Comprehensive Introduction and Patho-Epidemiology
Suprascapular nerve entrapment is a profoundly debilitating, albeit relatively uncommon, compressive neuropathy that manifests primarily as posterior shoulder pain, functional impairment, and progressive upper extremity weakness. First comprehensively described in the orthopedic literature by Kopell and Thompson in 1959, this clinical entity has evolved from a poorly understood cause of "idiopathic" shoulder pain to a well-defined anatomical and pathological syndrome. While historical texts occasionally mislabel this condition as "subscapular" nerve entrapment due to typographical legacy or anatomical misunderstanding, the precise pathology occurs strictly along the course of the suprascapular nerve. The entrapment most frequently occurs at two distinct fibro-osseous bottlenecks: the suprascapular notch beneath the superior transverse scapular ligament, and the spinoglenoid notch beneath the spinoglenoid ligament (inferior transverse scapular ligament).
The patho-epidemiology of suprascapular nerve entrapment is highly dependent on the anatomical site of compression. Entrapment at the suprascapular notch typically results in a global denervation pattern affecting both the supraspinatus and infraspinatus muscles, often presenting with a deep, poorly localized aching pain that mimics cervical radiculopathy or advanced rotator cuff arthropathy. Conversely, entrapment at the spinoglenoid notch is uniquely characterized by isolated weakness and profound atrophy of the infraspinatus muscle, entirely sparing the supraspinatus. This distal compression is predominantly seen in specific demographic cohorts, most notably elite overhead athletes such as volleyball players, baseball pitchers, tennis players, and competitive weightlifters. The repetitive, high-velocity overhead motion, particularly during the deceleration phase of throwing or striking, subjects the nerve to extreme traction and microtrauma at the spinoglenoid fulcrum.
The most frequent structural etiology for compression at the spinoglenoid notch is the formation of a paralabral ganglion cyst. The pathophysiology of these cysts is intimately tied to intra-articular derangements. They typically arise from a pathological "one-way valve" mechanism created by a posterosuperior labral tear or a superior labrum anterior and posterior (SLAP) lesion. During the dynamic extremes of shoulder motion, particularly in abduction and external rotation, synovial fluid is hydraulically pumped from the pressurized glenohumeral joint through the capsulolabral defect into the paralabral space. Because the tissue architecture prevents the retrograde flow of fluid back into the joint, the fluid progressively accumulates in the confined space of the spinoglenoid notch. This expanding mass exerts direct, unrelenting mechanical pressure on the suprascapular nerve, leading to localized ischemia, impairment of axoplasmic transport, and subsequent Wallerian degeneration of the motor axons supplying the infraspinatus.
Beyond ganglion cysts, the patho-epidemiology encompasses other, less common etiologies that necessitate a thorough diagnostic workup. These include direct blunt trauma to the posterior shoulder leading to hematoma and subsequent fibrosis, traction injuries from massive rotator cuff tears (which alter the resting length and tension of the nerve), iatrogenic tethering following surgical procedures (such as open Bankart repairs or aggressive capsular plications), and primary neurogenic tumors such as schwannomas or neurofibromas. Understanding this diverse epidemiological and pathological spectrum is paramount for the orthopedic surgeon, as the underlying etiology dictates not only the surgical approach but the ultimate prognosis for neurological recovery.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the posterior shoulder anatomy and the intricate course of the suprascapular nerve is mandatory before undertaking any open or arthroscopic intervention. The suprascapular nerve is a mixed motor and sensory peripheral nerve that originates from the upper trunk of the brachial plexus, formed by the ventral rami of the fifth and sixth cervical nerve roots (C5, C6), with occasional and variable contributions from the fourth cervical root (C4). It diverges from the upper trunk at Erb's point, a critical anatomical landmark in the posterior triangle of the neck, and courses laterally and posteriorly, passing deep to the omohyoid muscle and the anterior border of the trapezius.
As the nerve approaches the superior border of the scapula, it enters its first major zone of potential entrapment: the suprascapular notch. This notch is bridged by the superior transverse scapular ligament. The anatomical configuration of this notch is highly variable, famously categorized by Rengachary into six distinct types ranging from a wide, U-shaped depression to a completely ossified foramen. The suprascapular nerve classically passes inferior to the transverse scapular ligament, directly through the notch, while the suprascapular artery and vein pass superior to the ligament. This anatomical separation is a critical surgical landmark; however, the surgeon must remain vigilant for anatomical variants where the artery passes through the notch alongside the nerve, increasing the risk of catastrophic vascular injury during blind decompression.
Upon exiting the suprascapular notch, the nerve enters the supraspinous fossa, where it provides two critical motor branches to the supraspinatus muscle. It also gives off sensory articular branches that ascend to innervate the acromioclavicular joint and the posterior capsule of the glenohumeral joint. The main trunk of the nerve then descends obliquely along the bony floor of the supraspinous fossa, tracking laterally toward the base of the scapular spine. It wraps around the lateral margin of the scapular spine to enter the spinoglenoid notch. This acute angulation around the bone acts as a mechanical fulcrum, subjecting the nerve to significant tension during dynamic shoulder movements.
Within the spinoglenoid notch, the nerve passes beneath the spinoglenoid ligament (also known as the inferior transverse scapular ligament). Anatomical studies by Plancher and others have demonstrated that this ligament is a distinct fibrous band present in approximately 50% to 80% of the population. Unlike the suprascapular notch, the suprascapular artery and vein typically accompany the nerve through the spinoglenoid notch, running superficial or adjacent to the ligament. After traversing this space, the nerve arborizes into three to four terminal motor branches that innervate the infraspinatus muscle. Biomechanically, the nerve is highly vulnerable in this region. Cross-body adduction and extreme internal rotation cause the spinoglenoid ligament to become taut, creating a "sling effect" that acutely compresses the nerve against the bony floor of the notch. This biomechanical reality explains the high prevalence of this specific entrapment neuropathy in athletes whose sports demand repetitive, forceful follow-through motions.
Exhaustive Indications and Contraindications
The decision-making process for selecting the open posterior surgical approach over modern arthroscopic techniques requires a nuanced understanding of the patient's specific pathology, the anatomical location of the compression, and the underlying etiology. While arthroscopic management has become the gold standard for intra-articular pathologies causing secondary nerve compression, the open approach remains an indispensable, definitive procedure for a distinct subset of complex clinical scenarios.
The primary indication for the open posterior approach is the presence of a massive, multiloculated paralabral ganglion cyst that extends far medially into the infraspinous fossa, beyond the safe reach of arthroscopic instruments. Similarly, cysts that demonstrate no identifiable intra-articular communication on advanced imaging (MRI arthrogram) or during diagnostic arthroscopy cannot be adequately decompressed via an articular marsupialization and must be excised openly. Solid space-occupying lesions, such as schwannomas, neurofibromas, lipomas, or primary bone tumors encroaching on the spinoglenoid notch, absolutely mandate an open approach to ensure complete, oncologically sound excision and meticulous neurolysis. Furthermore, cases of primary nerve entrapment caused by an isolated, hypertrophied spinoglenoid ligament in the absence of any labral pathology are optimally managed through a targeted open or mini-open posterior incision.
Contraindications to the open posterior approach are equally critical to recognize. The procedure is strictly contraindicated in the presence of active, untreated local or systemic infection. It is relatively contraindicated in patients with purely intra-articular pathology (e.g., a simple posterior labral tear with a small, localized cyst) that is highly amenable to arthroscopic repair and decompression. Subjecting such a patient to the morbidity of an open muscle-splitting or muscle-detaching approach violates the principles of minimally invasive surgery. Additionally, patients with advanced, irreversible fatty infiltration of the infraspinatus (Goutallier stage 3 or 4) combined with long-standing, profound denervation on electromyography (EMG) may not experience meaningful motor recovery, making the procedure a palliative endeavor for pain relief rather than a restorative one.
| Indication / Contraindication | Rationale / Pathophysiological Basis | Clinical Scenario / Example |
|---|---|---|
| Indication: Massive, multiloculated cysts | Arthroscopic reach is limited medially; risk of incomplete decompression and high recurrence. | A 45-year-old laborer with a 4 cm cyst extending into the medial infraspinous fossa. |
| Indication: Solid tumors (e.g., Schwannoma) | Requires meticulous, direct visualization for enucleation without sacrificing the parent nerve fascicles. | MRI reveals an enhancing, solid, fusiform mass in the spinoglenoid notch. |
| Indication: Iatrogenic nerve tethering | Scar tissue and altered anatomy from prior open surgery require meticulous, layer-by-layer open dissection. | Persistent severe posterior pain and new weakness following an open posterior capsular shift. |
| Indication: Failure of arthroscopic decompression | Persistent valving mechanism or inadequate capsulotomy necessitates direct excision of the cyst stalk. | Recurrent ganglion cyst 6 months post-arthroscopic labral repair and cyst marsupialization. |
| Contraindication: Purely intra-articular pathology | Morbidity of open approach outweighs benefits when arthroscopy can address the root cause (labral tear). | A 22-year-old pitcher with a posterior SLAP tear and a small, 1 cm paralabral cyst. |
| Contraindication: Active local infection | Surgical dissection through infected tissue planes can seed the deep posterior compartments and joint space. | Overlying cellulitis or a draining sinus tract on the posterior aspect of the shoulder. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of a successful open posterior decompression. The clinical evaluation must be meticulous. Patients typically present with a vague, deep-seated, aching pain in the posterior aspect of the shoulder, which frequently radiates down the arm or proximally into the posterolateral neck. The hallmark physical examination finding is profound weakness in external rotation with the arm positioned strictly at the side (to isolate the infraspinatus and eliminate the contribution of the posterior deltoid). This is almost universally accompanied by visible hollowing of the infraspinous fossa due to muscle atrophy. The "cross-body adduction test" may exacerbate the pain by stretching the nerve against the spinoglenoid ligament.
Diagnostic modalities are critical for confirming the clinical suspicion and mapping the surgical anatomy. Electromyography (EMG) and Nerve Conduction Studies (NCS) remain the physiological gold standard. Findings will classically demonstrate denervation potentials—such as fibrillations and positive sharp waves—isolated entirely to the infraspinatus muscle, while the supraspinatus remains electrically normal. Nerve conduction studies will show prolonged latencies or decreased amplitudes of the suprascapular nerve when stimulating at Erb's point and recording specifically over the infraspinatus motor point.
Magnetic Resonance Imaging (MRI) without and with intra-articular contrast (MR Arthrogram) is the anatomical gold standard. High-resolution MRI not only visualizes the space-occupying lesion with exquisite detail but also identifies the underlying intra-articular pathology, such as a posterior labral tear or SLAP lesion. Furthermore, T1-weighted sagittal oblique sequences are essential for assessing the degree of fatty infiltration in the rotator cuff musculature (Goutallier classification), which directly correlates with the prognosis for post-operative motor recovery.
The following MR images demonstrate the classic presentation of a paralabral ganglion cyst causing entrapment neuropathy of the suprascapular nerve at the spinoglenoid notch:

FIGURE 46-16A: Axial MR image. Arrowheads indicate a small, low-density shadow situated just posterior to the neck of the glenoid, representing the early formation of a paralabral cyst.

FIGURE 46-16B: Sagittal/Coronal oblique MR image. The solid black arrow highlights a distinct ganglion cyst residing within the region of the spinoglenoid notch, exerting mass effect on the neurovascular bundle.
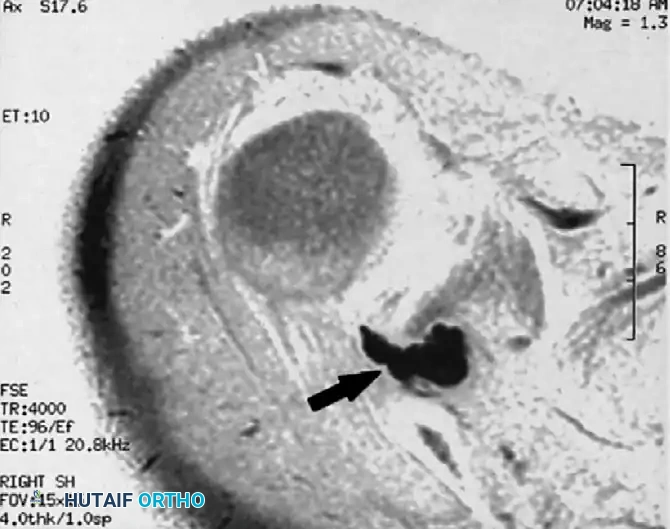
FIGURE 46-16C: Axial MR image demonstrating a large, multiloculated ganglion cyst (arrow). The cyst clearly appears to originate from the posterosuperior aspect of the glenohumeral joint, tracking posteriorly to fill the spinoglenoid notch.
Patient positioning for the open posterior approach requires careful consideration of the surgeon's preference and the need for concurrent procedures. The patient is typically placed in either a lateral decubitus position with a slight anterior tilt (semiprone) or a full prone position. The lateral decubitus position is highly favored in modern practice as it allows for a seamless transition from a diagnostic or therapeutic arthroscopy to the open posterior approach without the need for reprepping and redraping. The operative arm must be draped completely free to allow for full, unhindered manipulation during the procedure. Internal rotation and cross-body adduction of the arm can be utilized dynamically during the surgery to bring the posterior muscular structures under tension, facilitating easier identification of fascial planes and the spinoglenoid interval. Precise landmark identification is critical; the surgeon must palpate and mark the entire length of the scapular spine, the posterolateral corner of the acromion, and the posterior joint line prior to incision.
Step-by-Step Surgical Approach and Fixation Technique
The open posterior approach to the spinoglenoid notch is a technically demanding procedure that requires strict adherence to anatomical planes to prevent catastrophic iatrogenic injury. The technique detailed herein is a comprehensive synthesis of established methodologies, primarily drawing from the foundational work of Post and Mayer, as well as the deeper exposure techniques popularized by Thompson, Schneider, and Kennedy.
Superficial Dissection and Trapezius Management
The initial exposure focuses on safely navigating the superficial muscular layers to access the bony landmark of the scapular spine. A linear or slightly curvilinear incision, approximately 10 to 12 cm in length, is made parallel and approximately 1 to 2 cm cephalad (superior) to the spine of the scapula, extending from the medial border of the acromion toward the vertebral border of the scapula. The incision is carried sharply through the skin and subcutaneous adipose tissue to expose the thick, investing deep fascia overlying the trapezius muscle.
The fascia is incised in line with the skin incision. At this juncture, the surgeon must decide between splitting the trapezius fibers or elevating the muscle entirely. For isolated spinoglenoid notch pathology, elevating the lower fibers of the trapezius off the scapular spine often provides superior, unhindered visualization. Using electrocautery, the trapezius insertion is meticulously detached from the superior aspect of the scapular spine, leaving a small cuff of tendinous tissue on the bone to facilitate robust closure. The posterior shoulder is highly vascular, and meticulous hemostasis of the muscular perforators is mandatory to maintain a clear surgical field. The trapezius is then retracted superiorly and medially. The surgeon must be highly cognizant of the spinal accessory nerve (Cranial Nerve XI) and the transverse cervical artery, which lie medial and superior to the operative field; aggressive medial dissection or blind retractor placement in this quadrant must be strictly avoided.
Deep Exposure: Infraspinatus Reflection
Once the scapular spine is cleared and the trapezius is secured, the focus shifts to the infraspinous fossa and the underlying infraspinatus muscle. The thick infraspinatus fascia is incised sharply. To access the spinoglenoid notch, the infraspinatus muscle must be mobilized. Historically, some authors advocated for a medial detachment of the muscle from the vertebral border of the scapula. However, contemporary techniques favor a superior and partial medial detachment from the scapular body, allowing the muscle to be reflected laterally and inferiorly.
Using a Cobb elevator and electrocautery, the superior origin of the infraspinatus is carefully elevated off the bony floor of the supraspinous fossa, moving from medial to lateral. As the muscle is reflected laterally, the surgeon will expose the posterior capsule of the glenohumeral joint and the posterior neck of the glenoid. It is during this reflection that the utmost caution is required. The suprascapular neurovascular bundle lies intimately against the bony floor, tethered at the spinoglenoid notch. Excessive or forceful lateral retraction of the infraspinatus can cause severe iatrogenic traction injury (axonotmesis or neurotmesis) to the terminal motor branches of the nerve.
Decompression and Neurolysis at the Spinoglenoid Notch
With the infraspinatus safely reflected, the surgeon palpates the lateral base of the scapular spine to definitively locate the spinoglenoid notch. The operative field is carefully cleared of overlying fibro-fatty connective tissue using blunt dissection and delicate bipolar electrocautery. The suprascapular artery and vein are typically encountered first, running superficial to the ligament; these vessels must be carefully mobilized and protected, or selectively ligated if they obscure the surgical field or are intimately involved with the pathology.
If a ganglion cyst is the source of compression, it will often present as a bluish, tense, multi-lobulated cystic structure filling the notch. The primary surgical objective is to meticulously dissect the ganglion cyst away from the suprascapular nerve, leaving the nerve entirely intact and uninjured. The nerve should be identified proximally in normal, unscarred tissue within the lateral supraspinous fossa and traced distally into the zone of compression. The cyst is carefully separated from the epineurium using tenotomy scissors or a micro-dissector. Once the nerve is freed, the stalk of the cyst must be traced to its origin at the posterior glenohumeral joint capsule. The stalk is then ligated with a non-absorbable suture or aggressively cauterized to eradicate the one-way valve mechanism and minimize the risk of recurrence. If the pathology is a hypertrophied spinoglenoid ligament without a cyst, a right-angle clamp is passed deep to the ligament to protect the nerve, and the ligament is sharply sectioned, ensuring complete unroofing of the fibro-osseous tunnel.
Following thorough decompression, the surgical site is copiously irrigated. The infraspinatus is allowed to return to its anatomical bed and is repaired to its fascial origins using heavy absorbable sutures. The trapezius is meticulously reapproximated to the cuff of tissue left on the scapular spine using a running or interrupted locking stitch. A subfascial drain is strongly recommended due to the vast dead space and the highly vascular nature of the muscle beds, which predisposes the patient to post-operative hematoma formation. The subcutaneous tissues and skin are closed in a standard layered fashion.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the open posterior approach carries a distinct profile of potential complications. The deep, complex anatomy and the inherent vulnerability of the suprascapular nerve make this a high-stakes procedure where technical errors can lead to profound functional deficits. Surgeons must be intimately familiar with these risks, their estimated incidences, and the appropriate salvage strategies.
The most devastating complication is iatrogenic injury to the suprascapular nerve. This can occur via direct transection during blind excision of a cyst, thermal necrosis from errant electrocautery, or traction neuropraxia from aggressive retraction of the infraspinatus muscle. Incomplete decompression is another significant pitfall, often resulting from a failure to fully trace a multiloculated cyst to its articular origin or a failure to completely release a thick, broad spinoglenoid ligament. This leads to persistent pain and ongoing denervation.
Hematoma formation is a frequent concern due to the extensive muscular dissection required to expose the scapular spine and the infraspinous fossa. A large, expanding hematoma can not only lead to localized pain and delayed wound healing but can also act as a secondary space-occupying lesion, causing recurrent compression of the nerve. Furthermore, if the underlying intra-articular pathology (the capsulolabral defect) is not addressed—a known limitation of an isolated open approach without concurrent arthroscopy—the ganglion cyst has a high propensity to recur as the one-way valve mechanism remains active.
| Complication | Estimated Incidence | Prevention and Salvage Management Strategy |
|---|---|---|
| Iatrogenic Nerve Injury | 1% - 3% | Prevention: Identify nerve proximally in normal tissue; avoid aggressive retraction; use bipolar cautery. Salvage: Immediate microsurgical epineural repair or nerve grafting if transected; observation and serial EMGs for traction neuropraxia. |
| Incomplete Decompression | 5% - 8% | Prevention: Direct visualization of the entire spinoglenoid notch; complete sectioning of the ligament. Salvage: Revision open decompression with extensive neurolysis; consider concurrent arthroscopic evaluation. |
| Cyst Recurrence | 10% - 15% (Open alone) | Prevention: Ligate/cauterize the cyst stalk at the capsule; ideally, perform concurrent arthroscopic labral repair. Salvage: Arthroscopic labral repair and capsulotomy to close the valve mechanism. |
| Post-operative Hematoma | 3% - 6% | Prevention: Meticulous hemostasis of muscular perforators; routine use of a closed-suction subfascial drain. Salvage: Early operative evacuation, irrigation, and formal hemostasis if expanding or causing neurological compromise. |
| Adhesive Capsulitis / Stiffness | 5% - 10% | Prevention: Early, controlled passive range of motion; avoidance of prolonged immobilization. Salvage: Aggressive physical therapy; intra-articular corticosteroid injections; arthroscopic capsular release for refractory cases. |
Phased Post-Operative Rehabilitation Protocols
Postoperative rehabilitation following an open posterior approach for suprascapular nerve decompression is a delicate balancing act. The protocol must protect the healing, surgically reattached musculature (specifically the trapezius and the infraspinatus origins) while aggressively preventing the onset of adhesive capsulitis in the glenohumeral joint. Patient education is paramount; the surgeon must set realistic expectations, explicitly counseling the patient that while relief of the deep posterior aching pain is often rapid (within days to weeks), the return of infraspinatus muscle bulk and external rotation strength may take anywhere from 6 to 12 months, and in cases of severe preoperative atrophy, full recovery may never be achieved.
Phase I: Immediate Postoperative Protection Phase (Weeks 0-4)
The primary goal of this phase is to protect the surgical repair and manage pain and inflammation.
* Immobilization: The operative arm is placed in a standard shoulder sling or an abduction pillow sling, depending on the extent of the muscular detachment, to be worn continuously except for hygiene and exercises.
* Range of Motion (ROM): Active motion of the elbow, wrist, and hand is encouraged immediately to prevent distal edema. Gentle, passive range of motion (PROM) and active-assisted range of motion (AAROM) of the shoulder in forward elevation and internal rotation are initiated within the first 10 to 14 days.
* Strict Restrictions: Active external rotation and active overhead elevation are strictly prohibited to protect the healing infraspinatus and trapezius fascial repairs from tension failure.
Phase II: Intermediate Motion and Early Activation Phase (Weeks 4-8)
As the soft tissues achieve clinical healing, the focus shifts to restoring full mobility and initiating early muscle activation.
* ROM Progression: The sling is gradually weaned. Active motion is introduced and progressed as pain permits. The physical therapist focuses on restoring full passive, active-assisted, and active ROM in all planes.
* Strengthening: Gentle, submaximal isometric exercises are initiated for the deltoid, subscapularis, and the intact supraspinatus. Scapular stabilization exercises (e.g., scapular retractions, shrugs) are introduced to re-establish normal scapulothoracic kinematics.
Phase III: Advanced Strengthening and Neuromuscular Re-education (Weeks 8-16)
Once full, painless ROM is achieved and the muscular reattachments are structurally sound, progressive isotonic strengthening is initiated.
* Targeted Therapy: Specific, progressive resistance exercises targeting the infraspinatus and the posterior deltoid are the hallmark of this phase. Theraband exercises and light dumbbells are utilized for external rotation strengthening, initially with the arm at the side, and eventually progressing to the 90/90 position (abduction/external rotation) as tolerated.
* Neurological Monitoring: Clinical assessment of external rotation strength is performed monthly. If no improvement is noted by 4 to 6 months post-operatively, a repeat EMG may be indicated to assess for ongoing denervation or early signs of reinnervation (nascent motor unit potentials).
Phase IV: Return to Sport / Heavy Labor (Months 4-6+)
This final phase is highly individualized based on the patient's specific functional demands.
* Plyometrics and Dynamic Stability: For athletes, overhead plyometrics, throwing programs, and sport-specific kinetic chain exercises are implemented.
* Clearance Criteria: Return to full, unrestricted activity or competitive overhead sports is permitted only when the patient demonstrates pain-free full ROM, normal scapulothoracic rhythm, and external rotation strength that is at least 85% to 90% of the contralateral, uninjured side.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the surgical management of suprascapular nerve entrapment is deeply rooted in a rich history of anatomical and clinical research. The seminal work by Kopell and Thompson (1959) first brought the concept of peripheral nerve entrapment at the suprascapular notch to the forefront of orthopedic thought. Decades later, Rengachary et al. (1979) provided the definitive anatomical classification of the suprascapular notch, a framework that continues to guide surgeons in understanding the structural predispositions to proximal entrapment.
Regarding the spinoglenoid notch and the posterior surgical approach, the foundational techniques described by Post and Mayer established the standard for safe, reproducible access to the posterior shoulder. Their emphasis on meticulous fascial dissection and protection of the vascular leash remains highly relevant. Further anatomical studies by Plancher et al. elucidated the high prevalence of the spinoglenoid ligament, proving that mechanical compression could occur in the absence of a space-occupying cyst, thereby validating the need for surgical release in refractory cases of isolated infraspinatus wasting.
The paradigm shift toward arthroscopic management was heavily influenced by the work of Lafosse, who pioneered the entirely endoscopic release of the suprascapular nerve, and numerous sports medicine researchers who definitively linked paralab
