Posterolateral Arthrodesis for Spondylolisthesis: An Intraoperative Masterclass

Key Takeaway
This intraoperative masterclass guides fellows through posterolateral arthrodesis for spondylolisthesis. We cover comprehensive surgical anatomy, meticulous preoperative planning, and a granular, real-time breakdown of surgical execution. Learn precise instrument use, critical neurovascular considerations, and strategies for managing intraoperative challenges. Postoperative rehabilitation and complication management are also detailed, ensuring a holistic understanding of this complex procedure.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and to this definitive masterclass on spinal stabilization. Today, we are undertaking a comprehensive, highly technical exploration of a challenging yet profoundly rewarding procedure: Posterolateral Arthrodesis for Spondylolisthesis. Recognized universally as the gold standard for stabilizing the lumbar spine in specific spondylolisthesis presentations, this surgical intervention is particularly indicated for patients exhibiting mechanical instability without the profound neurologic compromise that inherently mandates a concurrent, aggressive direct decompression. The mastery of this procedure requires not only technical surgical dexterity but also a profound, academic understanding of the underlying pathoanatomy and biomechanics of the lumbosacral junction.
Before a scalpel is ever lifted, a rigorous, exhaustive understanding of spondylolisthesis is absolutely paramount for the operating surgeon. Spondylolisthesis, defined biomechanically, refers to the pathologic translation of one vertebra in relation to its adjacent caudal counterpart within the sagittal plane. While a significant proportion of the general population may harbor low-grade, asymptomatic slips discovered incidentally, the typical clinical presentation we encounter in the surgical clinic is characterized by mechanical, low-grade back pain. Radicular symptoms, while possible, are less frequent in early or low-grade presentations and typically manifest only when neuroforaminal stenosis or dynamic instability reaches a critical threshold.
To effectively plan surgical intervention, we must meticulously differentiate between the primary etiologies, most notably relying on the Wiltse classification. Isthmic spondylolisthesis, the most common variant encountered in the adolescent and young adult populations, is fundamentally the result of chronic, repetitive biomechanical loading acting upon a pars interarticularis that is genetically predisposed to fatigue failure. It is an acquired defect, a stress fracture that fails to achieve bony union, leading to a functional disconnection between the anterior and posterior columns of the affected vertebra. Conversely, dysplastic spondylolisthesis is secondary to congenital anomalies of the lumbosacral articulation. This often involves maloriented, sagittally aligned, or hypoplastic facet joints coupled with sacral deficiency. In dysplastic variants, the pars interarticularis is poorly developed and attenuated, leading to elongation or eventual macroscopic separation and subsequent forward slippage.
Crucially, dysplastic slips carry a significantly higher prognostic frequency of rapid progression. These patients are statistically more likely to present with insidious neurologic deficits and almost invariably require operative stabilization to halt progressive deformity. In both the pediatric and adolescent demographic, this condition exhibits a striking predilection for the L5–S1 junction, where the fifth lumbar vertebral body translates anteriorly over the sacral promontory, driven by the inherent shear forces dictated by the lumbosacral angle and individual pelvic morphology. Understanding these distinct pathophysiologic pathways dictates our surgical approach, our choice of instrumentation, and our postoperative expectations.
Detailed Surgical Anatomy and Biomechanics
Osteology and the Pars Interarticularis
A profound mastery of the surgical anatomy of the lumbosacral junction is the bedrock of a successful posterolateral arthrodesis. The pars interarticularis is the anatomic crux of this pathology. This critical, dense bony bridge resides between the superior and inferior articular processes, encompassing portions of the lamina, transverse processes, and the pedicle itself. Its structural integrity is vital for resisting anterior shear forces. In isthmic spondylolisthesis, the defect (spondylolysis) or severe elongation of this structure is the primary anatomic failure. When approaching this region surgically, identifying the fibrocartilaginous pseudarthrosis at the pars defect is essential, as it dictates the boundaries of our decortication and graft placement.
At the L5-S1 junction, longstanding biomechanical instability induces profound morphologic changes in the local osteology. The superior endplate of the sacrum, subjected to chronic, abnormal shear and compressive forces, frequently remodels to become dome-shaped. Concurrently, the inferior endplate of L5 adapts by becoming concave, often developing a prominent osteophytic "beak" at its anteroinferior corner. This beaking is a radiographic and anatomic hallmark of chronic instability and attempts at auto-stabilization. Furthermore, the transverse processes of L5 are frequently hypoplastic, presenting a uniquely challenging anatomic landscape. They are often situated deep within the surgical field, obscured by hypertrophic paraspinal musculature and the overarching iliac crests, making the identification of anatomic landmarks for pedicle screw placement exceptionally demanding.
Neurologic and Soft Tissue Considerations
The neurologic anatomy in the setting of spondylolisthesis is highly distorted and requires meticulous attention to avoid catastrophic iatrogenic injury. The L5 nerve roots exit through the L5-S1 neuroforamina and course anterior to the sacral ala. In the presence of a high-grade slip, these nerve roots are often stretched and draped tautly over the remodeled dome of the sacrum. This anatomic distortion renders the L5 nerve root exquisitely vulnerable to traction injuries, particularly during any surgical maneuvers aimed at reducing the translation. The surgeon must operate with the understanding that the extraforaminal segment of the L5 root is already under significant physiologic tension.
Another critical anatomic feature is the "Gill fragment." In cases of bilateral pars defects, the posterior elements of L5—comprising the spinous process and the bilateral laminae—become mechanically detached from the anterior vertebral body. This isolated bony complex, the Gill fragment, often remains tethered to the adjacent structures via the ligamentum flavum and facet capsules, but it floats independently of the L5 body. While it may contribute to localized compression of the dural sac or nerve roots via hypertrophic fibrocartilage at the defect site, its removal (the Gill procedure) must be carefully considered, as it simultaneously removes a substantial surface area that could otherwise be utilized for posterolateral bony fusion.
Exhaustive Indications and Contraindications
Clinical Presentation and Patient Evaluation
The decision to proceed with operative intervention is predicated on a rigorous clinical evaluation correlating with advanced imaging. The classic physical finding is an insidious onset of low back pain, which may occasionally radiate to the buttock or posterior thigh, mimicking radiculopathy but often representing somatic referred pain from the disrupted pars or degenerated disc. A hallmark physical sign is profound hamstring tightness, leading to a characteristic mild crouched gait. Popliteal angles greater than 40 degrees are highly indicative of significant hamstring contracture and represent the most common objective neurologic finding in these patients.
Visually, patients often present with flattened lumbar lordosis and a compensatory vertical pelvis. In high-grade slips, the torso may appear shortened, resulting in a characteristic "heart-shaped" appearance of the buttocks. A critical, palpable clinical finding is a step-off at the spinous processes of the involved levels. Because the posterior arch of L5 (the Gill fragment) remains relatively stationary while the L5 body slips anteriorly, the palpable step-off is actually felt between the spinous processes of L4 and L5.


Range of motion is characteristically limited; lumbar flexion and extension are restricted, and forced hyperextension frequently elicits sharp, localized pain. A comprehensive neurologic examination—including meticulous lumbar sensory and motor root testing, deep tendon reflexes, and abdominal reflexes—is mandatory. Rectal examination to assess sphincter tone is absolutely indicated in patients exhibiting any signs of bowel or bladder dysfunction, a rare but devastating complication of high-grade slips indicating cauda equina compromise.
Surgical Decision Making
We consider a multitude of factors when assessing the risk of slip progression and the absolute need for surgery. Key risk factors for progression include diagnosis prior to the adolescent growth spurt, female gender, and a baseline slip greater than 50%. Nonoperative management—comprising activity modification, targeted physiotherapy emphasizing core stabilization and hamstring stretching, and occasionally rigid bracing—remains our first line of defense for low-grade, minimally symptomatic slips. However, when nonoperative measures fail, or when faced with high-risk anatomic parameters, surgery is indicated.
| Category | Spondylolisthesis Surgical Parameters |
|---|---|
| Absolute Indications | Progressive neurologic deficit (motor weakness, bowel/bladder dysfunction); Documented progression of slip > 50% in a growing child; Intractable pain failing > 6 months of rigorous nonoperative care. |
| Relative Indications | Slip > 50% (Meyerding Grade III-V) even if asymptomatic (due to high risk of progression); Persistent, severe hamstring tightness altering gait mechanics; Slip angle > 50 degrees. |
| Absolute Contraindications | Active systemic or localized spinal infection; Severe medical comorbidities precluding safe general anesthesia; Complete absence of symptoms in a skeletally mature patient with a stable, low-grade slip. |
| Relative Contraindications | Severe osteoporosis (compromising hardware purchase); Active smoking (significantly increases pseudarthrosis rate); Unrealistic patient expectations regarding postoperative pain relief. |
The decision to perform an in-situ fusion versus a reduction is one of the most debated topics in spinal surgery. In-situ posterolateral arthrodesis is exceptionally safe and highly effective for halting progression and resolving pain in low-to-moderate grade slips. Reduction maneuvers, while restoring sagittal balance and potentially improving the biomechanical environment for fusion, carry a significantly elevated risk of L5 nerve root neuropraxia due to the stretching of the already taut nerve over the sacral dome.
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Radiographic Analysis
Our preoperative imaging protocol serves as the definitive roadmap for this complex surgery; meticulous planning here prevents intraoperative catastrophes. The foundation is standing posteroanterior (PA) and lateral radiographs of the entire spine. The PA view is scrutinized for coexisting scoliosis, which is often a non-structural, compensatory curve secondary to asymmetric paraspinal muscle spasm. The standing lateral view is paramount for assessing global sagittal balance, utilizing modern spino-pelvic parameters including Pelvic Incidence (PI), Pelvic Tilt (PT), and Sacral Slope (SS). A spot lateral view of the lumbosacral junction is critical for identifying the specific morphology of the spondylolytic defects and accurately quantifying the degree of spondylolisthesis.
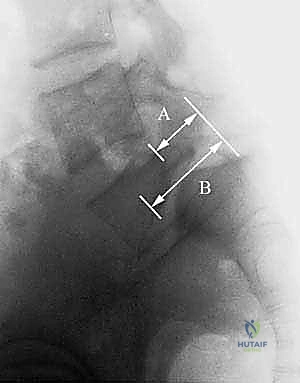
We universally apply the Meyerding Classification to quantify the forward translation of L5 on S1 based on the percentage of subluxation over the sacral endplate (Grade I: <25%, Grade II: 25-50%, Grade III: 50-75%, Grade IV: 75-100%, Grade V: >100% or spondyloptosis).

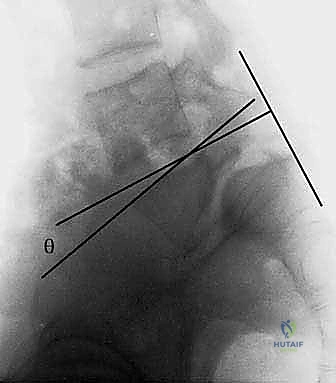
Equally important is the Slip Angle, subtended by the intersection of a line drawn along the superior endplate of L5 and the perpendicular of a line drawn along the posterior cortex of the sacrum. A slip angle exceeding 50 degrees is highly predictive of future instability, slip progression, and postoperative pseudarthrosis due to high local shear forces.

Advanced Imaging Modalities
Beyond plain radiography, advanced cross-sectional imaging is mandatory. Computed Tomography (CT) with fine-cut sagittal, coronal, and 3D reconstructions is the gold standard for defining the complex bony pathoanatomy. It allows for precise evaluation of cortical disruption, the extent of lysis, the presence of sclerosis at the pars, and the morphology of the pedicles for screw templating.

Magnetic Resonance Imaging (MRI), while less sensitive for the bony defect itself, is indispensable for evaluating the neural elements and the adjacent intervertebral discs. Specifically, we must assess the health of the L4–L5 disc. If this adjacent disc exhibits significant desiccation or degeneration on T2-weighted sagittal MRI, the surgeon must strongly consider extending the fusion construct to L4 to prevent rapid adjacent segment disease. Furthermore, MRI assesses any posterior protrusion of the L5–S1 disc, which, if present, could lead to catastrophic cauda equina compression during any reduction maneuvers.

Positioning and Templating
Patient positioning is a critical, active step in the surgical procedure. The patient is placed prone on a radiolucent Jackson spinal table. The abdomen must hang completely free to minimize intra-abdominal pressure, thereby reducing epidural venous engorgement and subsequent intraoperative blood loss. Careful padding of all bony prominences is mandatory to prevent positioning neuropathies.
Prior to draping, intraoperative fluoroscopy is utilized to confirm the surgical levels and optimize the C-arm trajectory. We mandate the use of comprehensive intraoperative neuromonitoring, including baseline and continuous somatosensory evoked potentials (SSEPs), motor evoked potentials (MEPs), and free-run electromyography (EMG). These modalities are crucial for real-time assessment of neural integrity, particularly when placing instrumentation in dysplastic pedicles or if any degree of reduction is attempted.
Step-by-Step Surgical Approach and Fixation Technique
Exposure and Soft Tissue Dissection
The surgical approach begins with a meticulously planned midline longitudinal incision, typically extending from the spinous process of L4 down to the mid-sacrum, ensuring adequate length for bilateral posterolateral exposure. The subcutaneous tissues are divided in line with the incision using electrocautery, maintaining strict hemostasis. The lumbodorsal fascia is incised longitudinally, slightly off-midline bilaterally, to preserve the supraspinous and interspinous ligamentous complex if an in-situ fusion without decompression is planned.

A meticulous, subperiosteal dissection of the paraspinal musculature is then performed using Cobb elevators and monopolar electrocautery. The dissection proceeds laterally over the laminae, the facet joints, and finally out to the tips of the transverse processes of L5 and the sacral ala. Achieving a clean, bloodless exposure of the transverse processes is critical, as this forms the primary bed for our posterolateral fusion mass. In spondylolisthesis, the L5 transverse processes are often deeply recessed and hypoplastic; the surgeon must carefully navigate the iliolumbar ligament and avoid straying anteriorly, which risks injury to the exiting L4 and L5 nerve roots or the retroperitoneal vasculature.

Instrumentation and Decortication
Once the bony anatomy is definitively exposed and the pars defects are identified, we proceed with instrumentation. Pedicle screws are the standard of care, providing rigid three-column fixation that obviates the need for postoperative casting and significantly enhances fusion rates. The entry point for the L5 pedicle screw is typically at the intersection of the pars interarticularis, the base of the superior articular process, and the transverse process. Given the distorted anatomy, a gearshift probe is used with extreme caution to cannulate the pedicle, constantly palpating the medial, lateral, superior, and inferior bony walls to ensure no cortical breaches occur.
The S1 pedicle screws are directed medially toward the sacral promontory, often utilizing a bi-cortical purchase for maximum pull-out strength. Following screw placement, the entire posterolateral bony bed—including the transverse processes of L5, the lateral aspect of the pars, the facet joints, and the sacral ala—undergoes rigorous decortication. Using a high-speed matchstick burr and sharp curettes, the cortical bone is systematically removed until bleeding cancellous bone is exposed. This step cannot be rushed; a robust, bleeding bony bed is the absolute prerequisite for a successful osteoinductive and osteoconductive fusion response.
Grafting and Closure
With the bed prepared, the bone graft is applied. While local bone from the spinous processes and laminae (if a Gill procedure was performed) is utilized, it is rarely sufficient in volume. Therefore, autologous cancellous bone harvested from the posterior superior iliac spine (PSIS) remains the gold standard. The graft is meticulously packed into the decorticated gutters, bridging the L5 transverse processes to the sacral ala bilaterally.
Once the graft is placed and the rods are secured to the pedicle screws—applying compression across the construct if an in-situ fusion is desired—the wound is irrigated copiously with antibiotic-impregnated saline. A subfascial drain is routinely placed to prevent postoperative hematoma formation, which could compress the neural elements. The deep fascial layers are closed in a watertight fashion using heavy, interrupted absorbable sutures, followed by meticulous closure of the subcutaneous tissues and skin.
Complications, Incidence Rates, and Salvage Management
Neurologic and Dural Complications
Despite meticulous surgical technique, posterolateral arthrodesis for spondylolisthesis carries a distinct profile of potential complications. The most feared intraoperative complication is iatrogenic neurologic injury, specifically neuropraxia of the L5 nerve root. This occurs most frequently during attempts to reduce a high-grade slip, where the L5 root is subjected to acute traction over the sacral dome. The incidence of transient L5 neuropraxia can approach 10-15% in reduction cases, presenting postoperatively as a foot drop or extensor hallucis longus (EHL) weakness.
Incidental durotomy is another known risk, particularly when dissecting dense fibrocartilaginous tissue surrounding the pars defect or during a Gill laminectomy. If a dural tear occurs, it must be recognized immediately and repaired primarily using 4-0 or 5-0 non-absorbable sutures, often augmented with a dural sealant and a fascial or fat graft. Unrecognized or inadequately treated dural tears can lead to persistent cerebrospinal fluid (CSF) leaks, pseudomeningoceles, and devastating postoperative meningitis.
| Complication | Estimated Incidence | Prevention & Salvage Management |
|---|---|---|
| L5 Neuropraxia | 2-15% (Higher with reduction) | Prevention: In-situ fusion instead of reduction; continuous intraoperative EMG/MEP monitoring. Management: Often transient; manage with AFO bracing, physical therapy, and high-dose corticosteroids if detected acutely. |
| Pseudarthrosis | 5-15% | Prevention: Meticulous decortication; use of robust autograft (iliac crest); rigid pedicle screw fixation; smoking cessation. Management: Revision surgery with hardware optimization, interbody fusion (TLIF/ALIF), and biologic augmentation (BMP-2). |
| Hardware Failure | 2-5% | Prevention: Accurate screw sizing; bi-cortical S1 purchase; avoiding excessive reduction forces. Management: Revision instrumentation, extending fusion constructs, and addressing underlying pseudarthrosis. |
| Adjacent Segment Disease (ASD) | 10-20% (Long-term) | Prevention: Preservation of the L4-L5 facet capsules during exposure; optimizing sagittal balance. Management: Extension of the fusion construct cephalad to L4 or L3, often requiring decompression of the newly stenotic levels. |
Hardware and Fusion Failures
Pseudarthrosis, or the failure of the bone graft to achieve a solid, continuous fusion mass, remains a significant long-term complication. It is clinically suspected when a patient presents with recurrent back pain months or years after an initial period of relief, and is radiographically confirmed by the presence of haloing around pedicle screws or hardware breakage. The management of symptomatic pseudarthrosis inevitably requires revision surgery.
Hardware failure—including screw pull-out, rod breakage, or screw fracture—is almost always secondary to an underlying pseudarthrosis. The hardware is designed to hold the spine temporarily while the biologic fusion occurs; if the fusion fails, the hardware will eventually succumb to fatigue failure due to repetitive micromotion. Salvage management for these scenarios often involves a combined anterior and posterior approach (e.g., ALIF followed by posterior revision instrumentation) to maximize the surface area for fusion and provide massive biomechanical stability.
Phased Post-Operative Rehabilitation Protocols
Immediate and Early Post-Operative Phase (Weeks 0-6)
The postoperative rehabilitation protocol is as critical to the ultimate success of the procedure as the surgery itself. In the immediate postoperative phase (Days 1-3), the primary goals are pain management, mobilization, and the prevention of deep vein thrombosis (DVT) and pulmonary complications. Patients are typically mobilized out of bed on postoperative day one with the assistance of physical therapy.
Because we utilize rigid pedicle screw instrumentation, the need for rigid postoperative bracing (such as a TLSO with a thigh extension) is largely obsolete in modern practice for low-to-moderate grade slips. However, for high-grade slips or in patients with questionable bone quality, a custom-molded orthosis may be utilized for 6 to 12 weeks to restrict extreme ranges of motion and provide proprioceptive feedback. During the first six weeks, patients are restricted from any bending, lifting (greater than 10 pounds), or twisting (the "BLT" restrictions). Cardiovascular conditioning is limited to progressive walking on flat surfaces.
Intermediate and Advanced Rehabilitation (Months 3-12)
Around the 12-week mark, assuming radiographic evidence of early consolidating fusion mass is present, the rehabilitation protocol advances significantly. Patients are transitioned into a formal, structured physical therapy program focusing on core stabilization, isometric strengthening of the paraspinal musculature, and aggressive lower extremity flexibility, particularly targeting the persistent hamstring tightness that often outlasts the surgical intervention.
Return to full, unrestricted sporting activities is a gradual process that is strictly individualized. For adolescents returning to contact sports or activities involving repetitive hyperextension (such as gymnastics or fast bowling in cricket), a minimum of 6 to 9 months of recovery is mandated, coupled with definitive radiographic proof of a solid posterolateral fusion mass on dynamic radiographs or CT scan. Premature return to high-impact activities risks
