How We Tackled Massive Bone Loss in a Revision Hip Arthroplasty

Key Takeaway
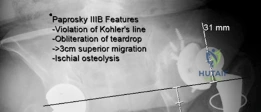
We review everything you need to understand about How We Tackled Massive Bone Loss in a Revision Hip Arthroplasty. A Paprosky IIIB defect signifies severe acetabular massive bone loss, typically seen in revision total hip arthroplasty. It's characterized by >3 cm superior migration of the hip center, significant ischial osteolysis exceeding 15mm, violation of Kohler's line, and obliteration of the teardrop. This complex defect often requires specialized reconstruction due to the extensive bony compromise.
A 72-year-old patient presents with a painful, stiff hip following a primary arthroplasty performed 15 years ago. On examination, there is a limb length discrepancy and significant Trendelenburg gait. Radiographs show significant acetabular and femoral osteolysis. Please describe the radiographic classification systems used to categorize this bone loss and why they are clinically relevant.

Candidate: I would use the Paprosky classification for both the acetabulum and the femur. For the acetabulum, it classifies the severity based on column integrity and migration. For the femur, it looks at metaphyseal loss and the amount of intact diaphyseal bone remaining. These are relevant because they dictate the type of reconstruction needed—for example, whether I can use a standard cup or need augments/custom implants, and whether a standard or modular fluted stem is appropriate.
Candidates often just list the classification numbers without defining the landmarks (teardrop, Kohler's line, isthmus). They also fail to mention that plain radiographs often underestimate the bone loss and don't advocate for CT/MARS imaging, which is the current standard for surgical planning in massive defects.
Start by categorizing the Paprosky system. Acetabulum: Type I (minimal), II (distorted but columns intact), III (compromised columns/migration). Mention Type IIIA (up and out) vs IIIB (up and in/pelvic discontinuity). Femoral: Type I-IV, focusing on the 4cm isthmus rule for diaphyseal fixation. Crucially, state that while radiographs are the primary tool, a CT scan with MARS is mandatory to assess column integrity and identify pelvic discontinuity, and mention that accurate classification is the prerequisite for selecting the reconstructive armamentarium (e.g., augments vs. CTAC vs. proximal femoral replacement).
During your revision, you encounter an acetabular Paprosky IIIB defect. Describe the biomechanical principles required to achieve stable fixation in this setting.
Candidate: In a IIIB defect, the columns are compromised. I need to achieve rigid fixation, ideally by restoring the anatomic center of rotation. I would use highly porous metal components, possibly with augments. If there is a pelvic discontinuity, I would use a cup-cage construct or a Custom Triflange Acetabular Component to span the defect and achieve fixation in the ilium and ischium.
Neglecting the "Center of Rotation." Many candidates forget that lateral and superior migration of the hip center increases joint reactive forces and reduces the abductor moment arm. They also fail to mention the neurovascular risks (sciatic vs. obturator) associated with screw placement in the ischium or superior dome.
A high-scoring answer addresses: 1) Center of Rotation: Importance of restoring anatomical center to normalize biomechanics. 2) Biologic Fixation: Utilizing porous metal to promote bone ingrowth. 3) Mechanical Stability: Bridging the discontinuity (Cage vs. CTAC) to bypass the uncontained defect. 4) Neurovascular Safety: Explicitly mentioning the superior gluteal bundle (superiorly) and obturator nerve (inferiorly) during screw trajectory planning.
You have decided to perform an Extended Trochanteric Osteotomy (ETO) for a femoral revision. What are the key technical steps to ensure success and minimize the risk of nonunion?
Candidate: The ETO is essential for extensile exposure and safe implant removal. I would plan the length preoperatively to bypass the distal extent of the existing stem. I would reflect the fragment anteriorly while preserving the muscle attachments. Closure requires multiple cerclage cables to ensure rigid fixation against the femoral shaft.
Failing to mention the "distal scratch fit" requirement. The revision stem must bypass the ETO by 4-6 cm to achieve distal fixation. Also, failing to mention the protection of the abductor mechanism or the necessity of avoiding post-operative abduction for 6-8 weeks is a major omission.
Focus on: 1) Planning: Length must be sufficient to bypass the implant/defect. 2) Execution: Controlled osteotomy preserving the vascularity of the abductor/vastus lateralis cuff. 3) Distal Bypass: The revision stem must have 4-6cm of diaphyseal engagement distal to the osteotomy. 4) Reconstruction: Use of tensioned cerclage cables. 5) Rehab: Strict avoidance of active abduction for 6-8 weeks to protect the osteotomy union.
