Skeletal Langerhans Cell Histiocytosis: Orthopedic Diagnosis, Biomechanics & Management
Key Takeaway
Skeletal Langerhans Cell Histiocytosis (LCH) involves osteolytic bone lesions causing structural compromise. Orthopedic implications include pathological fracture risk, spinal instability, and neurological deficits. Management often requires diagnostic biopsy and intervention for fractures, instability, or disabling pain. A multidisciplinary approach is crucial for optimal outcomes.
A 4-year-old child presents with a painful limp and a lytic lesion in the proximal femoral metaphysis. Radiographs show a geographic lytic lesion without a sclerotic rim. What is your differential diagnosis, and how would you proceed with the initial work-up?
Candidate: The differential includes Langerhans Cell Histiocytosis (LCH), unicameral bone cyst, osteomyelitis, and Ewing sarcoma. I would perform a biopsy to confirm, then look for other lesions with a skeletal survey.
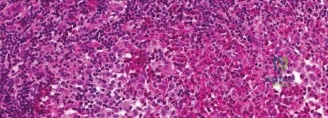
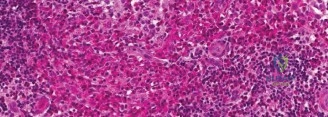
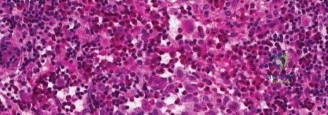
Candidates often jump straight to biopsy without mentioning the systemic nature of LCH. They fail to mention the need for multidisciplinary staging (e.g., bone scan/PET-CT) or the importance of avoiding biopsy if it is a suspected simple cyst, nor do they address the "coffee-bean" nuclei or specific markers (CD1a, CD207) expected on histopathology.
I would structure the differential by age-appropriate pathology: LCH, Unicameral Bone Cyst, Osteomyelitis, and primary bone sarcoma (Ewing's). Work-up starts with MRI to assess cortical integrity and surrounding soft tissue. I would perform a staged diagnostic approach: (1) Systemic staging with a skeletal survey or PET-CT, (2) Core needle biopsy—ensuring the tract is placed for future potential definitive excision, and (3) Multidisciplinary review. I would specifically look for the BRAF V600E mutation and confirm the diagnosis with CD1a and CD207 immunohistochemistry.
You are presented with this imaging of a thoracic spine in a child. The patient has no neurological deficit. How do you manage this?
Candidate: This is a vertebra plana, likely due to LCH. I would consider surgery to stabilize the spine to prevent further collapse and kyphosis.
The candidate shows a lack of knowledge regarding the natural history of pediatric LCH. They are too aggressive, suggesting surgical stabilization for a condition known for remarkable spontaneous reconstitution of height in children.
This is a classic 'vertebra plana'. In children with LCH, the natural history is highly favorable for spontaneous height reconstitution of the vertebral body over time. Surgical intervention is strictly reserved for progressive neurological deficit or severe, uncontrollable pain/instability. My management would involve non-operative observation with serial radiographs, potentially a TLSO brace for comfort, and monitoring for progressive kyphosis. I would reserve instrumentation only if the patient fails to show stability or develops neurological compromise.
A child presents with a large lytic lesion of the proximal femur. You are concerned about an impending pathological fracture. What are the biomechanical criteria for prophylactic fixation, and how do you decide between a nail and a plate?
Candidate: If the lesion is more than 50% of the cortical diameter or over 2.5cm, I fix it. I would use a nail for the femur to handle the stress.
The candidate ignores the physeal status. Using a rigid intramedullary nail in a young child can cause iatrogenic growth arrest. They also fail to mention the importance of intralesional curettage and the potential role of systemic targeted therapy in reducing the lesion size prior to fixating.
Indications for fixation include Mirels score >8, >50% cortical destruction, or >2.5cm axial diameter. The choice depends on physeal status: In skeletally mature patients, a load-sharing intramedullary nail is superior for diaphyseal lesions. In skeletally immature patients, we must prioritize physeal preservation; therefore, a load-bearing locking plate construct that avoids the physis is preferred. One must also consider if systemic BRAF-inhibitor therapy could shrink the lesion sufficiently to avoid high-risk surgery altogether.
