Comprehensive Introduction and Patho-Epidemiology
Suprascapular neuropathy is a well-recognized, albeit frequently underdiagnosed, etiology of posterior shoulder pain and profound shoulder girdle weakness. Historically, this clinical entity has been a diagnostic challenge, frequently misdiagnosed as primary rotator cuff pathology, cervical radiculopathy, or idiopathic brachial neuritis (Parsonage-Turner syndrome). One of the most common and structurally definable etiologies of this neuropathy is extrinsic compression by a ganglion cyst, commonly referred to as a paralabral cyst. These cysts typically arise secondary to capsulolabral injuries—most notably Superior Labrum Anterior and Posterior (SLAP) tears or posterior labral avulsions. The underlying pathophysiology involves a capsular defect that acts as a one-way biological valve, allowing pressurized synovial fluid to extravasate from the glenohumeral joint and pool in the anatomically constrained spaces of the spinoglenoid or suprascapular notch.
The epidemiological profile of suprascapular nerve entrapment secondary to ganglion cysts demonstrates a strong predilection for overhead athletes, including volleyball players, baseball pitchers, tennis players, and elite swimmers, as well as manual laborers subjected to repetitive overhead loading. The repetitive microtrauma to the posterior capsule and labrum in these populations predisposes them to the initial labral disruption. Once the cyst begins to form, the highly confined fibro-osseous tunnels of the scapula leave the suprascapular nerve highly vulnerable to compressive ischemia. Over time, this chronic compression leads to progressive demyelination and subsequent axonal loss, manifesting clinically as insidious onset, deep-seated posterior shoulder pain, and progressive atrophy of the supraspinatus and/or infraspinatus muscle bellies.
While modern orthopedic practice has seen a significant shift toward the arthroscopic management of these cysts—primarily through intra-articular decompression combined with labral repair—the open posterior approach remains an indispensable technique in the shoulder surgeon's armamentarium. The open approach is specifically mandated for massive, multiloculated cysts that extend far medially into the suprascapular fossa, cysts with thick, organized, and fibrotic walls that resist arthroscopic aspiration, or cases involving primary nerve entrapment by an ossified transverse scapular ligament without a concomitant intra-articular labral tear.
This masterclass provides a comprehensive, textbook-level guide to the open posterior surgical approach for the excision of a ganglion cyst and the decompression of the suprascapular nerve. It is meticulously tailored for orthopedic residents, shoulder and elbow fellows, and practicing consultant surgeons who require a definitive reference for managing complex, extra-articular compressive lesions of the suprascapular nerve.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the suprascapular nerve's anatomical course and its relationship to the surrounding osteofascial structures is non-negotiable for safe and effective surgical intervention. The suprascapular nerve is a mixed motor and sensory nerve originating primarily from the upper trunk of the brachial plexus, deriving its fibers from the C5 and C6 ventral rami, with occasional variable contributions from C4.
The Suprascapular Nerve Course and the Suprascapular Notch
After branching from the upper trunk at Erb’s point, the nerve courses laterally and posteriorly through the posterior triangle of the neck. It passes deep to the trapezius and omohyoid muscles, tracking along the inferior belly of the omohyoid to reach the superior border of the scapula. Here, the nerve encounters its first major anatomical bottleneck: the suprascapular notch. The nerve passes through the suprascapular notch, which is roofed by the superior transverse scapular ligament. The morphology of this notch is highly variable and has been classified by Rengachary into six distinct types, ranging from a wide, shallow depression (Type I) to a completely ossified foramen (Type VI). An ossified or highly stenotic notch significantly increases the risk of primary nerve entrapment, independent of ganglion cyst formation.
Crucially, the vascular bundle maintains a distinct relationship to the ligament. The suprascapular artery and vein pass over the transverse scapular ligament. This anatomical relationship is critical during surgical dissection to avoid catastrophic hemorrhage. Surgeons rely on the classic mnemonic "Army over Navy" at the suprascapular notch: The suprascapular Artery passes over the ligament, while the suprascapular Nerve passes under the ligament. Immediately after exiting the notch, the nerve provides two to three motor branches to the supraspinatus muscle, as well as sensory branches to the acromioclavicular and glenohumeral joints.
The Spinoglenoid Notch and Terminal Innervation
After innervating the supraspinatus, the main trunk of the nerve courses laterally and inferiorly around the lateral base of the scapular spine, a region known as the spinoglenoid notch. Here, the nerve passes under the spinoglenoid ligament (inferior transverse scapular ligament), a fascial band present in approximately 50% to 80% of individuals. After traversing this second fibro-osseous tunnel, the nerve provides terminal motor innervation to the infraspinatus muscle.
Biomechanics of Compression
The biomechanics of suprascapular nerve compression are entirely dependent on the anatomical location of the space-occupying lesion. Ganglion cysts located at the suprascapular notch compress the main trunk of the nerve before it gives off branches to the supraspinatus. This proximal compression leads to global denervation, resulting in profound weakness in both shoulder abduction (supraspinatus) and external rotation (infraspinatus), accompanied by visible atrophy in both fossae. Conversely, cysts located at the spinoglenoid notch selectively compress the inferior branch of the nerve after the supraspinatus branches have already diverged. This distal compression results in isolated infraspinatus atrophy and weakness in external rotation, while abduction strength and supraspinatus muscle bulk remain entirely intact. Understanding this biomechanical dichotomy is essential for accurate clinical diagnosis and precise surgical targeting.
Exhaustive Indications and Contraindications
The decision to proceed with open surgical excision of a suprascapular nerve ganglion cyst must be carefully weighed against the natural history of the disease, the potential for spontaneous resolution, and the efficacy of modern arthroscopic alternatives. Surgical intervention is generally reserved for patients who have failed a rigorous trial of conservative management, or those presenting with profound, irreversible neurological deficits.
Indications for Open Excision
The primary indication for the open posterior approach is the presence of a massive, extra-articular ganglion cyst causing symptomatic suprascapular neuropathy that cannot be adequately addressed via arthroscopy. Patients who have undergone 3 to 6 months of non-operative treatment—including non-steroidal anti-inflammatory drugs (NSAIDs), physical therapy focusing on periscapular stabilization, and ultrasound-guided cyst aspiration—without sustained symptomatic relief are prime candidates. Furthermore, clinical or electromyographic (EMG) evidence of progressive supraspinatus or infraspinatus muscle atrophy necessitates urgent decompression to prevent irreversible fatty infiltration of the rotator cuff musculature. The open approach is specifically mandated for multiloculated cysts with thick septations, cysts extending far medially into the suprascapular fossa, or revision cases where previous arthroscopic decompression has failed.
Contraindications to Surgery
Absolute contraindications include active local or systemic infection, severe medical comorbidities precluding the safe administration of general anesthesia, and the presence of asymptomatic cysts discovered incidentally on advanced imaging. A critical relative contraindication is the presence of end-stage muscle atrophy with severe fatty infiltration (Goutallier Stage 3 or 4). In these advanced cases, the motor endplates have undergone irreversible degeneration, and surgical decompression of the nerve is highly unlikely to result in the restoration of muscle bulk or strength, though it may still be offered strictly for palliative pain relief.
| Parameter | Indications for Open Excision | Contraindications (Absolute & Relative) |
|---|---|---|
| Clinical Presentation | Persistent pain/weakness > 3-6 months; progressive atrophy. | Asymptomatic incidental cyst; pain originating from cervical spine. |
| Imaging Findings | Massive, multiloculated cyst; extra-articular medial extension; ossified transverse ligament. | Goutallier Stage 3/4 fatty infiltration (relative); no identifiable compressive lesion. |
| Failed Prior Tx | Recurrence after ultrasound-guided aspiration or failed arthroscopic decompression. | Lack of prior conservative management trial (unless acute profound motor loss). |
| Patient Factors | High-demand overhead athlete; manual laborer requiring external rotation strength. | Medically unfit for general anesthesia; active surgical site infection. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of a successful open posterior approach to the shoulder. The surgeon must synthesize clinical findings, advanced imaging, and electrodiagnostic data to formulate a precise surgical roadmap.
Preoperative Imaging and Electrodiagnostics
High-resolution Magnetic Resonance Imaging (MRI) without contrast is the gold standard for evaluating suprascapular neuropathy. T2-weighted fat-suppressed sequences are exquisitely sensitive for identifying the hyperintense ganglion cyst, delineating its exact anatomical location, and tracing its stalk to the capsulolabral defect. Furthermore, T1-weighted sagittal oblique sequences are critical for assessing the degree of fatty infiltration and atrophy within the supraspinatus and infraspinatus muscle bellies, which dictates the patient's prognosis. MR Arthrogram may be utilized if a concomitant SLAP tear is suspected but poorly visualized on standard MRI. Electromyography and Nerve Conduction Studies (EMG/NCS) are essential adjuncts. They confirm the diagnosis of denervation (evidenced by fibrillation potentials and positive sharp waves), precisely localize the site of compression (suprascapular vs. spinoglenoid notch), and establish a crucial baseline to monitor postoperative neurological recovery.
Anesthesia Considerations
The procedure is universally performed under general anesthesia to ensure complete patient immobility and airway control in the prone or lateral decubitus position. An interscalene regional nerve block may be administered pre-operatively for profound postoperative pain control. However, the surgeon must carefully weigh this against the need for immediate postoperative neurological assessment. If an interscalene block is utilized, the patient must be counseled that they will experience a temporary, complete motor and sensory deficit of the operative extremity, precluding immediate evaluation of the suprascapular nerve's recovery. If intraoperative neuromonitoring is planned (though infrequent for this specific procedure), long-acting paralytic agents must be strictly avoided by the anesthesia team.
Patient Positioning and Preparation
The patient can be positioned in either the lateral decubitus or prone position, largely dependent on the surgeon's training and preference. The prone position is highly favored for the open posterior approach as it provides unparalleled, stable exposure of the scapular spine, the posterior shoulder musculature, and the suprascapular fossa.
When utilizing the prone position, the patient is carefully rolled onto a specialized padded frame (e.g., Jackson table with chest rolls) to ensure the abdomen hangs free, thereby minimizing venous pressure and epidural bleeding. The head is securely positioned in a neutral alignment using a foam face mask or Mayfield tongs, ensuring the cervical spine is not subjected to undue rotation or extension. The operative arm is draped free, allowing the surgical assistant to manipulate the limb through various degrees of abduction and rotation to optimize the tension on the posterior musculature during deep dissection. The entire shoulder girdle, hemithorax, axilla, and arm are prepped with a chlorhexidine-based solution and draped in a standard sterile fashion, ensuring wide exposure from the base of the neck to the inferior angle of the scapula.
Step-by-Step Surgical Approach and Fixation Technique
The open posterior approach to the suprascapular and spinoglenoid notches requires an intimate knowledge of posterior shoulder anatomy and meticulous surgical technique to avoid iatrogenic injury to the trapezius, the rotator cuff, and the neurovascular bundle.
1. Skin Incision and Superficial Dissection
Following the administration of prophylactic intravenous antibiotics and the application of a surgical time-out, the anatomical landmarks are meticulously palpated and marked. These include the acromion, the entire length of the scapular spine, and the medial border of the scapula. A linear skin incision, approximately 8 to 10 centimeters in length, is made parallel to and just superior (approximately 1 cm) to the spine of the scapula. The incision extends from the posterior aspect of the acromion medially toward the medial border of the scapula. Dissection is carried sharply through the subcutaneous tissue and superficial fat to expose the glistening deep fascia overlying the trapezius muscle. Hemostasis of the superficial dermal vessels is meticulously achieved using bipolar electrocautery.
2. Deep Dissection and Trapezius Mobilization
The trapezius fascia is incised in line with the skin incision. The critical step here is the detachment of the trapezius insertion from the superior aspect of the scapular spine. Using needle-tip electrocautery, the trapezius is carefully elevated off the bone. It is absolutely imperative to maintain a strict subperiosteal plane during this elevation to ensure a robust, thick tissue cuff of trapezius tendon remains for later transosseous repair. Poor or thin elevation of the trapezius will inevitably lead to postoperative dehiscence, resulting in profound weakness and a noticeable cosmetic deformity.
As the fibers of the trapezius and the underlying periosteum are elevated, a thin, fatty areolar layer becomes visible. This layer separates the undersurface of the trapezius from the underlying supraspinatus muscle fascia. The mobilized trapezius muscle is then retracted cephalad (superiorly) using a wide, blunt retractor, such as a Richardson or a specialized Kolbel retractor. This maneuver widely exposes the supraspinatus muscle belly residing within the suprascapular fossa. Crucially, the surgeon must not elevate the supraspinatus muscle from its fossa. Doing so risks devastating devascularization and denervation of the muscle belly.
3. Locating the Suprascapular Notch
With the supraspinatus exposed, the surgeon must navigate toward the suprascapular notch. Using blunt dissection—ideally with a wet, gloved index finger or a moist Kittner sponge—the surgeon gently palpates along the superior border of the scapula. The finger is swept from medial to lateral until the distinct U- or V-shaped bony depression of the suprascapular notch is palpated, along with the taut band of the overlying superior transverse scapular ligament. Only minimal distal (inferior) retraction of the supraspinatus muscle is required to visualize the notch. Aggressive over-retraction must be strictly avoided, as it can place excessive traction on the short motor branches supplying the supraspinatus, leading to iatrogenic neuropraxia.
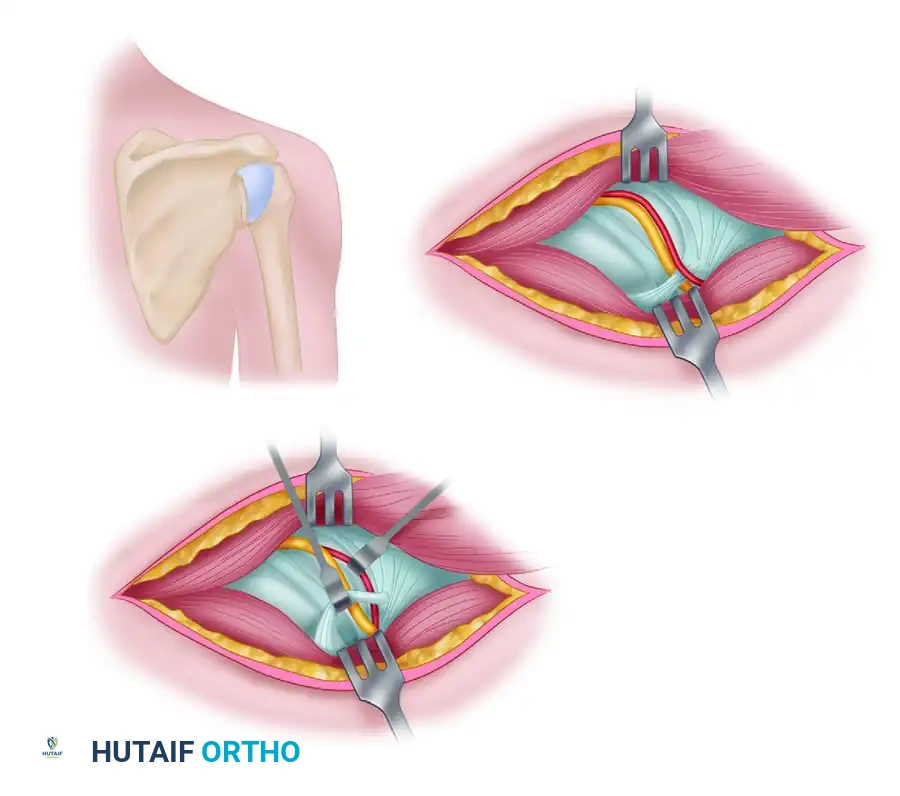
4. Isolation and Release of the Transverse Scapular Ligament
Once the suprascapular notch is definitively palpated and visualized, the surgeon uses a blunt elevator (such as a Freer or a small Cobb elevator) to meticulously clean the overlying fatty and areolar soft tissue off the transverse scapular ligament. This is the most perilous stage of the procedure due to the proximity of the suprascapular vessels. The suprascapular artery and vein, which run immediately superficial to the ligament, must be identified, skeletonized, and gently retracted superiorly or laterally using a vessel loop or a small blunt retractor.
Once the vessels are protected, a blunt nerve hook or a small right-angle clamp is carefully introduced under the transverse scapular ligament. This instrument serves as a mechanical barrier, protecting the underlying suprascapular nerve from inadvertent injury. With the nerve protected, the ligament is sharply released using a #15 scalpel blade or a 2mm Kerrison rongeur. If the ligament is heavily ossified, a small high-speed burr may be required to unroof the foramen. Further exploration of the nerve or extensive intraneural neurolysis is generally unnecessary and contraindicated. The primary goal is extrinsic decompression; excessive manipulation of the nerve itself can lead to iatrogenic axonotmesis.
5. Ganglion Cyst Excision and Decompression
Following the release of the ligament, the surrounding region is inspected and palpated to locate the ganglion cyst. The cyst often presents as a tense, bluish, or clear fluid-filled sac. Using meticulous blunt and sharp dissection, the cyst wall is separated from the surrounding areolar tissue and the adjacent nerve. If the cyst is massive and obscures the surgical field, it may be intentionally punctured with an 18-gauge needle and aspirated to decompress it. This reduces the cyst's volume and allows for easier, safer dissection of the remaining cyst wall. The surgeon must carefully trace the stalk of the cyst laterally and inferiorly toward its origin, which is invariably a capsular defect at the superior or posterior glenoid rim. Once the stalk is identified, it is securely ligated with a non-absorbable suture or thoroughly cauterized to seal the one-way valve and minimize the risk of postoperative recurrence.
6. Closure and Transosseous Trapezius Reattachment
The surgical field is copiously irrigated with sterile saline to remove any remaining cystic fluid and cellular debris. Absolute hemostasis must be achieved, paying particular attention to the suprascapular vessels and the muscular branches of the trapezius. The reattachment of the trapezius muscle to the spine of the scapula is a critical step that dictates the functional recovery of the shoulder girdle. A simple soft-tissue-to-soft-tissue repair is inadequate and prone to failure.
Instead, a secure transosseous repair must be performed. Several drill holes are placed along the superior edge of the scapular spine using a 2.0mm drill bit, spaced approximately 1.5 centimeters apart. Heavy, nonabsorbable, braided sutures (e.g., #2 FiberWire or Ethibond) are passed through these drill holes. The sutures are then passed through the robust fascial edge of the mobilized trapezius muscle utilizing a horizontal mattress configuration. The sutures are tied securely, bringing the trapezius tendon back to its exact anatomical footprint on the scapular spine. The deep fascial layers and subcutaneous tissue are closed in a routine, layered manner using absorbable sutures (e.g., 2-0 Vicryl). The skin is closed with a running subcuticular suture or surgical staples, depending on surgeon preference. A sterile, non-adherent dressing is applied, and the patient's arm is immediately placed in a standard shoulder sling for strict immobilization.
Complications, Incidence Rates, and Salvage Management
While the open posterior approach is generally safe and highly effective when performed by an experienced shoulder surgeon, it carries specific, potentially devastating risks that must be meticulously mitigated through rigorous surgical technique.
Iatrogenic Nerve and Vascular Injury
The most feared complication is iatrogenic injury to the suprascapular nerve. The nerve is highly vulnerable during the blind passage of instruments or during the sharp release of the transverse scapular ligament. Blind cutting of the ligament without a protective instrument (like a right-angle clamp) underneath is strictly prohibited. Injury to the nerve can range from transient neuropraxia due to traction, to complete axonotmesis or neurotmesis. Similarly, vascular injury to the suprascapular artery can cause rapid, significant hemorrhage. This not only obscures the surgical field but increases the risk of secondary nerve injury during frantic, blind attempts at hemostasis using electrocautery.
Trapezius Dehiscence
Failure to achieve a secure transosseous repair of the trapezius muscle is a catastrophic complication. If the repair fails, the trapezius retracts superiorly, leading to chronic, debilitating posterior shoulder pain, severe weakness in shoulder elevation and periscapular stabilization, and a highly visible cosmetic defect. Salvage management of a chronic trapezius dehiscence is exceedingly difficult and often requires complex fascial flap transfers or Achilles tendon allograft reconstructions to bridge the defect.
Incomplete Decompression and Cyst Recurrence
Failure to completely excise the cyst wall, failure to identify and ligate the cyst stalk, or failure to address a concomitant intra-articular labral tear significantly increases the risk of ganglion recurrence. If the capsulolabral "one-way valve" remains patent, synovial fluid will continue to extravasate, leading to the reformation of the cyst and the return of compressive neuropathy.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Iatrogenic Nerve Injury | 1% - 3% | Always use a protective instrument under the ligament; avoid excessive supraspinatus retraction. | Observation for neuropraxia; nerve grafting or transfers (e.g., spinal accessory nerve) for neurotmesis. |
| Suprascapular Artery Hemorrhage | 2% - 5% | Skeletonize and retract vessels before ligament release; avoid blind cautery. | Direct pressure, precise bipolar cautery, or formal vessel ligation. |
| Trapezius Dehiscence | 3% - 7% | Strict subperiosteal elevation; rigorous transosseous horizontal mattress repair. | Revision transosseous repair; Achilles allograft reconstruction for chronic retracted cases. |
| Cyst Recurrence | 5% - 15% | Complete stalk ligation; concurrent arthroscopic SLAP repair if indicated. | Revision open excision vs. arthroscopic intra-articular decompression and labral repair. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following an open excision of a suprascapular ganglion cyst requires a delicate, phased approach. The physical therapist and surgeon must balance the absolute necessity of protecting the transosseous trapezius repair with the imperative to prevent glenohumeral and scapulothoracic stiffness.
Phase I: Protection and Tissue Healing (Weeks 0–4)
The primary goal of the first four weeks is the protection of the trapezius reattachment. The patient must remain strictly immobilized in a standard shoulder sling for 4 to 6 weeks, removing it only for hygiene and specific, approved exercises. Active range of motion (AROM) of the elbow, wrist, and hand is encouraged immediately to prevent distal stiffness and promote venous return. Gentle, passive pendulum exercises may begin at week 2, provided they are performed without any active muscle contraction of the shoulder girdle. The patient is strictly instructed to avoid any active shoulder elevation, abduction, and any resisted movements of the shoulder, as these will place catastrophic tension on the healing trapezius repair.
Phase II: Early Motion and Scapular Mechanics (Weeks 4–8)
At the 4-to-6-week mark, assuming clinical evidence of adequate soft tissue healing, the sling is gradually weaned. The patient initiates formal physical therapy focusing on passive range of motion (PROM), slowly progressing to active-assisted range of motion (AAROM) in all planes (flexion, abduction, internal/external rotation). During this phase, the therapist places a heavy emphasis on restoring normal scapular kinematics. Gentle scapular retraction, depression, and stabilization exercises are initiated in a gravity-eliminated or supported position to awaken the periscapular musculature without overloading the trapezius footprint. Submaximal isometric exercises for the rotator cuff may begin late in this phase.
Phase III: Strengthening and Return to Function (Weeks 8–12+)
By week 8, the patient progresses to full active range of motion (AROM) against gravity. Once full, painless AROM is achieved, the protocol advances to isotonic strengthening of the rotator cuff, deltoid, and periscapular musculature. The rehabilitation must focus heavily on the specific recruitment of the supraspinatus and infraspinatus muscles, often utilizing electromyographic biofeedback to ensure the previously denervated muscles are firing correctly. Resistance is gradually increased using elastic bands and light free weights. Return to heavy lifting, overhead occupational activities, or overhead sports (e.g., throwing, serving) is typically permitted between 4 to 6 months postoperatively. This return to play is contingent upon the patient demonstrating a return of full, symmetrical strength, the absence of pain with provocative testing, and the restoration of normal scapulohumeral rhythm.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of suprascapular neuropathy secondary to ganglion cysts has undergone a significant evolution over the past three decades. Historically, the open posterior approach, as detailed in this chapter, was the undisputed gold standard. Landmark anatomical studies by Rengachary et al. in the late 1970s defined the morphology of the suprascapular notch and laid the foundation for understanding the mechanical basis of nerve entrapment. Subsequent clinical series in the 1980s and 1990s demonstrated that open excision of the cyst and release of the transverse scapular ligament reliably relieved pain and halted the progression of muscle atrophy.
However, the paradigm shifted dramatically with the advent of advanced shoulder arthroscopy. Seminal work by surgeons such as Romeo, Piasecki, and Cummins highlighted the pathophysiological link between SLAP tears and paralabral cyst formation. This led to the development of arthroscopic internal cyst decompression combined with labral repair. The literature now overwhelmingly supports arthroscopic management as the first-line surgical treatment for the vast majority of paralabral cysts, as it addresses the intra-articular root cause (the labral tear) while avoiding the morbidity of a large posterior incision and trapezius detachment.
Despite this shift, current clinical guidelines and contemporary operative texts (including Chapter 52 of major orthopedic references) firmly maintain that the open posterior approach remains an essential, non-obsolete technique. The literature dictates that the open approach is specifically indicated for massive cysts that cannot be reached or adequately decompressed via intra-articular arthroscopic portals, cysts with highly organized and fibrotic walls that resist aspiration, and cases of primary nerve entrapment by an ossified transverse scapular ligament where no labral pathology exists. By mastering both the intricate open anatomical approach detailed herein and modern arthroscopic techniques, the comprehensive orthopedic surgeon can ensure highly tailored, patient-specific management of complex suprascapular neuropathy.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).
