Patellar Tendon Repair via Transosseous Drill Holes: A Comprehensive Surgical Guide
Key Takeaway
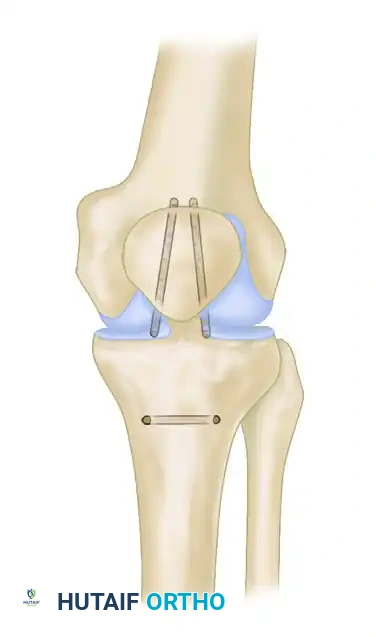
The transosseous drill hole technique remains a gold-standard approach for acute patellar tendon ruptures, particularly at the tendon-bone junction. This procedure involves creating a bony trough at the inferior patellar pole, passing heavy nonabsorbable sutures through longitudinal transosseous tunnels, and meticulously restoring patellar height. Proper execution prevents patella baja and restores extensor mechanism biomechanics, ensuring optimal functional recovery for the patient.
Comprehensive Introduction and Patho-Epidemiology
Disruption of the knee extensor mechanism via patellar tendon rupture is a profoundly debilitating orthopedic injury that mandates prompt, meticulous surgical intervention to restore normal ambulatory function. The extensor mechanism is an intricate, highly coordinated anatomical complex comprising the quadriceps musculature, the quadriceps tendon, the patella, the patellar tendon, and the adjacent medial and lateral retinacular structures. When the patellar tendon is acutely ruptured, the continuity of this biomechanical chain is severed, resulting in an immediate and catastrophic loss of active knee extension. Left untreated, or if managed suboptimally, this injury invariably leads to profound functional impairment, chronic patellofemoral pain, severe extensor lag, and early-onset secondary osteoarthritis of the patellofemoral joint.
Epidemiologically, patellar tendon ruptures present with a distinct demographic and mechanistic profile. They occur most frequently in male patients under the age of 40, contrasting with quadriceps tendon ruptures which predominantly affect individuals over the age of 40. The classic mechanism of injury involves a sudden, violent eccentric contraction of the quadriceps muscle against a fixed, flexed knee—such as landing awkwardly from a jump, abruptly decelerating during athletic competition, or stumbling on a descending stair. The massive tensile forces generated during this eccentric loading overwhelm the ultimate tensile strength of the tendon, leading to catastrophic failure. While high-energy trauma, such as motor vehicle collisions or direct high-velocity blows to the anterior knee, can also precipitate rupture, the eccentric overload mechanism remains the most prevalent etiology in clinical practice.
The pathophysiology of patellar tendon rupture is rarely an event occurring in a completely pristine, healthy tendon. Histopathological analyses of ruptured tendons consistently demonstrate pre-existing microvascular compromise and degenerative tendinosis at the site of failure. This underlying tendinopathy weakens the collagen matrix, predisposing the structure to acute mechanical failure under sudden load. Furthermore, several systemic and pharmacological risk factors significantly elevate the risk of rupture by altering collagen synthesis and degrading tendon architecture. These include systemic lupus erythematosus (SLE), rheumatoid arthritis, chronic renal failure, hyperparathyroidism, and diabetes mellitus. Pharmacologically, the prolonged use of systemic or local corticosteroids, as well as fluoroquinolone antibiotics, has been definitively linked to tendinous degeneration and subsequent spontaneous rupture.
While the advent of suture anchor constructs has introduced alternative fixation strategies in recent years, the classic transosseous drill hole repair remains a highly reliable, biomechanically robust, and cost-effective gold standard in operative orthopedics. This time-honored technique is predicated on the principle of biological healing, allowing the surgeon to dock the meticulously prepared tendon stump directly into a bleeding cancellous bone trough at the inferior pole of the patella. This direct tendon-to-bone interface, stabilized by heavy non-absorbable sutures passed through transosseous tunnels, creates an optimal environment for robust fibrovascular integration. This comprehensive guide details the precise surgical execution of the transosseous repair, emphasizing meticulous tissue handling, accurate restoration of patellar height, and advanced augmentation techniques for managing compromised or chronically retracted tissue.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the extensor mechanism's anatomy is the absolute prerequisite for executing a successful patellar tendon repair. The patellar tendon, despite its nomenclature, is anatomically a ligament, as it connects two osseous structures: the inferior pole of the patella and the tibial tubercle. In a healthy adult, the tendon averages approximately 30 mm in width, 4 to 5 mm in thickness, and roughly 40 to 50 mm in length. It is a dense, highly organized band of type I collagen fibers that originate from the non-articular apex of the patella and insert broadly onto the anterior aspect of the proximal tibia. The tendon is enveloped by a well-vascularized peritenon, which is critical for providing the blood supply necessary for healing following surgical repair or injury.
The vascular supply to the patellar tendon is segmental and highly specialized. The proximal and distal insertions receive osseous contributions, but the midsubstance is supplied primarily by the anastomotic ring formed by the inferior medial and inferior lateral genicular arteries. The infrapatellar fat pad (Hoffa's fat pad), situated immediately posterior to the tendon, also provides a vital vascular plexus. During surgical dissection, it is imperative to preserve the infrapatellar fat pad and the peritenon to the greatest extent possible to prevent avascular necrosis of the tendon stump and to optimize the biological healing environment. Innervation is supplied by branches of the femoral, obturator, and sciatic nerves, but surgically, the most critical neural structure is the infrapatellar branch of the saphenous nerve (IPBSN). This nerve frequently crosses the proximal tibia from medial to lateral, directly over the operative field. Iatrogenic transection or entrapment of the IPBSN can result in painful neuromas or persistent, bothersome numbness over the anterolateral aspect of the proximal leg.
Biomechanically, the patella functions as a highly efficient fulcrum, displacing the extensor mechanism anteriorly away from the center of rotation of the knee joint. This anterior displacement significantly increases the moment arm of the quadriceps muscle, enhancing its mechanical advantage by up to 50% during the initial degrees of knee extension. The patellar tendon must withstand extraordinary tensile forces to transmit this muscular effort to the tibia. During normal level walking, the tendon experiences forces equivalent to roughly 0.5 times body weight. However, during deep squatting, stair climbing, or athletic jumping, these forces can exponentially amplify to 7 or 8 times body weight. Consequently, any surgical repair must be biomechanically robust enough to withstand early cyclic loading during postoperative rehabilitation without gap formation at the repair site.
Patellofemoral kinematics are exquisitely sensitive to the resting length of the patellar tendon. The precise restoration of this length during surgery is the most critical determinant of long-term functional success. If the tendon is repaired with excessive tension, a condition known as patella baja (infera) ensues. Patella baja abnormally lowers the patella relative to the trochlear groove, severely altering patellofemoral contact pressures. This leads to accelerated, early-onset chondral wear, debilitating anterior knee pain, and a mechanical block to full flexion. Conversely, inadequate tensioning results in patella alta and a persistent extensor lag, significantly impairing gait efficiency and quadriceps function. Therefore, intraoperative assessment of patellar height using fluoroscopic landmarks, such as Blumensaat's line and the Insall-Salvati ratio, is an uncompromising necessity.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a suspected patellar tendon disruption relies on a meticulous clinical examination and appropriate radiographic interpretation. Complete, acute ruptures of the patellar tendon represent an absolute indication for prompt surgical repair. Clinically, these patients present with a palpable defect at the inferior pole of the patella, massive localized hemarthrosis, and a profound inability to perform an active straight leg raise (SLR) or maintain the knee in full active extension against gravity. Surgical intervention should ideally be performed within the first 1 to 2 weeks post-injury. Early intervention facilitates anatomical reduction before the onset of severe quadriceps contracture, extensive soft tissue scarring, and proximal retraction of the patella, which exponentially complicate the surgical reconstruction.
Relative indications for surgery include high-grade partial tears where the extensor mechanism is functionally compromised but not completely discontinuous. In highly active individuals or competitive athletes, even partial tears that demonstrate significant weakness or pain during eccentric loading may warrant surgical exploration and repair to prevent completion of the rupture and to restore peak athletic performance. Conversely, low-grade partial tears with an intact extensor mechanism (the patient can perform a pain-free, robust SLR) are typically managed conservatively with a period of immobilization in extension followed by a structured, progressive physical therapy program focused on eccentric strengthening.
Contraindications to immediate surgical repair are relatively few but clinically significant. Absolute contraindications include the presence of active, uncontrolled local or systemic infection, severe medical comorbidities that render the patient an unacceptable anesthetic risk (e.g., recent myocardial infarction, severe uncompensated heart failure), or a severely compromised anterior soft tissue envelope (e.g., extensive traumatic degloving, severe active cellulitis). In cases of compromised soft tissues, temporary immobilization with a spanning external fixator or a rigid knee immobilizer may be required until the soft tissue bed has adequately recovered to tolerate a surgical incision.
Relative contraindications revolve around chronicity and patient compliance. Chronic ruptures (presenting greater than 6 weeks post-injury) often feature severe quadriceps retraction, patella alta, and complete atrophy of the native tendon stump. While surgery is still indicated to restore function, these cases cannot typically be managed with a primary transosseous repair alone. They require complex reconstructive procedures utilizing massive allografts (e.g., Achilles tendon with bone block) or extensive autograft augmentation, often combined with quadriceps lengthening procedures (e.g., V-Y plasty). Furthermore, patients with severe cognitive impairment or those who are anticipated to be completely non-compliant with strict postoperative weight-bearing and range-of-motion restrictions pose a high risk for catastrophic repair failure, necessitating careful preoperative counseling and potentially the use of supplementary mechanical protection (e.g., cerclage wiring).
Summary of Indications and Contraindications
| Category | Specific Clinical Scenario | Surgical Recommendation / Management Strategy |
|---|---|---|
| Absolute Indications | Acute complete rupture, inability to perform SLR, palpable defect. | Immediate primary transosseous repair (ideally within 1-2 weeks). |
| Relative Indications | High-grade partial tear with functional weakness in athletes. | Surgical exploration, debridement, and primary repair or augmentation. |
| Conservative Management | Low-grade partial tear, intact SLR, minimal functional deficit. | Immobilization in extension, progressive eccentric rehabilitation. |
| Absolute Contraindications | Active local infection, severe medical instability, degloved soft tissue. | Delay surgery, manage medically, temporary rigid immobilization. |
| Relative Contraindications | Chronic neglected rupture (>6 weeks), severe non-compliance. | Complex allograft reconstruction required; consider mechanical augmentation. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a flawlessly executed patellar tendon repair. The diagnostic workup must begin with high-quality, orthogonal radiographs of the affected knee, including anteroposterior (AP) and true lateral views. The lateral radiograph is particularly diagnostic; it will almost universally demonstrate patella alta, confirming the complete disruption of the inferior tether of the extensor mechanism. The Insall-Salvati ratio (the ratio of the patellar tendon length to the greatest diagonal length of the patella) will be significantly elevated (>1.2). Radiographs are also essential for ruling out concurrent osseous pathology, such as tibial plateau fractures, distal femur fractures, or avulsion fractures of the tibial tubercle, which would necessitate a drastic alteration in the surgical plan.
While the diagnosis of a complete patellar tendon rupture is primarily clinical and radiographic, Magnetic Resonance Imaging (MRI) is highly beneficial and increasingly considered standard of care in the preoperative workup. MRI provides unparalleled soft-tissue resolution, allowing the surgeon to assess the exact anatomical location of the tear (proximal avulsion vs. midsubstance vs. distal avulsion), the degree of tendon retraction, and the quality of the remaining tendinous tissue. Furthermore, MRI is critical for identifying concurrent intra-articular pathology. Although isolated eccentric overload injuries rarely involve the cruciate ligaments or menisci, high-energy traumatic mechanisms can result in multiligamentous knee injuries that must be recognized and addressed either concurrently or in a staged fashion.
Preoperative patient optimization involves managing any systemic comorbidities and carefully timing the surgical intervention. While early surgery is advocated, allowing 24 to 48 hours for acute traumatic soft tissue swelling to subside can significantly reduce the risk of postoperative wound healing complications. During this waiting period, the limb should be immobilized in full extension and elevated. The surgical team must also ensure that all necessary equipment is available, including heavy non-absorbable sutures (#5 FiberWire or Ethibond), high-speed burrs, appropriate drill bits (2.5mm to 3.0mm), suture passers (Beath pins), and potential augmentation materials (allograft tissue or cerclage wire) should the intraoperative findings dictate a more complex reconstruction.
Patient positioning and anesthesia are critical for optimizing surgical exposure and facilitating intraoperative assessment of patellar tracking and tension. The procedure is typically performed under general anesthesia or regional spinal anesthesia. A regional nerve block, such as an adductor canal block, is highly recommended to provide excellent postoperative analgesia without causing profound quadriceps motor blockade, which could interfere with early postoperative rehabilitation. The patient is placed in the supine position on a standard radiolucent operating table to allow for intraoperative fluoroscopy. A well-padded pneumatic tourniquet is applied high on the proximal thigh. The surgical limb is prepped and draped in a standard sterile fashion, ensuring that the draping allows for full, unencumbered flexion and extension of the knee from 0 to 120 degrees. A sterile bump or a triangulated leg positioner can be utilized to maintain the knee in varying degrees of flexion during the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the transosseous patellar tendon repair demands meticulous attention to soft tissue handling, anatomical restoration, and biomechanical principles. The procedure begins with a generous longitudinal midline incision centered directly over the palpable defect, typically extending from the superior pole of the patella to approximately 2 centimeters distal to the tibial tubercle. This extensile approach is preferred over transverse incisions as it allows for unhindered proximal and distal extension should extensive mobilization of the quadriceps or harvesting of a hamstring autograft for augmentation become necessary. Subcutaneous dissection is performed sharply, raising full-thickness fasciocutaneous flaps to preserve the delicate vascularity of the overlying skin.
During the initial dissection, the surgeon must remain highly vigilant regarding the infrapatellar branch of the saphenous nerve (IPBSN). This nerve frequently crosses the operative field in the distal aspect of the incision. Meticulous identification, gentle mobilization, and retraction of the nerve out of harm's way are paramount. However, patients must be explicitly counseled preoperatively that some degree of altered sensation or numbness lateral to the incision is a highly probable, and often unavoidable, consequence of the surgical approach. Once the superficial fascia is cleared, the peritenon is incised longitudinally in the midline and carefully preserved. The massive hematoma typically encountered within the defect is evacuated, revealing the ruptured tendon ends and the invariably associated tears of the medial and lateral retinacula.
The preparation of the tendon stump and the bony footprint is the next critical phase. The rupture most commonly manifests as a proximal avulsion from the inferior pole of the patella. The distal stump is identified, grasped with a heavy clamp, and mobilized. Any frankly necrotic, severely contused, or completely devitalized tissue is sharply debrided; however, the surgeon must be exceedingly judicious to preserve as much functional tendon length as possible. Attention is then turned to the inferior pole of the patella. Using a rongeur or a high-speed burr, the remaining soft tissue footprint is cleared, and a small, horizontal cancellous bone trough is created. This trough exposes a bleeding, highly vascular bone bed that is absolutely critical for the biological integration and healing of the repaired tendon.
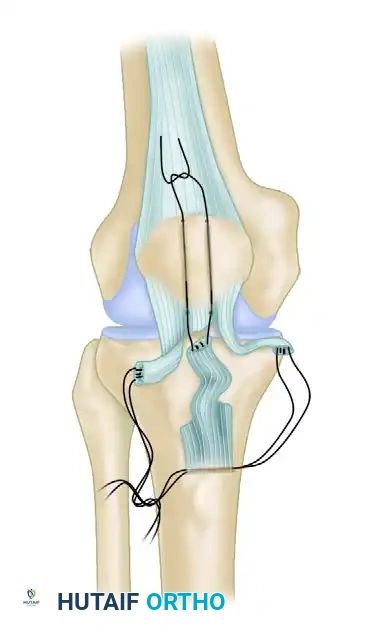
With the bony bed prepared, the heavy non-absorbable sutures are placed into the distal tendon stump. The preferred configuration involves placing two or three interlocking (Krackow or Bunnell type) running sutures using #5 braided non-absorbable material (e.g., FiberWire). These sutures are placed along the medial, central, and lateral thirds of the tendon, ensuring that the locking bites securely grasp the robust, healthy collagen bundles. Three parallel, longitudinal transosseous tunnels (typically 2.5 mm to 3.0 mm in diameter) are then drilled from the prepared bleeding trough at the inferior pole, exiting at the superior pole of the patella.
Utilizing a suture passer or a Beath pin, the free limbs of the heavy sutures are drawn proximally through the drilled osseous tunnels. This action anatomically reduces the tendon stump, docking it securely and intimately into the prepared cancellous trough.
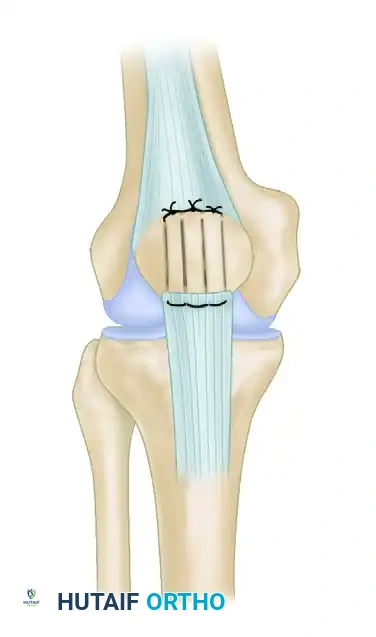
The tensioning and securing of the repair is arguably the most unforgiving step of the entire procedure. To prevent the catastrophic complication of patella baja, the knee must be flexed to exactly 45 degrees. At this angle of flexion, the patellar height is assessed utilizing Blumensaat's line (the roof of the intercondylar notch). A rigid straight edge or a hemostat is placed parallel to Blumensaat's line on the lateral aspect of the femoral condyle. The inferior pole of the patella should sit at, or just slightly proximal to, the level of this line. Intraoperative lateral fluoroscopy is highly recommended to confirm the Insall-Salvati ratio and ensure precise anatomical restoration. Once the correct tension is verified, the heavy sutures are tied securely over the superior pole of the patella, burying the bulky knots deep to the quadriceps tendon insertion to prevent post-operative hardware prominence and skin irritation.
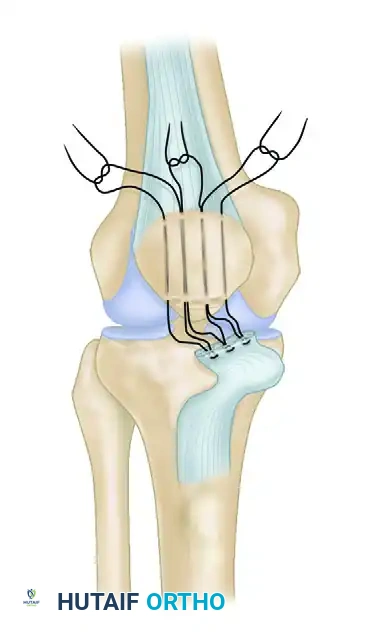
In scenarios involving extensively frayed tissue, delayed presentation, or midsubstance ruptures, advanced techniques are required. For severe fraying, the interlocking Krackow sutures must be extended further distally to capture competent tissue.
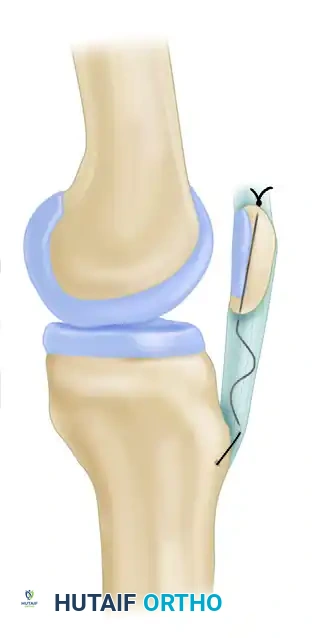
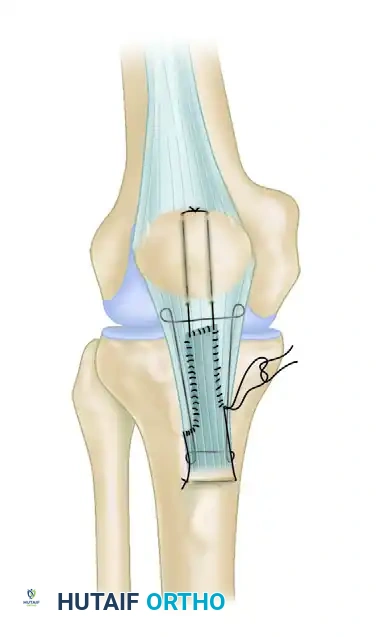
For true midsubstance ruptures, running interlocking sutures are placed in both the proximal and distal tendon stumps. These sutures are then secured through parallel vertical holes in the patella and a transverse drill hole in the tibial tuberosity, effectively bypassing the midsubstance defect and offloading the primary repair site.
Regardless of the specific technique utilized for the central tendon, the final, mandatory step of the procedure is the meticulous repair of the medial and lateral retinacula. These structures are repaired using #0 absorbable or #2 non-absorbable sutures. Robust retinacular repair is essential for restoring the coronal plane stability of the patella, ensuring normal patellofemoral tracking, and providing supplementary biomechanical support to the central tendon repair.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, patellar tendon repair carries a distinct profile of potential postoperative complications. The surgeon must be acutely aware of these risks, actively employ preventative intraoperative strategies, and possess the requisite knowledge to manage them should they arise. The most frequent complications include arthrofibrosis (stiffness), patellofemoral pain secondary to altered kinematics, re-rupture of the repaired tendon, and superficial or deep surgical site infections. The incidence of these complications is significantly influenced by patient factors (e.g., smoking, diabetes), the chronicity of the injury, and the specific postoperative rehabilitation protocol employed.
Arthrofibrosis, characterized by a persistent deficit in knee flexion and occasionally an extensor lag, is the most common complication, affecting up to 15-20% of patients. It is historically associated with prolonged periods of rigid postoperative immobilization in a cast. Modern rehabilitation protocols emphasizing early, controlled passive motion have significantly reduced the incidence of severe stiffness. However, if a patient fails to progress in physical therapy and exhibits severe arthrofibrosis at 3 to 6 months postoperatively, aggressive intervention is warranted. This typically involves an initial trial of manipulation under anesthesia (MUA), followed by arthroscopic lysis of adhesions and anterior interval release if the MUA is unsuccessful.
Patella baja (infera) is a devastating, largely iatrogenic complication resulting from over-tensioning the repair intraoperatively or secondary to severe postoperative scarring and contracture of the tendon. Patella baja dramatically increases patellofemoral contact forces, leading to accelerated chondral wear, debilitating anterior knee pain, and a mechanical block to flexion. Prevention is entirely dependent on meticulous intraoperative assessment of patellar height at 45 degrees of flexion using fluoroscopy. If severe, symptomatic patella baja develops and is refractory to conservative management, salvage procedures are complex. They may include tibial tubercle osteotomy with proximal translation (to restore the anatomical length of the extensor mechanism) or, in extreme cases of concurrent severe arthrosis, a complex total knee arthroplasty.
Re-rupture of the repaired patellar tendon is a catastrophic failure that occurs in approximately 2-5% of cases. It is most frequently precipitated by patient non-compliance with weight-bearing restrictions, an accidental fall during the early vulnerable phase of healing, or failure to recognize and augment severely compromised, degenerative tissue during the index procedure. Re-rupture necessitates a highly complex revision surgery. Primary repair is rarely feasible due to profound tissue retraction and poor biological quality. Revision strategies invariably require massive structural allografts, such as an Achilles tendon allograft with a calcaneal bone block, securely fixed into a prepared trough in the tibial tubercle and woven through the remaining quadriceps mechanism.
Complications and Salvage Strategies
| Complication | Estimated Incidence | Preventative Strategy | Salvage / Management Strategy |
|---|---|---|---|
| Arthrofibrosis (Stiffness) | 10 - 20% | Early controlled passive motion; avoid prolonged casting. | Aggressive physical therapy; Manipulation Under Anesthesia (MUA); Arthroscopic lysis of adhesions. |
| Patella Baja (Infera) | 5 - 10% | Tension repair strictly at 45° flexion; use intraoperative fluoroscopy. | Tibial tubercle proximalization osteotomy; complex patellofemoral arthroplasty if severe arthrosis present. |
| Re-Rupture | 2 - 5% | Robust fixation (Krackow sutures); strict adherence to rehab protocol; augment poor tissue. | Revision reconstruction using structural allograft (e.g., Achilles tendon with bone block). |
| Surgical Site Infection | 1 - 3% | Meticulous soft tissue handling; prophylactic antibiotics; optimize comorbidities. | Superficial: Oral antibiotics. Deep: Urgent surgical irrigation and debridement (I&D), retain hardware if repair is stable, IV antibiotics. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a transosseous patellar tendon repair is a delicate, highly structured progression. The overarching philosophy must continuously balance the absolute necessity of protecting the fragile, healing tendon-bone interface from excessive tensile loads with the equally critical need to initiate early motion to prevent debilitating arthrofibrosis. The historical paradigm of placing the patient in a rigid cylinder cast for six weeks has been largely abandoned in modern orthopedic practice due to the unacceptably high rates of severe, intractable stiffness and profound quadriceps atrophy. Current evidence-based protocols utilize hinged knee braces and emphasize early, heavily protected, controlled motion.
Phase I: Maximum Protection (Weeks 0 to 6)
Immediately following surgery, the operative limb is placed in a hinged knee brace locked in full, absolute extension. For the first two to three weeks, weight-bearing is typically restricted to toe-touch or partial weight-bearing with crutches, strictly with the brace locked in extension. This prevents any eccentric loading of the quadriceps, which could catastrophically pull through the fresh repair. At approximately week 2 or 3, once the surgical incisions have healed, controlled passive range of motion (PROM) is initiated under the strict supervision of a physical therapist. The brace is unlocked during therapy sessions to allow flexion from 0 to 45 degrees. Active extension is strictly prohibited to protect the repair. Isometric quadriceps sets and straight-leg raises (SLR) in the locked brace are initiated to prevent profound muscle atrophy. Flexion is gradually progressed by 10 to 15 degrees per week, aiming for 90 degrees of passive flexion by the end of week 6.
Phase II: Controlled Active Motion and Early Strengthening (Weeks 6 to 12)
At the 6-week mark, biological healing at the tendon-bone interface has progressed sufficiently to tolerate mild active forces. The patient is transitioned to weight-bearing as tolerated (WBAT) with the brace unlocked, provided they demonstrate excellent quadriceps control and no extensor lag during a straight leg raise. Active-assisted range of motion is initiated, and passive flexion is progressed towards full, symmetric range of motion. Closed kinetic chain exercises are cautiously introduced, starting with mini-squats (0 to 30 degrees) and leg presses with light resistance. Open kinetic chain active extension exercises (e.g., seated leg extensions) remain strictly prohibited, as they place massive shear forces across the repair site. Proprioceptive training and stationary cycling (initially with a high seat to limit deep flexion) are incorporated to enhance joint nutrition and neuromuscular control.
Phase III: Advanced Strengthening and Return to Function (Months 3 to 6+)
By the third postoperative month, the brace is typically discontinued entirely for activities of daily living. Rehabilitation shifts focus toward maximizing quadriceps strength, power, and endurance. Advanced closed kinetic chain exercises, step-ups, and functional movement patterns are emphasized. Jogging and light plyometrics may be introduced between months 4 and 5, contingent upon the patient demonstrating at least 70-80% quadriceps strength symmetry compared to the contralateral limb.
Phase IV: Return to Sport (Months 6 to 9+)
The final phase of rehabilitation is highly individualized and focuses on sports-specific agility and power generation. Return to high-impact, cutting, or jumping sports is generally delayed until 6 to 9 months postoperatively. Clearance for unrestricted athletic participation requires the patient to demonstrate a complete, pain-free range of motion
