Gastrocnemius Fascia Lengthening: An Intraoperative Masterclass for Equinus Deformity

Key Takeaway
Join us in the OR for a detailed masterclass on gastrocnemius fascia lengthening, a critical procedure for equinus deformities. We'll meticulously cover surgical anatomy, preoperative planning, precise intraoperative execution of Strayer, Baker, and Vulpius techniques, essential pearls and pitfalls, and comprehensive postoperative management to optimize patient outcomes and prevent recurrence.
Comprehensive Introduction and Patho-Epidemiology
Equinus deformity represents one of the most ubiquitous and biomechanically disruptive pathologies encountered in both pediatric and adult orthopaedic surgery. Defined strictly as a fixed or dynamic plantarflexion contracture of the ankle joint, equinus prevents the foot from achieving a neutral or dorsiflexed position relative to the tibia. This seemingly isolated joint restriction initiates a cascade of biomechanical compensations that profoundly alter the human gait cycle. Normal ambulation relies on the smooth progression of the foot through three distinct "rockers." An equinus contracture obliterates the first rocker (heel strike), forcing a forefoot or midfoot initial contact. Consequently, the tibia is driven posteriorly during the stance phase, which can precipitate secondary genu recurvatum (knee hyperextension) or, conversely, a compensatory crouch gait if concomitant hamstring contractures are present. Understanding these kinematic chain reactions is paramount before contemplating surgical intervention.
The etiology of equinus is broad, encompassing congenital, neuromuscular, post-traumatic, and idiopathic origins. In the pediatric realm, cerebral palsy (CP) remains the most frequent instigator. In spastic diplegia or hemiplegia, the upper motor neuron lesion leads to resting spasticity and a failure of longitudinal muscle growth. The muscle-tendon unit of the triceps surae becomes functionally, and eventually anatomically, shortened relative to the rapidly growing skeletal elements (tibia and fibula). However, the differential diagnosis must remain expansive. Idiopathic toe walking, while often a diagnosis of exclusion that may resolve spontaneously, can culminate in fixed contractures requiring surgical release in older children. Other neuromuscular disorders, such as Duchenne muscular dystrophy and Charcot-Marie-Tooth (CMT) disease, frequently present with equinus, though CMT often features a concomitant cavovarus deformity driven by a plantarflexed first ray rather than true hindfoot equinus.
Pathophysiologically, a fixed muscle contracture is not merely a "tight" muscle; it represents fundamental structural alterations at the cellular and extracellular levels. In spastic muscles, histological analyses reveal a significant reduction in serial sarcomere numbers, an accumulation of disorganized extracellular matrix, and profound fibrotic infiltration. The muscle fibers themselves become stiffer and less compliant. Furthermore, we must distinguish between absolute shortening of the triceps surae and relative shortening. Relative shortening often occurs iatrogenically following limb salvage procedures, such as distraction osteogenesis (Ilizarov tibial lengthening), where the bone is lengthened at a rate that exceeds the adaptive capacity of the spanning soft tissues.
Historically, the surgical management of equinus relied heavily on Tendo-Achilles Lengthening (TAL). However, the orthopaedic community has recognized the catastrophic functional consequences of over-lengthening the Achilles tendon, which frequently results in an iatrogenic calcaneal gait—a debilitating condition characterized by a complete loss of plantarflexion push-off power and progressive crouch. Consequently, the paradigm has shifted dramatically toward isolated gastrocnemius fascia lengthening (such as the Strayer, Vulpius, or Baker procedures) for patients with isolated gastrocnemius contractures. This masterclass will elucidate the precise anatomical, diagnostic, and technical nuances required to execute a flawless gastrocnemius lengthening, thereby restoring dorsiflexion while meticulously preserving the power of the soleus muscle.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the posterior calf anatomy is the bedrock of safe and effective equinus correction. The primary engine of ankle plantarflexion is the triceps surae complex, comprising the gastrocnemius, soleus, and the vestigial plantaris muscles. The biomechanical distinction between these muscles dictates our surgical decision-making. The gastrocnemius is a biarticular muscle, crossing both the knee and the ankle joints. Its medial head originates from the popliteal surface of the femur, superior to the medial femoral condyle, while the lateral head arises from the superolateral surface of the lateral femoral condyle. Because it spans the posterior knee, the tension within the gastrocnemius is highly dependent on knee position; knee extension maximizes tension, whereas knee flexion introduces slack into the system.
Deep and anterior to the gastrocnemius lies the soleus, a powerful monoarticular muscle that originates from the proximal posterior tibia, the fibular head, and the soleal line. Because it only crosses the ankle joint, its tension remains constant regardless of the knee's flexion angle. Biomechanically and histologically, these muscles serve distinct functional roles. The gastrocnemius is predominantly composed of fast-twitch (Type II) muscle fibers, designed for explosive, short-duration activities such as sprinting and jumping. Conversely, the soleus is rich in slow-twitch (Type I) fibers, functioning as a tireless postural stabilizer that prevents the tibia from collapsing forward during the stance phase of gait. Preserving this soleal function is the primary rationale for choosing isolated gastrocnemius lengthening over total Achilles lengthening whenever anatomically feasible.
The surgical target in a Strayer procedure is the gastrocnemius aponeurosis. Distal to the muscle bellies, the medial and lateral heads of the gastrocnemius converge into a broad, glistening, central tendinous raphe. This aponeurosis extends distally, lying directly superficial to the muscular fascia of the soleus. Critically, there is a distinct, avascular areolar tissue plane separating the deep surface of the gastrocnemius aponeurosis from the underlying soleus muscle. Developing this specific interval is the most crucial step of the operation. Distally, in the lower third of the leg, the gastrocnemius aponeurosis and the soleus tendon finally merge to form the conjoined tendo Achilles, which inserts into the posterior tuberosity of the calcaneus.
Operating in the posterior calf requires vigilant navigation of key neurovascular structures. The sural nerve is the primary structure at risk during posterior and posterolateral approaches. Formed by the union of the medial sural cutaneous nerve (a branch of the tibial nerve) and the sural communicating branch (from the common fibular nerve), it pierces the deep fascia in the middle third of the posterior leg. It then courses distally along the lateral border of the Achilles tendon, providing critical sensation to the posterolateral leg and the lateral border of the foot. Medially, the great saphenous vein and the saphenous nerve ascend along the medial aspect of the tibia. While a posteromedial incision safely avoids the sural nerve, careless superficial dissection or overly aggressive medial retraction can easily injure the saphenous structures, leading to troublesome neuromas or localized venous stasis.
Exhaustive Indications and Contraindications
The decision to proceed with operative lengthening of the gastrocnemius fascia requires a rigorous synthesis of the patient’s clinical history, physical examination, and functional goals. Surgery is rarely the first line of treatment. Indications solidify only after the exhaustion of comprehensive conservative modalities, which typically include serial casting, rigid Ankle-Foot Orthoses (AFOs), aggressive physical therapy focusing on stretching, and targeted botulinum toxin A (Botox) injections to manage dynamic spasticity. When these measures fail to prevent progressive contracture, or when the deformity causes intractable pain, recurrent skin breakdown over the metatarsal heads, or an inability to tolerate orthotic bracing, surgical intervention becomes necessary.
The absolute cornerstone of preoperative decision-making is the Silfverskiöld test, which differentiates isolated gastrocnemius contracture from combined gastrocnemius-soleus contracture. The test is performed by assessing passive ankle dorsiflexion with the knee fully extended, and then repeating the measurement with the knee flexed to 90 degrees. If the ankle cannot be dorsiflexed past neutral with the knee extended, but corrects to 10-15 degrees of dorsiflexion when the knee is flexed, the contracture is isolated to the biarticular gastrocnemius muscle. This is the definitive indication for an isolated gastrocnemius fascia lengthening. If the equinus persists regardless of knee position, the soleus or the posterior ankle capsule is also contracted, necessitating a more extensive procedure such as an Achilles tendon lengthening or a posterior capsulotomy.
Contraindications must be carefully respected to avoid disastrous functional outcomes. A primary relative contraindication is the presence of global triceps surae weakness. In patients with profound neuromuscular weakness (e.g., certain variants of spina bifida or advanced muscular dystrophy), the equinus posture may be a necessary compensatory mechanism to stabilize the knee during stance. Lengthening the muscle in this scenario can precipitate an uncontrollable crouch gait. Furthermore, apparent equinus driven by a "midfoot break" or severe cavovarus deformity (often seen in Charcot-Marie-Tooth disease) is a strict contraindication for isolated posterior lengthening; addressing the hindfoot without correcting the midfoot will exacerbate the rocker-bottom deformity.
Indications and Contraindications Summary
| Category | Specific Clinical Scenarios |
|---|---|
| Primary Indications | Positive Silfverskiöld test (dorsiflexion improves with knee flexion). |
| Failure of conservative management (AFOs, serial casting, Botox). | |
| Symptomatic idiopathic toe walking in older children/adolescents. | |
| Spastic diplegia/hemiplegia (CP) with progressive fixed contracture. | |
| Painful plantar forefoot calluses or recurrent ulcerations due to equinus. | |
| Absolute Contraindications | Negative Silfverskiöld test (equinus persists with knee flexion) - requires TAL. |
| Fixed anterior ankle bony block (e.g., massive anterior tibial osteophytes). | |
| Severe midfoot break (rocker-bottom foot) without concurrent midfoot stabilization. | |
| Relative Contraindications | Profound pre-existing triceps surae weakness (risk of iatrogenic crouch gait). |
| Unaddressed severe hamstring contractures (must be addressed simultaneously). | |
| Active local skin infection or compromised posterior calf integument. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the distinguishing mark of a master surgeon. The clinical assessment extends far beyond the examination table. While the Silfverskiöld test provides the anatomical rationale for the procedure, observational or 3D instrumented gait analysis (IGA) provides the functional context. IGA is particularly critical in patients with cerebral palsy, where multi-level spasticity is the norm. Kinematic and kinetic data allow the surgeon to evaluate the timing of ankle plantarflexion, the presence of a premature soleus reflex, and the power generation at push-off. Importantly, gait analysis helps identify compensatory mechanisms at the knee and hip. For instance, an apparent equinus might actually be a compensatory response to severe hamstring tightness and knee flexion contracture. Performing an isolated gastrocnemius lengthening in such a patient without addressing the hamstrings will unmask the knee flexion, driving the patient into a severe crouch.
Radiographic evaluation is mandatory, utilizing standard weight-bearing lateral and anteroposterior views of the foot and ankle. These images serve to rule out structural bony anomalies that mimic or exacerbate equinus.

As demonstrated in the radiographic measures, we specifically evaluate the lateral tibiotalar angle and the calcaneal pitch. A normal calcaneal pitch ranges from 15 to 30 degrees; a severely decreased angle suggests a midfoot break rather than true hindfoot equinus. Furthermore, assessing the anterior distal tibia for osteophytes is crucial, as a bony impingement will mechanically block dorsiflexion regardless of adequate soft tissue release. Meary's angle (the talo-first metatarsal angle) must also be scrutinized to ensure the longitudinal arch is intact and that the equinus is not an illusion created by a severely plantarflexed forefoot.
Patient positioning in the operating room is dictated by the surgical plan and the need for concurrent procedures. For an isolated gastrocnemius lengthening, the prone position offers the most direct, unimpeded anatomical visualization of the posterior calf. However, in the context of neuromuscular disease, equinus correction is frequently performed as part of Single-Event Multilevel Surgery (SEMLS), which may include hamstring lengthenings, adductor releases, or derotational osteotomies. In these scenarios, the supine position is vastly superior.
When positioned supine, a bump is placed under the ipsilateral hip to allow the leg to naturally externally rotate into a "frog-leg" posture. This provides excellent access to the posteromedial calf while allowing simultaneous access to the anterior and medial thigh and hip. Regardless of the position chosen, a well-padded pneumatic tourniquet is applied to the proximal thigh to ensure a completely bloodless surgical field. This ischemia is not merely for convenience; it is absolutely critical for the precise identification of the delicate areolar plane between the gastrocnemius and soleus, and for the safe visualization of the sural and saphenous neurovascular bundles.
Step-by-Step Surgical Approach and Fixation Technique
With the patient properly positioned and the tourniquet inflated, the surgical execution demands precision and respect for tissue planes. We will detail the classic Strayer procedure via a posteromedial approach, which is favored for its safety profile regarding the sural nerve and its excellent exposure of the gastrocnemius aponeurosis.
Incision and Superficial Dissection
The anatomical landmarks are the medial border of the tibia and the palpable musculotendinous junction of the medial head of the gastrocnemius. A 3 to 5-centimeter longitudinal incision is made over the posteromedial aspect of the middle third of the calf, approximately two fingerbreadths posterior to the palpable medial edge of the tibia.

Subcutaneous dissection is carried out meticulously using a combination of sharp dissection and blunt spreading with Metzenbaum scissors. The surgeon must remain highly vigilant during this superficial phase to identify and retract the great saphenous vein and the accompanying saphenous nerve, which frequently traverse the superior aspect of the operative field. Once the subcutaneous fat is parted, the glistening white crural (deep) fascia of the leg is exposed.
Deep Fascial Release and Interval Development
The crural fascia is incised longitudinally in line with the skin incision. Deep to this fascia lies the medial belly of the gastrocnemius muscle. Depending on the exact proximal-distal level of the incision, the surgeon will encounter either the distal muscle belly itself or the proximal extent of the aponeurosis. Using blunt retractors (such as Army-Navy or Langenbeck retractors), the medial border of the gastrocnemius is mobilized and retracted laterally.

As the muscle belly is swept laterally, the broad, flat, pearlescent gastrocnemius aponeurosis comes into full view. The critical technical maneuver of the operation is the development of the interval between the deep surface of the gastrocnemius aponeurosis and the superficial muscular fascia of the underlying soleus muscle.
This plane is typically filled with loose, avascular areolar tissue. A curved hemostat or a blunt periosteal elevator is gently introduced into this interval from medial to lateral. The instrument must glide smoothly; any resistance suggests that the instrument has inadvertently plunged into the soleus muscle belly.

The instrument is passed completely across the posterior calf until its tip can be palpated on the lateral side, ensuring the entire width of the aponeurosis is captured while the soleus remains safely deep to the instrument.
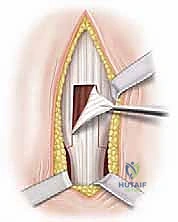
Executing the Aponeurotic Release
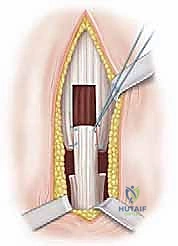
With the soleus protected by the underlying instrument, the gastrocnemius aponeurosis is ready for division. In a classic Strayer procedure, a straight transverse cut is made across the entire width of the aponeurosis using a scalpel or electrocautery.

As the tendinous fibers are divided, the surgeon will immediately observe the proximal stump retracting superiorly, often by 2 to 3 centimeters, revealing the intact, red muscle fibers of the soleus beneath.

It is imperative to ensure that the lateral-most fibers of the aponeurosis are completely released, as retained lateral bands are a common cause of under-correction. Furthermore, the small, cord-like plantaris tendon, which typically lies just medial or deep to the medial edge of the gastrocnemius, should be identified and transected to prevent tethering.
Alternative techniques include the Vulpius procedure (an inverted-V or chevron cut) and the Baker procedure (a tongue-in-groove U-shaped cut). These variations are designed to leave a continuous, albeit lengthened, tendinous bridge, which some surgeons believe facilitates faster healing and reduces the risk of over-lengthening. However, the Strayer remains the most reliable method for achieving significant, predictable correction.

Intraoperative Assessment and Closure
Following the complete transverse release of the aponeurosis, the surgeon must immediately assess the correction. The ankle is forcefully dorsiflexed with the knee held in full, locked extension.

The goal is to achieve a smooth, unresisted 10 to 15 degrees of dorsiflexion beyond neutral. If resistance is still encountered, the surgeon must carefully palpate the depths of the wound for any uncut fascial bands, particularly on the far lateral side or deep within the soleus fascia itself.

Once satisfactory alignment is confirmed, the wound is thoroughly irrigated with sterile saline. The tourniquet is deflated prior to closure to achieve meticulous hemostasis. The dead space created by the retracting muscle can easily fill with a hematoma if bleeding vessels within the soleus or subcutaneous fat are not meticulously cauterized. Crucially, the deep crural fascia is never closed. Closing this fascial layer tightly over the now-lengthened muscle-tendon unit drastically increases the risk of acute compartment syndrome. Only the subcutaneous tissue is reapproximated using interrupted absorbable sutures (e.g., 2-0 or 3-0 Vicryl), followed by a cosmetically meticulous skin closure using a running subcuticular stitch or interrupted nylon sutures.
Complications, Incidence Rates, and Salvage Management
While gastrocnemius fascia lengthening is generally considered a safe and highly effective procedure, it is not devoid of complications. The most dreaded complication, though less common with isolated gastrocnemius lengthening than with total Achilles lengthening, is over-lengthening. Over-lengthening destroys the plantarflexion moment arm, leading to a calcaneal gait. The patient loses the ability to push off during terminal stance, resulting in a shortened step length, increased energy expenditure, and a progressive crouch as the tibia collapses forward unresisted. Salvage of a severely over-lengthened triceps surae is extraordinarily difficult, often requiring complex tendon transfers (e.g., FHL or peroneus brevis to the calcaneus) or even calcaneal osteotomies.
Nerve injury is a recognized risk, particularly to the sural nerve when utilizing a midline or posterolateral approach. Sural neuropraxia occurs in approximately 2-5% of cases, usually presenting as transient numbness or dysesthesia along the lateral foot. More severe injuries, such as complete transection or entrapment within scar tissue, can lead to the formation of a painful neuroma. Management of a symptomatic neuroma involves surgical exploration, excision of the neuroma, and burying the proximal nerve stump deep into the adjacent muscle belly to prevent recurrent surface irritation.
Under-correction or recurrent equinus is the most frequent complication, particularly in the growing child with cerebral palsy. The incidence of recurrence can be as high as 15-20% in spastic diplegia, driven by the relentless nature of the underlying neuromuscular pathology and the longitudinal growth of the tibia outpacing the muscle. Management of recurrence typically involves a return to conservative measures (serial casting, Botox) and, if necessary, a revision lengthening procedure.
Wound complications, including dehiscence, hematoma formation, and superficial surgical site infections, occur in 1-3% of patients. These are largely preventable through meticulous hemostasis post-tourniquet deflation, avoidance of excessive electrocautery near the skin edges, and the use of well-padded, bivalved casts to prevent pressure necrosis over the heel or the incision site.
Complications, Incidence Rates, and Salvage Management Summary
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| Recurrent Equinus |
