Proximal Hamstring Avulsion Repair: An Intraoperative Masterclass
Key Takeaway
This masterclass provides an exhaustive guide to proximal hamstring avulsion repair. We cover crucial surgical anatomy, meticulous preoperative planning, and a granular, step-by-step intraoperative execution from incision to closure. Fellows will learn precise instrument use, critical pearls and pitfalls, and comprehensive postoperative rehabilitation protocols to optimize patient outcomes. Master this complex procedure with expert guidance.
Comprehensive Introduction and Patho-Epidemiology
Proximal hamstring avulsions represent a catastrophic disruption of the posterior thigh musculature, drastically altering the biomechanical kinetic chain of the lower extremity. Unlike the ubiquitous low-grade musculotendinous strains frequently encountered in athletic populations, a complete avulsion from the ischial tuberosity is a profound structural failure. This injury fundamentally compromises the dynamic stabilization of both the hip and the knee, leading to a profound loss of power during the swing phase of gait and explosive athletic maneuvers. For the high-demand athlete, or even the active middle-aged patient, conservative management of a complete three-tendon avulsion frequently results in unacceptable chronic pain, crippling weakness in deep knee flexion, and a high likelihood of permanent exclusion from their pre-injury level of physical activity.
The epidemiology of this injury spans a bimodal distribution, capturing both the young, explosive athlete and the middle-aged "weekend warrior." In the younger demographic, the mechanism typically involves a sudden, violent eccentric contraction of the hamstring complex with the hip hyperflexed and the knee forcefully extended—classic scenarios include water skiing starts, forced splits in gymnastics, or a misjudged hurdle. In the middle-aged population, degenerative tendinopathy often acts as a precursor, lowering the threshold for ultimate tensile failure. In these instances, a seemingly innocuous slip on wet grass or a sudden lunge on the tennis court can precipitate a complete avulsion. Understanding this demographic variance is crucial, as the biologic healing potential and the degree of associated tendinosis dictate our surgical strategy and expected outcomes.
Pathophysiologically, the moment the tendons avulse from the ischial footprint, the unopposed resting tone of the massive hamstring muscle belly causes immediate distal retraction. This retraction creates a vast hematoma within the posterior thigh, which, if left untreated, organizes into dense, fibrotic scar tissue. This "hamstring syndrome" is characterized not only by mechanical weakness but also by severe neuropathic pain. The massive hematoma and subsequent fibroblastic response frequently engulf the adjacent sciatic nerve, leading to chronic tethering and debilitating radicular symptoms that radiate down the posterior leg. This underscores the critical importance of early surgical intervention; acute repairs performed within the first three to four weeks capitalize on mobile tissue planes, whereas chronic repairs degenerate into complex, high-risk neurolysis procedures.
Clinically, the presentation of a complete proximal hamstring avulsion is unmistakable to the astute orthopedist. Patients invariably report a distinct, audible "pop" accompanied by immediate, searing pain in the deep gluteal region. Upon physical examination, a massive ecchymosis typically tracks down the posterior thigh, sometimes reaching the popliteal fossa within days. Palpation reveals a distinct defect or "divot" immediately distal to the ischial tuberosity, and the retracted muscle belly may present as a pseudo-mass in the mid-posterior thigh. Provocative testing demonstrates profound weakness with resisted knee flexion and hip extension, particularly when the hip is placed in 90 degrees of flexion. It is imperative to differentiate this true avulsion from lumbar radiculopathy, piriformis syndrome, or, in the skeletally immature patient, an ischial apophyseal avulsion, which requires a completely different management algorithm.
Detailed Surgical Anatomy and Biomechanics
A masterful surgical repair demands an intimate, three-dimensional understanding of the posterior thigh anatomy. The hamstring complex comprises three distinct muscles: the semimembranosus, the semitendinosus, and the biceps femoris (long and short heads). With the exception of the short head of the biceps femoris, which originates from the linea aspera of the posterior femur, these muscles share a common, robust origin on the ischial tuberosity. The footprint on the ischium is highly organized; the semitendinosus and the long head of the biceps femoris form a conjoint tendon that originates on the posteromedial aspect of the tuberosity, while the semimembranosus has a distinct, broad, crescent-shaped origin positioned slightly more anterolateral and deep to the conjoint tendon. Recreating this specific footprint topography is essential for restoring native biomechanics.
Biomechanically, the hamstrings are biarticular muscles, spanning two major joints to act as primary hip extensors and knee flexors. This dual-joint span is precisely what renders them highly susceptible to injury. During the terminal swing phase of running, the hamstrings undergo massive eccentric loading to decelerate the rapidly extending tibia while simultaneously preparing to drive the hip into extension for the stance phase. The force generated during this eccentric phase can exceed several times the individual's body weight. When the load surpasses the ultimate tensile strength of the tendon-bone interface, catastrophic failure occurs. The surgical repair must therefore possess sufficient biomechanical strength to withstand not only the passive resting tone of the muscle but also the eventual return to these extreme eccentric loads.
The neurovascular anatomy of the posterior thigh is unforgiving, and the sciatic nerve is the paramount structure of concern. The sciatic nerve emerges from the greater sciatic foramen, passing deep to the piriformis muscle, and courses distally down the posterior thigh. At the level of the ischial tuberosity, the nerve lies immediately lateral to the hamstring origin—often separated by a mere 1.0 to 1.5 centimeters. In the acute setting, the nerve is usually safe if dissection remains strictly medial to the lateral border of the ischium. However, in subacute or chronic cases, the massive hematoma and subsequent scarring can completely distort normal tissue planes, pulling the sciatic nerve medially and encasing it within the retracted tendon stump. Meticulous, millimeter-by-millimeter dissection is required to identify and protect the nerve before any traction is applied to the hamstrings.
Equally important, though frequently underappreciated, is the posterior femoral cutaneous nerve (PFCN). This nerve provides critical sensory innervation to the posterior thigh, the perineum, and the inferior gluteal region. The PFCN exits the pelvis inferior to the piriformis, running deep to the gluteus maximus but superficial to the long head of the biceps femoris. Its inferior cluneal branches curve superiorly around the inferior border of the gluteus maximus. During our surgical approach, aggressive retraction of the gluteus maximus or indiscriminate fascial incisions can easily stretch or transect these delicate branches. Iatrogenic injury to the PFCN results in severe, intractable dysesthesia and numbness with sitting, a complication that patients find exceptionally distressing and which can overshadow an otherwise mechanically perfect tendon repair.
Exhaustive Indications and Contraindications
The decision-making algorithm for managing proximal hamstring injuries has evolved significantly over the past two decades. Historically, even complete avulsions were often managed non-operatively, leading to a cohort of patients with chronic weakness, cramping, and sciatic nerve tethering. Today, the indications for surgical intervention are clearly defined and lean heavily toward early, aggressive repair for specific injury patterns. The primary indication for acute surgical repair is a complete avulsion of all three hamstring tendons (semimembranosus, semitendinosus, and biceps femoris long head) from the ischial tuberosity, particularly when associated with distal retraction greater than 2 centimeters. Furthermore, two-tendon avulsions (typically the conjoint tendon) in high-level athletes or highly active individuals are strongly considered for operative management to ensure a return to peak explosive power.
Conversely, conservative management remains the gold standard for isolated, single-tendon avulsions (most commonly the semimembranosus) with minimal to no retraction, as well as for all partial tears and musculotendinous junction strains. These injuries possess a robust vascular supply and demonstrate excellent healing potential with a structured, progressively loaded rehabilitation program. Surgery is also generally contraindicated in low-demand, sedentary patients, or elderly individuals with significant medical comorbidities where the risks of anesthesia, prolonged prone positioning, and potential postoperative complications outweigh the functional benefits of anatomical restoration. In these populations, the primary goal is pain control and functional adaptation rather than athletic restoration.
The timing of the surgical intervention is a critical variable that dictates both the technical difficulty of the procedure and the ultimate prognosis. Acute repairs, performed within 3 to 4 weeks of the initial injury, are the ideal scenario. During this window, the hematoma is still relatively liquid, tissue planes are preserved, and the tendon stumps can generally be mobilized and brought back to the ischial footprint with minimal tension. Subacute (4 to 6 weeks) and chronic (>6 weeks) repairs present a formidable surgical challenge. The tendons become scarred, atrophic, and severely retracted, often requiring extensive, high-risk sciatic neurolysis and fractional lengthening of the muscle belly. In severe chronic cases, direct primary repair may be impossible, necessitating the use of Achilles tendon allografts to bridge the gap, which significantly alters the postoperative rehabilitation timeline and functional expectations.
| Variable | Indications for Surgical Repair | Contraindications for Surgical Repair |
|---|---|---|
| Tendon Involvement | Complete 3-tendon avulsion; 2-tendon avulsion in athletes. | Single-tendon avulsion; Partial tears; MTJ strains. |
| Retraction Degree | Retraction > 2 cm from the ischial tuberosity. | Minimal or no retraction (< 2 cm). |
| Patient Profile | High-demand athletes; Active middle-aged patients. | Sedentary lifestyle; Elderly with high surgical risk. |
| Timing/Chronicity | Acute (< 4 weeks) preferred; Chronic cases with intractable pain/weakness. | Chronic cases in low-demand patients without sciatic nerve tethering. |
| Associated Pathology | Sciatic nerve tethering/compression symptoms. | Severe local infection; Medically unfit for prone anesthesia. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock of a successful proximal hamstring repair. The clinical evaluation must be corroborated by high-quality magnetic resonance imaging (MRI), which serves as the definitive gold standard for diagnosis and preoperative mapping. We rely heavily on fluid-sensitive T2-weighted coronal and axial sequences to identify the acute hematoma, quantify the exact number of avulsed tendons, and measure the precise degree of distal retraction. T1-weighted images are equally critical, particularly in subacute or chronic cases, to assess the quality of the muscle belly for fatty infiltration and atrophy, akin to the Goutallier classification used in rotator cuff pathology. Severe fatty infiltration may portend a poor functional outcome and can influence the decision to proceed with complex reconstructive efforts.


While traditional radiographic templating is less relevant here than in arthroplasty, mental templating and strategic preparation are paramount. The surgeon must evaluate the bone quality of the ischial tuberosity on the MRI. In older patients or those with osteopenia, the cortical shell of the ischium may be thin, increasing the risk of suture anchor pullout or cortical blowout during drilling. In such cases, the surgical plan must be adapted to utilize a higher number of smaller-diameter all-suture anchors to distribute the load, or the use of heavy non-absorbable sutures passed through transosseous bone tunnels. Furthermore, the surgical team must ensure that all necessary equipment, including a variety of high-strength suture tapes, specialized deep retractors, neurolysis loops, and potential allograft tissue for chronic cases, is readily available in the operating theater before the patient is anesthetized.

Patient positioning for this procedure is an exercise in precision and vigilance. The patient is placed in the prone position on a standard operating table following the induction of general anesthesia. It is imperative to utilize well-placed chest rolls or a specialized prone frame to allow for unencumbered abdominal excursion, thereby reducing venous pressure and minimizing intraoperative bleeding. Every pressure point—including the face, eyes, shoulders, iliac crests, and the dorsum of the feet—must be meticulously padded to prevent devastating perioperative nerve palsies or pressure necrosis. The arms are typically positioned on padded arm boards with the shoulders abducted no more than 90 degrees to protect the brachial plexus.
The draping of the operative extremity is a critical step that cannot be overstated. The entire affected leg must be prepped and draped free into the sterile field, from the iliac crest down to the foot. This free-draping technique is non-negotiable, as it allows the surgical assistant to manipulate the limb dynamically throughout the procedure. By flexing the knee to 90 degrees and extending the hip, the surgeon can dramatically reduce the tension on the hamstring muscle belly. This maneuver is essential for assessing the excursion of the retracted tendon stumps, determining if primary repair is feasible, and ultimately tying the high-strength suture knots without catastrophic tension that would otherwise lead to immediate construct failure upon waking.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach begins with a carefully planned incision over the posterior thigh. For acute injuries with minimal retraction, a transverse incision within the gluteal crease provides an excellent cosmetic result. However, for complete avulsions with retraction exceeding 3 centimeters, or in any chronic scenario, a longitudinal incision is mandatory. This incision begins precisely over the palpable prominence of the ischial tuberosity and extends distally for 10 to 15 centimeters, following the midline of the posterior thigh. After incising the skin and subcutaneous tissues with electrocautery, we identify the investing deep fascia. Meticulous hemostasis at this stage is vital, as the highly vascular subcutaneous fat can bleed profusely, obscuring the deep anatomical landmarks.
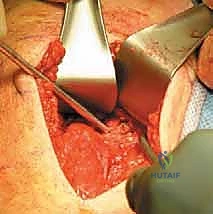
Upon incising the deep fascia, the inferior border of the gluteus maximus comes into view. Using blunt dissection, we mobilize the inferior edge of the muscle and retract it superiorly using a broad, blunt retractor such as a Meyerding or a large right-angle retractor. It is at this exact moment that the surgeon must actively seek out and protect the inferior cluneal branches of the posterior femoral cutaneous nerve. Once the gluteus is elevated, the massive hematoma characteristic of this injury is typically encountered. We carefully evacuate the hematoma to reveal the underlying pathology. The sciatic nerve must be identified immediately. We locate the nerve lateral to the ischial tuberosity, using a peanut sponge to gently clear the surrounding areolar tissue. Once positively identified, a vessel loop is passed around the sciatic nerve to maintain continuous visual control and protect it from inadvertent traction or sharp injury throughout the remainder of the case.

With the sciatic nerve safeguarded, attention is turned to the avulsed hamstring tendons. The stumps are often retracted distally and may be folded upon themselves or encased in early fibrous scar tissue. We grasp the distal aspect of the tendinous mass with heavy Alice or Kocher clamps and apply gentle proximal traction. The assistant simultaneously extends the hip and flexes the knee to facilitate mobilization. We then place multiple locking Krackow stitches using #2 or #5 ultra-high-molecular-weight polyethylene (UHMWPE) suture tape into the distinct tendon stumps (conjoint tendon and semimembranosus). With control of the tendons secured, we meticulously debride the ischial tuberosity footprint. Using a combination of a Cobb elevator, rongeurs, and a motorized burr, we remove all soft tissue remnants and decorticate the bone down to a bleeding cancellous bed. This biological preparation is absolutely critical; without a bleeding bone surface, the tendon will fail to integrate, leading to inevitable construct failure regardless of the mechanical strength of the anchors.

The final phase is the mechanical fixation of the tendons to the prepared ischial footprint. We utilize a multi-anchor construct to maximize the surface area of compression and distribute the tensile load. Typically, three to four double- or triple-loaded suture anchors (solid titanium, PEEK, or all-suture designs depending on bone quality) are placed into the ischial tuberosity. The anchors are positioned to recreate the native crescent-shaped footprint, with care taken to angle the drill trajectories away from the hip joint and the sciatic notch. The sutures from the anchors are then passed through the corresponding tendon stumps using a free needle, often employing a modified Mason-Allen or a double-row equivalent configuration for maximum rip-stop security. The assistant holds the leg in maximum tension-relieving position (hip extended, knee flexed to 90 degrees) while the knots are sequentially tied. The repair is visually inspected, and the leg is gently ranged to ensure the construct is mechanically sound before meticulous closure over a closed-suction drain.
Complications, Incidence Rates, and Salvage Management
While proximal hamstring avulsion repair yields excellent functional outcomes when executed flawlessly, the complication profile is significant due to the unforgiving regional anatomy. The most devastating intraoperative complication is iatrogenic injury to the sciatic nerve. The incidence of transient sciatic nerve neurapraxia ranges from 2% to 8% in the literature, often resulting from aggressive retraction, thermal injury from electrocautery, or compression from a postoperative hematoma. Permanent sciatic nerve palsy is rare (less than 1%) but catastrophic, resulting in foot drop and profound sensory loss. If a patient awakens with a new-onset sciatic deficit, an immediate evaluation is required. If a compressive hematoma is suspected, emergent surgical decompression is mandated. Transient neurapraxias are managed conservatively with an ankle-foot orthosis (AFO) to prevent equinus contracture and gabapentinoids for neuropathic pain control, with recovery often taking 6 to 12 months.
Mechanical failure of the repair is another major concern, with re-rupture rates reported between 3% and 7%. Failures typically occur at the suture-tendon interface (suture pull-through) or at the bone-anchor interface (anchor pullout). The primary risk factors for mechanical failure include poor bone density at the ischial tuberosity, inadequate intraoperative mobilization leading to a high-tension repair, and, most commonly, patient non-compliance with postoperative weight-bearing and bracing restrictions. Early eccentric loading before biologic healing has occurred will invariably destroy the repair. Salvage management for a failed primary repair is highly complex. It almost always requires a massive, extensile exposure, extensive sciatic neurolysis, and the utilization of a robust Achilles tendon allograft with a calcaneal bone block to bridge the resultant massive defect.
Infection and wound healing complications, while less frequent (1% to 3%), are particularly problematic in this anatomical region. The proximity of the incision to the perineum increases the risk of contamination with enteric flora. Furthermore, the massive dead space created by the hematoma evacuation and tendon mobilization is highly prone to fluid accumulation. Meticulous hemostasis and the routine use of a deep closed-suction drain for 24 to 48 hours postoperatively are essential preventative measures. Superficial wound dehiscence or minor infections can often be managed with oral antibiotics and local wound care. However, deep infections tracking down to the suture anchors require aggressive surgical irrigation and debridement, and may ultimately necessitate the removal of the hardware and the repair, resulting in a permanent functional deficit.
| Complication | Estimated Incidence | Primary Etiology / Risk Factors | Management / Salvage Strategy |
|---|---|---|---|
| Sciatic Nerve Neurapraxia | 2% - 8% | Overzealous retraction; Hematoma compression; Chronic scarring. | AFO for foot drop; Gabapentinoids; Emergent decompression if hematoma. |
| Re-rupture / Construct Failure | 3% - 7% | Patient non-compliance; Poor bone quality; High-tension repair. | Revision surgery with Achilles tendon allograft augmentation. |
| PFCN Dysesthesia | 5% - 10% | Iatrogenic transection; Stretch injury during gluteal retraction. | Symptomatic management; Desensitization therapy; Rarely surgical neuroma excision. |
| Deep Surgical Site Infection | 1% - 3% | Perineal proximity; Large dead space; Hematoma formation. | Urgent I&D; Intravenous antibiotics; Potential hardware removal. |
| Deep Vein Thrombosis (DVT) | < 2% | Prolonged immobility; Prone positioning; Lower extremity trauma. | Chemical prophylaxis (LMWH/Aspirin) per risk stratification; Compression devices. |
Phased Post-Operative Rehabilitation Protocols
The surgical repair is merely the first step in a protracted journey toward functional recovery; the postoperative rehabilitation protocol is equally critical to the ultimate success of the procedure. The rehabilitation is strictly phased, respecting the biological timeline of tendon-to-bone healing. Phase I (0 to 6 weeks postoperatively) is the Maximum Protection Phase. The primary goal is to protect the fragile mechanical repair while allowing the initial inflammatory and proliferative phases of healing to occur. The patient is placed in a custom, hinged hip-knee-ankle-foot orthosis (HKAFO) or a specialized pelvic band brace. The hip is locked in neutral to 20 degrees of extension, and the knee is locked in 60 to 90 degrees of flexion to absolutely minimize tension on the ischial footprint. Patients are strictly non-weight bearing or toe-touch weight-bearing with bilateral crutches. Only passive range of motion within highly restricted, safe zones is permitted under the direct supervision of a physical therapist.
Phase II (6 to 12 weeks) marks the Controlled Mobilization Phase. As the tendon begins to incorporate into the cancellous bone bed, we gradually introduce controlled mechanical stress to promote collagen alignment and tissue remodeling. The brace is sequentially unlocked, allowing for progressive knee extension and hip flexion. Weight-bearing is advanced linearly, transitioning from partial to full weight-bearing by the end of week 8 to 10, allowing the patient to wean off crutches. Active-assisted and active knee flexion are initiated, but active hip extension and combined hip flexion/knee extension (the classic hamstring stretch position) are still strictly avoided. Isometric strengthening exercises are introduced in neutral positions to prevent profound muscle atrophy without jeopardizing the repair site.
Phase III (3 to 6 months) is the Strengthening Phase. By the third month, biological healing is robust enough to withstand significant loading. The focus shifts to restoring muscle bulk, endurance, and concentric power. Closed kinetic chain exercises, such as leg presses, step-ups, and bridging, form the core of the program. The critical transition in this phase is the cautious introduction of eccentric loading. We begin with submaximal eccentric exercises and slowly progress toward more demanding protocols, such as modified Nordic hamstring curls, as tolerated. The physical therapist must closely monitor the patient for any signs of pain or apprehension at the ischial origin, adjusting the intensity accordingly. Core stabilization and lumbopelvic control exercises are also heavily emphasized to correct any compensatory movement patterns developed during the injury and early recovery phases.
Phase IV (6+ months) is the Return to Sport Phase. This final stage bridges the gap between clinical rehabilitation and high-level athletic performance. The protocol becomes highly individualized based on the patient's specific sport and positional demands. Agility drills, plyometrics, and sport-specific sprinting mechanics are integrated. The progression to full, unrestricted sprinting is the final and most dangerous hurdle, as it replicates the exact mechanism of the initial injury. Before a patient is cleared for full return to play, they must pass rigorous objective criteria. We require an isokinetic dynamometer strength test demonstrating greater than 85% to 90% symmetry compared to the uninjured contralateral
