cage) |
| Pelvic Integrity | Intact columns, contained cavitary defects | Pelvic Discontinuity (absolute without cage) |
| Infection Status | Aseptic loosening, cleared 2-stage revision | Active or suspected periprosthetic infection |
| Host Biology | Viable, bleeding host bone bed | Severe radiation necrosis, severe osteoporosis |
| Patient Factors | Need for bone stock restoration (younger age) | Non-compliant with weight-bearing restrictions |
Pre-Operative Planning, Templating, and Patient Positioning
Success in revision hip surgery is definitively determined long before the first incision is made. Our preoperative planning must be meticulous, comprehensive, and uncompromising. We begin with a thorough history, detailing the patient's journey: previous surgical approaches, the original primary diagnosis, the timeline of symptoms leading to failure, any history of prior wound healing issues or infections, and a complete review of systemic comorbidities. On physical examination, we meticulously assess previous incisions for quality and impending skin compromise. The presence of a sinus tract is highly suggestive of deep infection and mandates aggressive preoperative investigation. We quantify leg-length discrepancy (LLD), assess abductor function via the Trendelenburg test, and establish a baseline neurovascular status of the affected limb.
Diagnostic imaging is the cornerstone of our preoperative strategy. We obtain standard high-quality AP pelvis, AP, and cross-table lateral radiographs of the affected hip, alongside Judet views (iliac and obturator obliques) to assess the integrity of the anterior and posterior columns. However, plain radiographs notoriously underestimate the true volumetric extent of acetabular osteolysis. Therefore, a fine-cut Computed Tomography (CT) scan with Metal Artifact Reduction Sequence (MARS) is absolutely invaluable. The CT scan allows us to define the precise three-dimensional morphology of the bone loss, differentiate between contained cavitary and uncontained segmental defects, and definitively assess the integrity of the medial wall and the pelvic columns.
A rigorous preoperative work-up for periprosthetic joint infection is non-negotiable in every single revision case. We routinely obtain a complete blood cell count with differential (CBC), Erythrocyte Sedimentation Rate (ESR), and C-Reactive Protein (CRP). If any laboratory values are elevated or clinically suspicious, a fluoroscopic-guided aspiration of the hip joint must be performed. The aspirate is analyzed for cell count, polymorphonuclear percentage, alpha-defensin, and extended cultures (aerobic, anaerobic, fungal, and acid-fast bacilli). Proceeding with an elective biological reconstruction like AIA in the face of an undiagnosed, smoldering infection is a catastrophic error that will result in massive graft failure.
Precise preoperative templating is necessary to execute the reconstruction. Our primary goal is to restore the acetabular component to its true anatomic position. We utilize digital templating software to estimate the size of the definitive all-polyethylene cup, the required restoration of offset, and the volumetric amount of bone graft required. For extensive defects, we must ensure the bone bank has an adequate supply of fresh-frozen femoral heads (often requiring 2 to 4 heads per case). Patient positioning is typically in the lateral decubitus position, utilizing a rigid pelvic positioner or peg-board system to ensure absolute pelvic stability during aggressive graft impaction. The C-arm fluoroscopy unit must be positioned and tested prior to draping to ensure unimpeded AP and lateral views can be obtained intraoperatively without breaking the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
Exposure and Component Explantation
A wide, extensile exposure of the acetabulum is paramount. We routinely utilize a standard posterior approach, extending the previous skin incision. Deep dissection involves splitting the gluteus maximus fibers and carefully identifying the sciatic nerve, which is protected throughout the case. The short external rotators are tagged and released near their femoral insertions to expose the posterior capsule. A circumferential capsulotomy is performed, and the hip is dislocated. If a well-fixed femoral stem is present and impedes acetabular exposure, it must be protected; however, if exposure is critically compromised, a femoral osteotomy or stem explantation may be necessary.
Component explantation requires patience and specialized instrumentation. We utilize curved acetabular osteotomes, explant systems, and high-speed burrs to disrupt the implant-bone or implant-cement interface. The goal is to remove the failed component while meticulously preserving every millimeter of remaining host bone. Following implant removal, aggressive debridement is initiated. All fibrous tissue, granulomatous membranes, and necrotic bone must be excised using curettes and rongeurs until punctate bleeding bone is encountered. This bleeding host bed is the absolute prerequisite for graft revascularization and incorporation. If the host bone is profoundly sclerotic, we utilize a 2.0mm drill bit to create multiple fenestrations, accessing the underlying vascular marrow spaces to promote bleeding.
Host Bone Preparation and Defect Containment
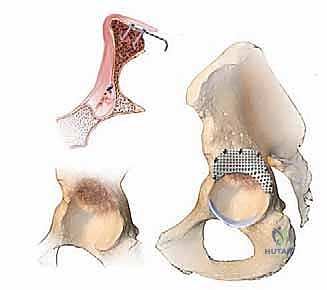
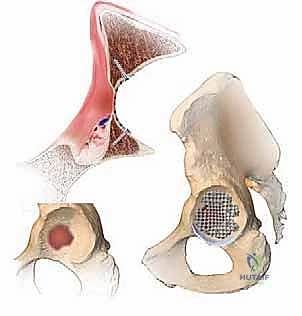
With the acetabulum debrided, we define the extent of the defects. The transverse acetabular ligament is identified inferiorly to establish the true acetabular floor. Segmental defects, particularly in the medial wall or the peripheral rim, must be converted into contained cavitary defects to allow for graft pressurization. This containment is achieved using flexible, pure titanium or stainless-steel wire mesh.
For medial wall defects (protrusio), the mesh is contoured to the defect and impacted medially. Often, the mesh is held in place by the subsequent graft impaction, but small unicortical screws can be utilized for initial stability. For peripheral rim defects, such as a superolateral deficiency, the mesh is applied to the outer cortex of the ilium and secured with multiple screws, effectively rebuilding the lateral wall of the acetabulum to contain the graft.
Graft Preparation and Impaction Mechanics
Simultaneous to the exposure, the back table team prepares the allograft. Fresh-frozen femoral heads are stripped of all cartilage and soft tissue. The bone is then passed through a bone mill to create morselized chips. The ideal chip size is critical—typically 8 to 10 millimeters. Chips that are too small lack structural interlocking capacity, while chips that are too large prevent adequate cement interdigitation. Crucially, the morselized graft must be thoroughly washed with pulsatile lavage to remove marrow, fat, and immunogenic elements. This washing step significantly improves the mechanical properties of the final graft-cement interface and reduces the risk of fat embolism during impaction.
The impaction process is the most technically demanding phase. We begin by placing the washed graft into the contained defect. Using specialized, graded acetabular impactors and a heavy mallet, the graft is vigorously and sequentially impacted.
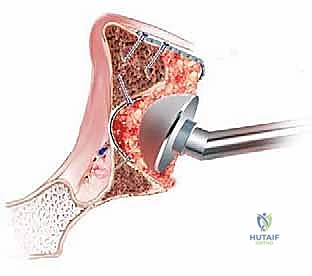
We start peripherally and work medially, building the neoacetabulum layer by layer. The impaction must be forceful enough to create a dense, interlocking matrix that feels structurally solid to a Cobb elevator. We frequently utilize a technique called "reverse reaming," where an acetabular reamer is run in reverse over the impacted graft to perfectly contour the hemispherical bed for the final implant, ensuring uniform cement mantle thickness.

Cementation and Component Insertion
Once the graft is densely impacted and contoured, we prepare for cementation. The graft bed is gently cleansed with a bulb syringe to remove surface blood, though aggressive pulsatile lavage at this stage is avoided to prevent disrupting the impacted architecture. We utilize a high-viscosity, radiopaque polymethylmethacrylate (PMMA) bone cement, often mixed with antibiotics (e.g., Tobramycin or Vancomycin) as prophylaxis.
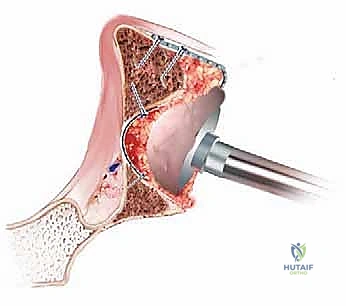
The cement is introduced in a doughy state. Crucially, profound pressurization is applied using a specialized acetabular seal and pressurizer. This sustained pressure forces the cement 3 to 5 millimeters into the interstices of the superficial graft layer, creating the essential composite micro-interlock. Following pressurization, the definitive all-polyethylene acetabular component is inserted. The cup is oriented in the standard 40-45 degrees of abduction and 15-20 degrees of anteversion. The cup pusher is held absolutely motionless with sustained pressure until complete exothermic polymerization of the cement is achieved.
Complications, Incidence Rates, and Salvage Management
The learning curve for acetabular impaction allografting is notoriously steep, and complications, particularly in the hands of inexperienced surgeons, can be catastrophic. Intraoperative complications primarily involve neurovascular injury or failure to achieve adequate initial construct stability. Aggressive manipulation of the posterior column or errant retractor placement can lead to sciatic nerve neuropraxia (incidence 1-3%). Superior dissection and mesh placement put the superior gluteal neurovascular bundle at risk. Furthermore, overzealous impaction in the setting of an unrecognized or inadequately meshed medial wall defect can result in intrapelvic extrusion of the bone graft and potentially fatal injury to the external iliac vessels.
Postoperatively, instability and dislocation represent the most frequent complication, with incidence rates ranging from 5% to 15% in complex revisions. This is often multifactorial, related to compromised abductor musculature, altered offset, or suboptimal cup positioning. Deep periprosthetic joint infection is a devastating complication (incidence 2-4%). Because the surgical site is loaded with avascular allograft, an infection will rapidly colonize the graft matrix, almost universally necessitating complete explantation of the construct, aggressive debridement, and placement of an antibiotic spacer.
Aseptic loosening and massive graft resorption are the primary long-term modes of mechanical failure. If the graft fails to incorporate—due to poor host biology, inadequate initial stability, or immunological rejection—it will gradually resorb, leading to massive cup subsidence and catastrophic failure. Salvage options for a failed AIA are extremely limited and technically daunting. Because the bone stock has typically been further compromised, salvage usually mandates the use of custom 3D-printed triflange acetabular components, massive structural allografts with cup-cage constructs, or, in the most dire circumstances, a permanent resection arthroplasty (Girdlestone procedure).
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management Options |
|---|---|---|---|
| Dislocation | 5% - 15% | Restore offset, precise cup version, larger femoral heads | Bracing, constrained liners, dual mobility constructs |
| Aseptic Loosening / Subsidence | 3% - 10% (at 10 yrs) | Vigorous impaction, strict defect containment, rigid mesh | Custom triflange, cup-cage construct, re-revision |
| Periprosthetic Infection | 2% - 4% | Strict pre-op screening, antibiotic cement, lavage | 2-stage revision, aggressive debridement |
| Sciatic Nerve Palsy | 1% - 3% | Careful posterior retraction, avoid over-lengthening | AFO bracing, physical therapy, neurolysis (rare) |
| Intrapelvic Graft Extrusion | < 1% | Secure medial mesh, careful medial impaction force | Vascular surgery consult, retroperitoneal exploration |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following acetabular impaction allografting requires a delicate, highly supervised balance. The surgeon must facilitate early patient mobilization to prevent cardiopulmonary and thromboembolic complications while strictly protecting the healing allograft from excessive shear and compressive forces that could induce early subsidence before biological incorporation occurs.
Phase I of rehabilitation encompasses the first 0 to 6 weeks postoperatively. During this critical window, the mechanical stability of the construct relies entirely on the frictional fit of the impacted graft and the cement interdigitation. Patients are restricted to strictly Toe-Touch Weight-Bearing (TTWB) or, at maximum, 20 pounds of flat-foot partial weight-bearing with the use of a walker or bilateral crutches. Active hip abduction is strictly prohibited to prevent massive compressive forces across the superior dome. Physical therapy focuses on isometric quadriceps and gluteal sets, ankle pumps, and safe transfer techniques adhering to standard posterior hip precautions (no flexion past 90 degrees, no adduction across the midline, no internal rotation).
Phase II spans from 6 to 12 weeks. At the 6-week mark, comprehensive radiographic evaluation is performed to assess for any early component migration or graft subsidence. If the construct remains radiographically stable, the patient is permitted to gradually advance their weight-bearing status, typically progressing by 25% body weight per week until full weight-bearing is achieved. Active-assisted and gentle active range of motion exercises are initiated. Pool therapy is highly beneficial during this phase, allowing for buoyancy-assisted gait training and gentle abductor strengthening.
Phase III, from 3 months to 1 year, focuses on maximizing functional recovery and long-term surveillance. Patients are transitioned to a cane and eventually to unassisted ambulation as abductor strength normalizes. High-impact activities (running, jumping) remain permanently contraindicated to protect the longevity of the reconstruction. Annual radiographic surveillance is mandatory. The surgeon must meticulously evaluate the radiographs for signs of creeping substitution—evidenced by the blurring of the distinct allograft chips and the formation of continuous trabecular lines bridging the host-graft interface—and monitor for any progressive radiolucent lines indicating failure of incorporation.
Summary of Landmark Literature and Clinical Guidelines
The foundation of modern acetabular impaction allografting rests upon the seminal work of the Exeter group in the United Kingdom, specifically the pioneering efforts of Slooff, Ling, and Gie in the 1980s. Their early publications established the fundamental principles of defect containment, rigorous morselization, and aggressive impaction, shifting the paradigm from merely bridging bone defects to actively restoring bone stock. Their initial cohorts demonstrated that biological incorporation of massive allografts was not only possible but reproducible when precise mechanical principles were adhered to.
Long-term survivorship data for AIA is highly encouraging when applied to appropriately selected patients. Extensive registry data, particularly from the Swedish Hip Arthroplasty Register and long-term cohort studies from specialized revision centers, demonstrate 15- to 20-year survivorship rates free from aseptic loosening ranging from 80% to 90%. Schreurs et al. published landmark 15-to-20-year follow-up data showing excellent maintenance of bone stock and stable clinical outcomes, cementing AIA as a gold-standard technique for cavitary and contained segmental defects.
Radiographic evaluation of graft incorporation remains a subject of intense academic study. The criteria established by Conn and Volz are frequently utilized to assess the success of the graft. Successful incorporation is characterized by an initial radiodensity of the graft, followed by a transient period of relative radiolucency (representing osteoclastic resorption and revascularization), and ultimately the re-establishment
