Comprehensive Surgical Management of Extensor Mechanism Injuries
Key Takeaway
Disruption of the knee extensor mechanism requires meticulous surgical intervention to restore biomechanical function. This guide details the operative management of chronic patellar tendinosis, inferior pole stress fractures, and acute patellar tendon ruptures. Key principles include excision of degenerative tissue, rigid internal fixation, and precise restoration of patellar height to prevent patella alta or baja, followed by a phased, evidence-based rehabilitation protocol.
Comprehensive Introduction and Patho-Epidemiology
The extensor mechanism of the knee—comprising the quadriceps muscle group, quadriceps tendon, patella, patellar retinaculum, patellar tendon, and tibial tubercle—is critical for normal ambulation, deceleration, and dynamic stabilization of the lower extremity. Pathologies affecting this complex range from chronic, overuse-induced degenerative tendinosis to catastrophic acute ruptures. Surgical management of these conditions requires a profound understanding of knee biomechanics, as the extensor mechanism is subjected to tremendous forces, often exceeding seven to eight times body weight during activities such as jumping, deep squatting, or rapid deceleration. Consequently, operative interventions must prioritize rigid biomechanical fixation, precise restoration of anatomical length, and the biological stimulation of healing in hypovascular zones.
Disruption of the extensor mechanism is a profoundly debilitating injury that severely compromises the functional independence of the patient. While fractures of the patella represent the most common etiology of extensor mechanism failure, soft tissue disruptions—namely, ruptures of the quadriceps tendon and the patellar tendon—are the next most frequent causes and present unique surgical challenges. The classic mechanism of injury involves a violent, eccentric overload to the extensor mechanism. This typically occurs when the foot is firmly planted, the knee is partially flexed, and the patient's body weight forcefully decelerates, overwhelming the tensile strength of the tendon.
Epidemiologically, these injuries exhibit a distinct bimodal distribution based on the specific anatomical structure involved. Patellar tendon ruptures are predominantly observed in patients younger than 40 years old, particularly within an athletic demographic engaged in sports requiring explosive jumping or sprinting. The rupture most frequently occurs as an avulsion from the inferior pole of the patella. Conversely, quadriceps tendon ruptures are statistically more common in patients older than 40 years. These proximal ruptures are highly associated with systemic diseases that compromise collagen integrity, alter matrix metalloproteinase activity, and diminish microvascular perfusion. Associated systemic conditions include systemic lupus erythematosus (SLE), diabetes mellitus, gout, hyperparathyroidism, chronic renal failure (uremia), and morbid obesity.
Furthermore, a well-documented relationship exists between macroscopic tendon rupture and iatrogenic risk factors. The prior use of local corticosteroid injections, systemic corticosteroids, or fluoroquinolone antibiotics can induce rapid collagen necrosis, tenocyte apoptosis, and severe tendinopathy. It is a widely accepted orthopedic principle that healthy, normal tendons rarely rupture under physiological loads. Numerous histologic analyses of ruptured quadriceps and patellar tendons have demonstrated significant pre-existing degenerative changes—such as angiofibroblastic hyperplasia, mucoid degeneration, and disorganized type III collagen proliferation—in up to 64% to 85% of cases. The frequency and severity of these subclinical degenerative changes increase linearly with patient age, explaining why many patients report no antecedent symptoms prior to a catastrophic failure.

Detailed Surgical Anatomy and Biomechanics
A masterful surgical reconstruction of the extensor mechanism demands an intimate knowledge of its layered anatomy and complex biomechanical function. The quadriceps femoris is the primary extensor of the knee, consisting of four distinct muscle bellies: the rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius. These muscles converge distally to form the quadriceps tendon, which inserts into the superior pole (base) of the patella.
Anatomy of the Quadriceps Tendon
The quadriceps tendon is a complex, trilaminar structure. The superficial layer is formed predominantly by the tendinous fibers of the rectus femoris. The middle layer consists of the confluent aponeuroses of the vastus lateralis and vastus medialis, which interdigitate as they approach the patella. The deep layer is composed of the aponeurosis of the vastus intermedius. Understanding this trilaminar anatomy is crucial during the surgical repair of quadriceps tendon ruptures, as anatomical reduction requires the identification and secure mobilization of all three layers, which may retract independently following an acute injury. The vastus medialis obliquus (VMO) inserts lower on the medial border of the patella and plays a critical role in dynamic medial stabilization, preventing lateral patellar subluxation.
The Patella and Patellar Tendon
The patella is the largest sesamoid bone in the human body, embedded within the extensor mechanism to mechanically enhance the moment arm of the quadriceps force vector. By displacing the quadriceps tendon anteriorly away from the center of rotation of the knee joint, the patella increases the mechanical advantage of the extensor mechanism by up to 50% in full extension. The posterior surface of the patella is divided into a heavily cartilaginous superior articular portion and a non-articular inferior pole.
The patellar tendon (ligamentum patellae) originates from the non-articular inferior pole of the patella and inserts distally onto the tibial tubercle. It is approximately 4 to 5 cm in length, 3 cm in width proximally, and narrows to about 2.5 cm at its distal insertion. The vascular supply to the patellar tendon is tenuous, relying on a delicate anastomotic ring formed by the inferior medial and inferior lateral genicular arteries. The central third of the tendon, particularly adjacent to the inferior patellar pole, represents a relative watershed area. This hypovascularity contributes significantly to the pathogenesis of chronic patellar tendinosis ("jumper’s knee") and explains the propensity for ruptures to occur precisely at the osteotendinous junction.
Biomechanical Considerations in Surgery
The forces transmitted through the extensor mechanism are staggering. During level walking, the force across the patellofemoral joint is approximately 0.5 times body weight. However, during stair climbing, this increases to 3 to 4 times body weight, and during deep squatting or explosive jumping, forces can escalate to 7 to 8 times body weight. Consequently, surgical repairs must be incredibly robust. A repair utilizing heavy, non-absorbable sutures (e.g., No. 5 FiberWire or equivalent ultra-high-molecular-weight polyethylene sutures) passed in a locking configuration (such as Krackow or Bunnell) is mandatory to withstand early postoperative rehabilitation forces. Furthermore, restoring the exact anatomical length of the patellar tendon is vital. Over-tensioning the repair results in patella baja (infera), leading to significantly elevated patellofemoral contact pressures, accelerated chondromalacia, and restricted knee flexion. Conversely, under-tensioning leads to patella alta, resulting in an extension lag, reduced mechanical advantage, and potential patellofemoral instability.

Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for extensor mechanism pathology depends heavily on the specific diagnosis, the chronicity of the injury, the patient's functional demands, and the presence of underlying medical comorbidities. Acute complete ruptures are absolute surgical indications, whereas chronic tendinopathies require an exhaustive trial of conservative management prior to surgical consideration.
| Pathology / Condition | Operative Indications | Non-Operative Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|---|
| Complete Extensor Rupture (Patellar/Quad) | Acute complete disruption; Extension lag > 15°; Palpable defect; Retracted patella. | Partial tears with intact active extension; Non-ambulatory patients. | Active deep joint infection; Medically unstable patient. | Severe overlying soft tissue compromise (e.g., massive fracture blisters); Severe dementia. |
| Chronic Patellar Tendinosis | Failure of 6+ months of conservative care; MRI confirming focal mucoid degeneration/partial tear; High-demand athlete unable to compete. | First-line treatment for all patients (eccentric loading, shockwave, PRP). | Active local infection; Complex Regional Pain Syndrome (CRPS). | Unrealistic patient expectations; Poor compliance with rehab protocols. |
| Inferior Pole Stress Fractures | Displaced fractures; Non-unions with persistent pain and functional deficit; Elite athletes requiring rigid stabilization. | Non-displaced fractures in compliant patients (immobilization). | Active infection; Charcot arthropathy. | Severe osteopenia compromising screw purchase (requires alternative fixation). |
| Chronic/Neglected Ruptures (>6 weeks) | Profound weakness; Inability to ambulate without bracing; Severe patella alta/baja. | Asymptomatic patients (rare); Patients who have adapted with minimal functional deficit. | Active infection; Inadequate soft tissue envelope for complex reconstruction. | Severe patellofemoral osteoarthritis (may require simultaneous arthroplasty). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of a successful extensor mechanism reconstruction. The diagnosis of a disrupted extensor mechanism is primarily clinical, though it can be easily missed or delayed in the acute setting, particularly in patients with large lower extremities, massive hemarthrosis, or intact retinacular structures that permit weak, deceptive active extension.
Clinical and Radiographic Evaluation
The hallmark of a complete extensor mechanism disruption is a significant extension lag or the complete inability to perform an active straight-leg raise. A palpable gap is often felt superior to the patella (quadriceps rupture) or inferior to the patella (patellar tendon rupture). Standard anteroposterior (AP) and lateral radiographs are mandatory. A lateral radiograph, particularly with the knee flexed to 30 degrees, is highly sensitive for evaluating patellar height.
Surgeons must strictly utilize established radiographic indices to assess patellar height:
1. Insall-Salvati Ratio: The ratio of the patellar tendon length to the greatest diagonal length of the patella. A normal ratio is between 0.8 and 1.2. A ratio > 1.2 indicates patella alta (suggestive of patellar tendon rupture), while < 0.8 indicates patella baja (suggestive of quadriceps rupture).
2. Caton-Deschamps Index: Measures the distance from the inferior articular edge of the patella to the anterior angle of the tibial plateau, divided by the length of the patellar articular surface.
3. Blackburne-Peel Ratio: The perpendicular distance from the inferior articular margin of the patella to the tibial plateau line, divided by the length of the patellar articular surface.

If the clinical diagnosis remains equivocal due to swelling or patient guarding, ultrasonography or Magnetic Resonance Imaging (MRI) provides definitive visualization of the soft tissue defect. MRI is particularly useful in chronic cases to assess the degree of tendon retraction, muscle atrophy, and fatty infiltration, which will dictate the necessity for complex reconstructive procedures such as a V-Y quadricepsplasty or the use of Achilles tendon allografts.
Patient Positioning and Setup
The patient is positioned supine on a standard radiolucent operating table. A high-thigh pneumatic tourniquet is applied but typically not inflated unless visualization is severely compromised by hemorrhage, as tourniquet inflation can tether the quadriceps muscle, artificially restricting its excursion and complicating anatomical reduction. A lateral post or a sterile leg positioner (e.g., a triangular ramp) is utilized to allow the knee to be comfortably flexed to 90 degrees during the procedure. The contralateral limb must be carefully padded to prevent peroneal nerve palsy. Prophylactic intravenous antibiotics (typically a first-generation cephalosporin) are administered within 60 minutes prior to the skin incision.

Step-by-Step Surgical Approach and Fixation Technique
The surgical techniques for extensor mechanism injuries vary significantly based on the specific pathology, ranging from localized debridement to massive structural reconstructions.
Surgical Technique: Open Debridement of Chronic Patellar Tendinosis
The primary goal of surgery for chronic patellar tendinosis ("jumper’s knee") is the excision of degenerative, non-healing tissue and the stimulation of a robust vascular response.
* Approach and Exposure: A longitudinal midline or parapatellar incision is made over the anterior knee. The subcutaneous tissues are sharply dissected to expose the peritenon.
* Peritenon Management: The tendon sheath is incised longitudinally. It is critical to handle this tissue meticulously, as it houses the primary vascular supply to the anterior tendon.
* Identification and Excision: Longitudinal incisions are made directly into the tendon substance to expose the central core. The area of degeneration—often appearing as gray, friable, mucoid tissue—is sharply excised using a No. 15 blade.
* Biological Stimulation: The inferior pole of the patella is aggressively curetted or drilled using a fine Kirschner wire or high-speed burr to incite a localized healing response and introduce marrow-derived mesenchymal elements.
* Closure: The tendon defect is approximated with side-to-side interrupted 2-0 Vicryl sutures. The peritenon is meticulously closed over the tendon to prevent adhesion formation. Failure to close the peritenon adequately is a major surgical pitfall that leads to severe postoperative adhesions, anterior knee pain, and restricted range of motion.
Surgical Technique: Internal Fixation of Inferior Pole Stress Fractures
Stress fractures through the inferior pole of the patella often present as non-unions due to the constant distraction forces exerted by the patellar tendon.
* Debridement and Reduction: The fibrous non-union tissue is meticulously debrided. The sclerotic fracture surfaces are freshened with a curette or burr to expose bleeding cancellous bone.
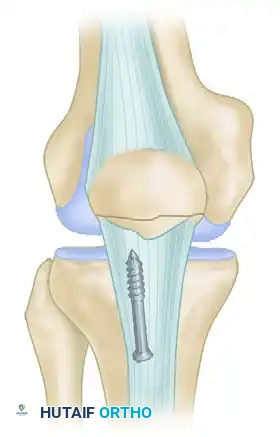
* Internal Fixation: The fracture is reduced and secured using parallel, vertical 4.0 mm partially threaded cancellous screws inserted from distal to proximal.
* Tension Band Augmentation: The fixation is augmented with heavy nonabsorbable sutures (e.g., No. 5 FiberWire) passed circumferentially through the screw holes or around the screw heads in a figure-of-eight tension-band configuration. This converts the anterior distraction forces of the quadriceps into compressive forces at the articular surface.
* Corticocancellous Slot Graft: To enhance biological healing, an oscillating saw is used to harvest a corticocancellous slot graft (10 mm wide × 15 mm long) from the anterior surface of the proximal patella, which is then translated distally across the fracture site.
Surgical Technique: Acute Patellar Tendon Rupture Repair
Acute ruptures should be repaired ideally within the first 2 weeks post-injury. Delaying surgery leads to severe quadriceps contracture.
* Tendon Preparation: The ruptured ends of the tendon are debrided to healthy, organized collagen. Two heavy, non-absorbable sutures (e.g., No. 5 FiberWire) are woven through the distal tendon stump using a locking Krackow or Bunnell technique.
* Transosseous Tunnel Technique (Gold Standard): Three parallel 2.0 mm or 2.5 mm longitudinal drill holes are created through the patella, starting at the inferior pole and exiting at the superior pole. The suture limbs from the tendon are passed through these tunnels using a Beath pin or suture passer.
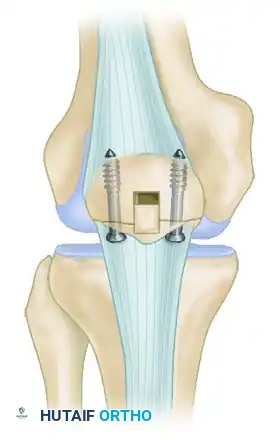
* Suture Anchor Alternative: Recent biomechanical studies support the use of suture anchors. Two or three 4.75 mm to 5.5 mm biocomposite anchors are placed into the inferior pole of the patella. The sutures are then passed through the tendon using a Krackow technique and tied. This eliminates the need for transosseous tunnels and reduces the risk of iatrogenic patellar fracture.
* Tensioning and Retinacular Repair: The knee is flexed to 30 degrees to ensure physiological tensioning. The sutures are tied over the superior pole bone bridge (if using tunnels). The medial and lateral retinacular tears, which almost universally accompany a complete rupture, are meticulously repaired with No. 1 absorbable sutures.
* Augmentation: In cases of poor tissue quality, a cerclage wire or heavy synthetic tape (e.g., FiberTape) is passed through a transverse drill hole in the tibial tubercle and looped over the superior pole of the patella to protect the primary repair during early rehabilitation.


Surgical Technique: Acute Quadriceps Tendon Rupture Repair
The principles are identical to patellar tendon repair. The trilaminar tendon is identified, and a locking Krackow stitch is placed in the medial and lateral aspects of the tendon. Transosseous tunnels are drilled from the superior pole of the patella exiting the inferior pole. The footprint on the superior pole is decorticated with a burr to promote bone-to-tendon healing. The sutures are passed distally and tied over the inferior pole with the knee in extension.
Complications, Incidence Rates, and Salvage Management
Surgical management of the extensor mechanism is fraught with potential complications. The massive forces transmitted through the knee make these repairs particularly vulnerable to failure if rehabilitation is non-compliant or if biological healing is impaired.
| Complication | Incidence (%) | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Postoperative Stiffness (Arthrofibrosis) | 15 - 25% | Prolonged immobilization; Failure to close peritenon; Excessive scar formation. | Aggressive physical therapy; Manipulation under anesthesia (MUA) at 12 weeks; Arthroscopic lysis of adhesions. |
| Re-rupture / Repair Failure | 2 - 5% | Premature eccentric loading; Poor tissue quality (systemic disease); Inadequate initial fixation. | Revision surgery with allograft augmentation (Achilles tendon with bone block); V-Y quadricepsplasty. |
| Patella Baja (Infera) | 5 - 10% | Over-tensioning the repair; Ischemic contracture of the patellar tendon. | Difficult to treat. Proximal tibial tubercle osteotomy (transfer) if severe symptomatic patellofemoral arthritis develops. |
| Hardware Prominence / Pain | 10 - 20% | Subcutaneous position of cerclage wires or knots over the superior patellar pole. | Hardware removal after complete biological healing (minimum 6-12 months post-op). |
| Superficial / Deep Infection | 1 - 3% | Poor soft tissue envelope; Diabetes; Prolonged operative time; Corticosteroid use. | Aggressive operative I&D; Intravenous antibiotics; Retention of hardware until union if possible, or transition to external fixation. |
Phased Post-Operative Rehabilitation Protocols
Successful outcomes following the repair of extensor mechanism injuries rely heavily on a structured, phased rehabilitation program. The surgeon must balance the need to protect the fragile repair with the imperative to prevent devastating arthrofibrosis.
Phase I: Immediate Postoperative Protection (Weeks 0-4)
Immediately following surgery, a rigid knee immobilizer or a hinged knee brace locked in full extension is applied. The patient utilizes crutches for weight-bearing as tolerated with the brace locked in extension. The primary goal of this stage is the protection of the repair and the prevention of profound quadriceps atrophy.
* Therapeutic Exercises: Isometric quadriceps sets, straight-leg raises (in the locked brace), ankle pumps, and core strengthening.
* Range of Motion: Passive range of motion (PROM) is initiated under the strict guidance of a physical therapist. For acute tendon repairs, flexion is typically limited to 0-30 degrees for the first two weeks, advancing to 45-60 degrees by week four.
Phase II: Intermediate Mobilization (Weeks 4-8)
Provided that postoperative swelling has subsided and the surgical incisions are fully healed, the brace is unlocked to allow progressive active-assisted range of motion.
* Therapeutic Exercises: Closed-chain kinetic exercises are cautiously introduced. Shallow leg presses, mini-squats (0-30 degrees), and stationary cycling (once 90 degrees of flexion is achieved) are initiated.
* Precautions: It is imperative to avoid any open-chain active knee extension, as this places massive shear and tensile stress directly across the healing tendon interface.

Phase III: Advanced Strengthening (Weeks 8-12)
The hinged knee brace is progressively discontinued as the patient demonstrates a normal gait pattern and sufficient quadriceps control (no extension lag).
* Therapeutic Exercises: Progression of closed-chain exercises. Step-ups, wall slides, and proprioceptive training (balance boards) are emphasized. Mild eccentric loading can be cautiously introduced late in this phase for tendinosis patients, but must be delayed in massive rupture repairs.
Phase IV: Return to Play and Unrestricted Activity (Months 3-6+)
Return to full, unrestricted athletic activities is a rigorous process. It is permitted only when the patient has achieved 85% to 90% of contralateral limb strength on isokinetic testing, a full and completely painless range of motion, and psychological readiness. For elite jumping athletes recovering from a complete rupture, this process routinely takes 9 to 12 months.
Summary of Landmark Literature and Clinical Guidelines
The surgical evolution of extensor mechanism repair is deeply rooted in several landmark biomechanical and clinical studies. Historically, the transosseous tunnel technique, popularized by Insall and others, remained the undisputed gold standard for both quadriceps and patellar tendon ruptures. However, the requirement to drill multiple tunnels through the patella carries an inherent risk of iatrogenic fracture and significant soft tissue dissection.
Recent paradigm shifts, guided by robust biomechanical literature, have validated the use of suture anchors. Studies by Bushnell et al. and Ettinger et al. have demonstrated that suture anchor repairs for patellar tendon ruptures offer equivalent or superior ultimate load-to-failure rates compared to traditional transosseous tunnels. More importantly, suture anchors have been shown to result in significantly less gap formation at the repair site under cyclic loading. Gap formation is the primary precursor to clinical failure and elongation (resulting in patella alta).
For chronic, neglected ruptures, the literature strongly supports the use of Achilles tendon allografts with a calcaneal bone block. As described by Rougraff and others, the bone block is press-fit into a trough created in the tibial tubercle, while the tendinous portion is woven through the remaining native tissue and the quadriceps tendon. This technique provides immediate structural stability and a robust collagen scaffold for host tissue ingrowth, representing the definitive salvage procedure for massive extensor mechanism defects.
Ultimately, the successful management of extensor mechanism pathology dictates that the orthopedic surgeon acts with anatomical precision, utilizes uncompromisingly rigid fixation constructs, and implements a deeply supervised, biologically respectful rehabilitation protocol.
