Sacral Chordoma: An Advanced Orthopedic Case Study on Diagnosis & Imaging
Key Takeaway
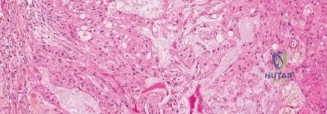
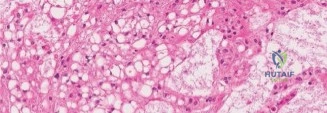
Sacral chordoma diagnosis integrates patient history (sacral pain, radiculopathy, bladder/bowel changes), detailed neurological examination revealing deficits, and advanced imaging (lytic lesion on CT, hyperintense "soap bubble" on T2 MRI). Definitive diagnosis relies on CT-guided biopsy confirming pathognomonic physaliferous cells, guiding precise surgical planning and management.
A 58-year-old male presents with 18 months of progressive gluteal pain, radicular symptoms in the posterior thighs, and new-onset constipation. Clinical exam reveals a firm, non-mobile, rubbery presacral mass on digital rectal examination. How do you approach the initial investigation and biopsy planning for this suspected pathology?
Candidate: I would order plain radiographs of the sacrum, followed by a pelvic MRI as the gold standard for soft tissue evaluation. If a mass is confirmed, I would organize a CT-guided core needle biopsy using a posterior approach, avoiding any transrectal or transvaginal routes to prevent contamination of the presacral space.
Candidates often fail to explicitly state the need for a CT-guided biopsy via a posterior midline approach. Failing to highlight the risk of transrectal biopsy—which is a "game-over" mistake that contaminates the surgical plane and violates the oncological integrity—is a critical failure.
The perfect answer emphasizes: 1) MRI as the modality of choice for characterizing the tumor-nerve relationship, 2) The absolute contraindication of transrectal/transvaginal biopsy, 3) The planning of the biopsy tract to be within the midline, ensuring it is incorporated into the definitive en bloc resection specimen (the "biopsy tract excision" principle).
The imaging (as shown below) confirms a large sacral mass. What are the key radiographic features, and what is your primary differential diagnosis?

Candidate: Radiographically, this is a lytic, expansile, midline lesion. My differential includes chordoma (most likely given the location and age), giant cell tumor, and chondrosarcoma. Metastatic disease and myeloma should also be considered in a 58-year-old patient.
Providing a laundry list of tumors without stratifying them by patient age or anatomical location. Failing to mention chordoma as the top differential for a midline sacral lesion in this age group.
A high-scoring answer links the findings: "The midline location and expansile lytic nature are classic for Chordoma. I would distinguish this from a Giant Cell Tumor, which is more common in younger patients and might appear 'soap-bubbly,' and Chondrosarcoma, which often shows 'rings and arcs' calcification. MRI features like T2 hyperintensity and internal septations further support the chordoma diagnosis."
You have decided on surgery. Explain the oncological rationale for an en bloc resection versus intralesional curettage for this sacral chordoma.
Candidate: Chordomas are radio- and chemo-resistant. An en bloc resection with wide margins is the standard of care. Intralesional curettage has an unacceptable recurrence rate near 100% and significantly worsens prognosis.
Failing to emphasize that chordoma recurrence after piecemeal surgery is almost universal. Also, failing to mention that wide margins are required because the tumor is essentially radio-resistant, meaning surgery is the only path to a potential cure.
The candidate should articulate that "the goal is an R0, wide-margin resection. Chordomas are gelatinous and have a high propensity for seeding. Any intralesional intervention, such as piecemeal resection, violates the pseudocapsule, leading to local recurrence. The surgical plan must include the sacrum, the presacral soft tissue mass, and the biopsy tract as a single, intact unit."
Looking at the preoperative MRI and surgical planning, describe your approach to spinopelvic stability after a high sacrectomy (S1-S2 level).
Candidate: Because the sacroiliac joint is partially or fully compromised in a high sacrectomy, we create spinopelvic dissociation. I would use a lumbopelvic fixation construct, using L4-L5 pedicle screws connected to bilateral iliac screws to restore stability.
Forgetting to mention the specific need for iliac fixation. Pedicle screws alone at the lumbar level are insufficient to stabilize the pelvic ring after sacral resection; you must bridge the gap into the ilium.
The candidate discusses the biomechanical demand of "spinopelvic dissociation." They should specify using a multi-point fixation construct (L4/L5 pedicle screws to iliac screws), the necessity of dual rods for torsional rigidity, and the use of structural allograft to facilitate long-term arthrodesis across the resection site.
