Orthopedic Pathology Review | Dr Hutaif Basic Science R -...
Key Takeaway
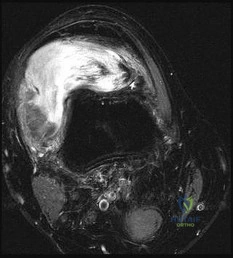
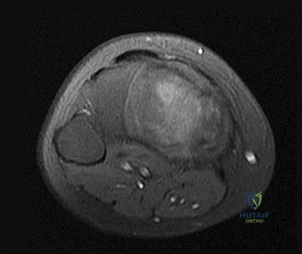
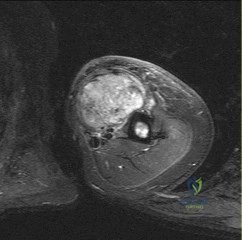
Discover the latest medical recommendations for ORTHOPEDIC MCQS ONLINE PATHOLOGY 017. Dedifferentiated liposarcoma is diagnosed via imaging and biopsy, often involving figures like those encountered in a pubmed question of figures. High-grade sarcomas require wide surgical resection. Radiation therapy reduces local recurrence, while chemotherapy remains investigational. This management contrasts with marginal resection for benign conditions like atypical lipomatous tumors, highlighting distinct treatment pathways based on pathology.
Orthopedic Pathology Review | Dr Hutaif Basic Science R -...
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 14-year-old boy presents with progressive pain in the diaphysis of the femur. Radiographs show a permeative, destructive lesion with a wide zone of transition and an 'onion-skin' periosteal reaction. Biopsy reveals uniform sheets of small round blue cells. Immunohistochemistry is strongly positive for CD99 in a membranous pattern.
Which of the following chromosomal translocations is most characteristic of this patient's diagnosis?

Explanation
Question 2
A 32-year-old female presents with knee pain. Radiographs demonstrate an eccentric, entirely lytic lesion located in the epiphysis of the proximal tibia, extending to the subchondral bone plate. Biopsy reveals a proliferation of uniform mononuclear cells interspersed with numerous osteoclast-like giant cells. What genetic mutation is most commonly associated with the pathogenesis of this tumor?
Explanation
Question 3
A 16-year-old girl presents with swelling in her distal femur. MRI reveals an expansile, multiloculated cystic lesion with prominent fluid-fluid levels. Core needle biopsy confirms multiple blood-filled spaces lacking an endothelial lining, surrounded by fibrous septa containing giant cells and woven bone.
Which of the following genetic alterations is the primary driver of this lesion?
Explanation
Question 4
A 28-year-old male presents with a slow-growing, painful mass near his knee joint, though imaging confirms the lesion is extra-articular. Biopsy demonstrates a biphasic pattern consisting of sheets of uniform spindle cells and scattered glandular structures lined by cuboidal epithelial cells. Which of the following represents the characteristic genetic translocation for this soft tissue sarcoma?
Explanation
Question 5
A 15-year-old boy is diagnosed with conventional high-grade osteosarcoma of the distal femur. Biopsy displays an overtly malignant stroma with high pleomorphism.
Regardless of whether the subtype is osteoblastic, chondroblastic, or fibroblastic, what is the absolute requisite histological hallmark required to establish this diagnosis?
Explanation
Question 6
A 55-year-old man presents with a painful mass in the proximal humerus. Radiographs show a lytic lesion with intralesional stippled and 'popcorn' calcifications. Biopsy demonstrates a cartilaginous matrix with moderate cellularity, atypical chondrocytes, binucleation, and permeation into surrounding marrow spaces. Which of the following genetic mutations is frequently observed in this neoplasm?
Explanation
Question 7
A 65-year-old man presents with severe lower back pain. Radiographs reveal multiple punched-out lytic lesions in the vertebral bodies and skull. A technetium-99m bone scan is surprisingly normal (cold) in these affected areas.
Biopsy of a vertebral lesion would most likely reveal which of the following?

Explanation
Question 8
A 12-year-old girl is evaluated for a limp and a leg length discrepancy. Radiographs demonstrate a well-defined 'ground-glass' appearance in the metaphysis and diaphysis of the proximal femur, accompanied by a shepherd's crook deformity. What is the underlying pathogenesis of this condition?
Explanation
Question 9
A 50-year-old man presents with chronic, insidious sacral pain and recent onset of bowel/bladder dysfunction. MRI reveals a large, destructive midline mass in the sacrum. Biopsy reveals lobules of large cells with prominent intracytoplasmic vacuoles (physaliferous cells) set within a rich myxoid stroma.
Which immunohistochemical marker is highly specific for this tumor?
Explanation
Question 10
A 25-year-old female presents with a deep-seated, slowly enlarging mass in the plantar aspect of her foot, which appears attached to the plantar aponeurosis. Biopsy reveals nests of clear and pale cells with prominent nucleoli. Immunohistochemistry is strongly positive for HMB-45, Melan-A, and S100. Which of the following translocations is diagnostic of this entity?
Explanation
Question 11
A 5-year-old boy presents with a painful lytic lesion in his parietal skull. Biopsy reveals a proliferation of mononuclear cells exhibiting folded, grooved nuclei (resembling coffee beans), admixed with a dense infiltrate of eosinophils. Electron microscopy of the lesional cells demonstrates intracytoplasmic 'tennis-racket' shaped Birbeck granules. These cells will characteristically express which of the following markers?
Explanation
Question 12
A 16-year-old boy presents with knee pain. Radiographs demonstrate a 2 cm lytic lesion with a thin sclerotic rim confined entirely to the epiphysis of the proximal tibia. Biopsy shows mononuclear cells, scattered osteoclast-like giant cells, and distinctive areas of 'chicken-wire' intercellular calcification. What is the underlying genetic mutation most commonly associated with this tumor?
Explanation
Question 13
A 35-year-old man presents with chronic dull pain and swelling in the anterior mid-shaft of his leg. Radiographs reveal a multilocular, expansile, eccentric osteolytic lesion with a 'soap-bubble' appearance. Biopsy demonstrates a biphasic tumor with nests and cords of epithelial cells surrounded by a bland fibrous stroma.
This specific tumor occurs almost exclusively in which of the following bones?

Explanation
Question 14
A 22-year-old male presents with dull, aching pain in his mid-back that does not completely resolve with NSAIDs. Imaging reveals a 2.8 cm radiolucent lesion in the posterior elements of the L3 vertebra with an surrounding zone of reactive sclerosis. Histological evaluation shows a nidus of irregular, interconnected woven bone trabeculae lined by prominent osteoblasts, highly vascular loose connective tissue, and no atypical cells. Based on clinical and pathologic features, what is the most likely diagnosis?
Explanation
Question 15
An asymptomatic 10-year-old boy undergoes a radiograph after a minor knee sprain. The plain film reveals an incidental finding: an eccentric, cortically based, multilocular radiolucency with a well-defined sclerotic border in the distal femur metaphysis.
Which of the following is the most appropriate management for this lesion?

Explanation
Question 16
A 65-year-old male presents with a large, deep intramuscular mass in his proximal thigh. Biopsy reveals two distinct components: one area shows well-differentiated liposarcoma (atypical lipomatous tumor) with lipoblasts, and abruptly transitioning adjacent areas show a high-grade, non-lipogenic pleomorphic sarcoma. Which of the following genetic alterations is the hallmark of this condition?
Explanation
Question 17
A 35-year-old female presents with chronic knee swelling, stiffness, and recurrent hemarthrosis without any history of trauma. MRI displays a nodular and frond-like synovial mass with extensive 'blooming' artifact on gradient-echo sequences due to hemosiderin deposition.
Which genetic alteration is primarily implicated in the pathogenesis of this disease?
Explanation
Question 18
A 40-year-old man presents with a painless, deep, intramuscular mass in the thigh. Biopsy shows a proliferation of small, uniform, round-to-oval cells set in an abundant myxoid stroma, accompanied by a prominent delicate arborizing 'chicken-wire' capillary network and scattered signet-ring lipoblasts. What is the characteristic translocation associated with this tumor?
Explanation
Question 19
A 15-year-old boy presents with a rapidly growing, deep soft tissue mass in his forearm. Biopsy reveals a dense proliferation of primitive small round blue cells. The cells are divided into discrete nests by fibrous septa, with central discohesion of cells creating spaces that mimic pulmonary alveoli. Which genetic fusion is most characteristic of this aggressive sarcoma?
Explanation
Question 20
A 30-year-old female presents with a painless, slow-growing mass on the posterior aspect of the distal femur. Radiographs reveal a dense, heavily ossified mass broadly attached to the posterior cortex. Notably, a thin radiolucent line ('string sign') separates a portion of the tumor from the underlying cortex.
Histologically, the lesion consists of low-grade spindle cells interspersed among parallel trabeculae of woven and lamellar bone. Which genetic abnormality is characteristic of this tumor?

Explanation
Question 21
A 35-year-old male presents with a painless, slowly enlarging swelling over his right shin. Radiographs reveal an eccentric, multi-loculated osteolytic lesion in the anterior cortex of the tibial diaphysis. Biopsy demonstrates a biphasic tumor with nests of epithelial cells surrounded by a bland fibrous stroma. Which of the following immunohistochemical markers is most characteristically positive in the neoplastic cellular nests of this lesion?
Explanation
Question 22
A 42-year-old male presents with persistent shoulder pain. Radiographs show a lytic lesion in the proximal humeral epiphysis. Histological examination reveals sheets of neoplastic cells with abundant clear cytoplasm, distinct cell membranes, scattered osteoclast-like multinucleated giant cells, and areas of chondroid matrix. What is the most likely diagnosis?
Explanation
Question 23
An 8-year-old boy presents with polyuria and a solitary lytic skull lesion. Biopsy of the lesion shows sheets of large, pale mononuclear cells with grooved (coffee-bean) nuclei, mixed with eosinophils. Electron microscopy reveals Birbeck granules. Which of the following immunohistochemical profiles best characterizes the lesional cells?
Explanation
Question 24
A 25-year-old male presents with a slow-growing soft tissue mass in the plantar aspect of his foot. Radiographs show a soft tissue density with focal stippled calcifications. Biopsy reveals a biphasic tumor consisting of spindle cells and glandular epithelial structures. Which of the following translocations is diagnostic for this tumor?
Explanation
Question 25
A 30-year-old female presents with recurrent, painful swelling of her knee. Joint aspiration yields brownish fluid. MRI reveals a thickened synovium with prominent blooming artifact on gradient-echo sequences. The pathogenesis of this condition is primarily driven by a t(1;2) translocation leading to the overexpression of which of the following?
Explanation
Question 26
A 62-year-old male presents with chronic constipation and lower back pain. Imaging reveals a large, destructive, midline mass in the sacrum. Biopsy demonstrates lobules of large cells with prominent intracytoplasmic vacuoles (physaliferous cells) in a myxoid background. Which immunohistochemical marker is highly sensitive and specific for distinguishing this tumor from chondrosarcoma?
Explanation
Question 27
A 32-year-old male presents with a slowly enlarging, ulcerated nodule on the volar aspect of his wrist. Initial biopsy was misinterpreted as a necrotizing granuloma. Re-evaluation reveals a proliferation of plump epithelioid cells surrounding central areas of necrosis. Immunohistochemistry shows loss of nuclear expression of INI1 (SMARCB1). What is the diagnosis?
Explanation
Question 28
A 28-year-old male has an expansile, multiloculated radiolucent lesion in the body of the mandible. Histology shows interlacing fascicles of uniform, bland spindle cells with abundant collagen production and no cytologic atypia or mitotic figures. The lesion is locally aggressive. Mutations in which of the following signaling pathways are most commonly implicated in this tumor?
Explanation
Question 29
A 72-year-old male with a long history of bone pain, increasing head size, and progressive hearing loss suddenly develops severe pain and swelling in his right thigh. Radiographs reveal a highly destructive diaphyseal lesion with cortical breakthrough and a wide zone of transition. His alkaline phosphatase is markedly elevated. The underlying disease process that predisposed him to this malignancy primarily begins with the dysfunction of which cell type?
Explanation
Question 30
A 16-year-old boy presents with mild, chronic knee pain. Radiographs demonstrate an eccentric, sharply circumscribed, well-demarcated osteolytic lesion with a sclerotic margin in the metaphysis of the proximal tibia. Histology shows a lobulated architecture with hypocellular centers containing stellate/spindle cells in a myxoid stroma, and hypercellular peripheries containing multinucleated osteoclast-like giant cells. What is the diagnosis?
Explanation
Question 31
A 15-year-old male undergoes curettage of a 3 cm lytic lesion located exclusively in the greater tuberosity epiphysis of the proximal humerus. Histological analysis reveals sheets of mononuclear cells with characteristic nuclear grooves, prominent eosinophilic cytoplasm, and focal areas of fine, intercellular pericellular calcifications. Molecular testing of this lesion is most likely to reveal a mutation in which of the following genes?
Explanation
Question 32
A 34-year-old female presents with an expansile, eccentric lytic lesion in the distal radius that extends to the subchondral bone plate. A biopsy confirms Giant Cell Tumor (GCT) of bone. Regarding the cellular constituents of this tumor, which of the following statements is most accurate regarding its pathogenesis and targeted medical treatment?
Explanation
Question 33
A 55-year-old male is referred for an asymptomatic calcified lesion discovered incidentally on a radiograph of his proximal humerus. The radiologist suggests distinguishing between an enchondroma and a low-grade (Grade 1) central chondrosarcoma. Which of the following MRI or radiographic findings is the most reliable indicator favoring a diagnosis of low-grade chondrosarcoma over enchondroma?
Explanation
Question 34
A 48-year-old female presents with generalized weakness, recurrent nephrolithiasis, and bilateral multi-focal lytic bone lesions. A biopsy of a femoral lesion demonstrates a highly vascularized stroma containing plump spindle cells, areas of hemorrhage, and clusters of osteoclast-like multinucleated giant cells. Which of the following laboratory profiles is most likely to be found in this patient?
Explanation
Question 35
A 22-year-old female presents with a slow-growing, painless mass deep in the vastus lateralis. Staging reveals multiple small brain metastases. Biopsy of the primary tumor shows large, polygonal cells with abundant granular eosinophilic cytoplasm arranged in a nested, pseudoalveolar pattern. PAS staining reveals diastase-resistant rhomboid crystals in the cytoplasm. What is the specific genetic alteration driving this tumor?
Explanation
Question 36
A 52-year-old male undergoes MRI for chronic lumbar radiculopathy. An incidental lesion is noted in the L3 vertebral body. Sagittal T1- and T2-weighted MRI both show high signal intensity in the lesion, and axial CT shows a "polka-dot" pattern of thickened trabeculae. What is the most appropriate management for this specific lesion?
Explanation
Question 37
A 6-year-old boy presents with painless anterolateral bowing of his left tibia. Radiographs show multiple anterior intracortical lytic lesions in the tibial diaphysis. Histology shows a fibroblastic stroma surrounding trabeculae of woven bone that are lined by a prominent layer of active osteoblasts. No epithelial cells are identified on extensive sectioning. This lesion has a known clinical association with, and must be carefully distinguished from, which of the following malignancies?
Explanation
Question 38
A 68-year-old male with a history of fatigue and normocytic anemia presents with severe, acute onset back pain. Radiographs reveal multiple 'punched-out' lytic lesions in his skull and a compression fracture of T10. Serum protein electrophoresis (SPEP) demonstrates an M-spike. If a biopsy of the skull lesion were performed, what would be the most prominent immunohistochemical finding?
Explanation
Question 39
A 32-year-old female presents with a slowly enlarging, hard mass on the posterior aspect of her distal femur. Plain radiographs display a heavily ossified, dense, lobulated mass arising from the cortex, with a radiolucent line (cleft) separating parts of the tumor from the underlying bone cortex. Histological examination shows bland, well-differentiated spindle cells arranged between parallel trabeculae of mature woven and lamellar bone. Molecular analysis is most likely to show amplification of which genomic region?
Explanation
Question 40
An 18-year-old female presents with a deep thigh mass. Biopsy reveals a primitive, small round cell tumor. Molecular analysis demonstrates a t(11;22)(q24;q12) translocation resulting in an EWSR1-FLI1 fusion transcript. Although this tumor typically arises in bone, when it presents as a primary soft tissue mass (extraskeletal), it must be differentiated from which morphologically identical tumor that belongs to the same family and shares the identical genetic driver?
Explanation
Question 41
A 15-year-old boy presents with knee pain and swelling. Radiographs reveal a lytic and blastic lesion in the distal femoral metaphysis with a 'sunburst' periosteal reaction. Biopsy demonstrates malignant cells producing osteoid matrix. Which of the following tumor suppressor genes are most frequently inactivated in the pathogenesis of this primary bone tumor?
Explanation
Question 42
A 55-year-old man presents with chronic, progressively worsening thigh pain. Radiographs demonstrate a large radiolucent lesion with 'popcorn' calcifications in the proximal femur and prominent endosteal scalloping. Histological evaluation shows lobules of hyaline cartilage with atypical, binucleated cells within lacunae. What is the most important histologic predictor of prognosis and metastasis for this patient's lesion?
Explanation
Question 43
A 30-year-old woman presents with a slow-growing, painful mass around her ankle. Imaging reveals an extra-articular soft-tissue mass with stippled calcifications. Biopsy demonstrates a biphasic pattern consisting of both epithelial and spindle cells. Cytogenetic testing of the lesion is most likely to reveal which of the following translocations?
Explanation
Question 44
A 60-year-old man presents with bowel and bladder dysfunction and sacral pain. MRI shows a destructive, lobulated mass centered in the sacrum. Histopathology shows lobules of myxoid tissue containing large cells with vacuolated cytoplasm (physaliferous cells). Immunohistochemistry for this tumor will characteristically be positive for cytokeratin, EMA, S-100, and which of the following highly specific markers?
Explanation
Question 45
A 24-year-old man presents with a nodular lesion on the volar aspect of his finger that has slowly ulcerated, mimicking a chronic infection or granuloma. Biopsy reveals epithelioid and spindle cells arranged in a nodular pattern with central necrosis. Immunohistochemistry demonstrates a loss of SMARCB1 (INI1) expression. What is the most likely diagnosis?
Explanation
Question 46
A 28-year-old female presents with a palpable, painless mass on the posterior aspect of her distal thigh. Radiographs demonstrate a dense, lobulated, ossified mass attached to the posterior cortex of the distal femur with a 'string sign' (radiolucent cleft). Biopsy confirms a low-grade spindle cell stroma interspersed with well-formed woven bone trabeculae. Which genetic alteration is characteristic of this tumor?
Explanation
Question 47
A 15-year-old boy presents with shoulder pain. Radiographs reveal a well-circumscribed, lytic lesion in the epiphysis of the proximal humerus with a thin sclerotic margin. Histological examination shows mononuclear cells with grooved nuclei and areas of 'chicken-wire' calcification. Which specific genetic mutation drives this neoplasm?
Explanation
Question 48
A 12-year-old girl is evaluated for a pathological fracture of the proximal femur. Radiographs reveal a large, diaphyseal expansile lesion with a 'ground-glass' matrix and a 'shepherd's crook' deformity. A biopsy shows irregular, C-shaped trabeculae of woven bone lacking prominent osteoblastic rimming in a fibrous stroma. What is the underlying molecular mechanism of this disorder?
Explanation
Question 49
A 45-year-old man undergoes excision of a large, deep soft-tissue mass in his thigh. Pathology reveals a uniform proliferation of primitive mesenchymal cells, small signet-ring lipoblasts, and a prominent plexiform ('chicken-wire') capillary network within a myxoid stroma. Which cytogenetic abnormality is pathognomonic for this tumor?
Explanation
Question 50
A 32-year-old man presents with chronic anterior tibial pain. Radiographs show a multiloculated, eccentric, osteolytic lesion in the anterior diaphysis of the tibia. Histopathology demonstrates a biphasic tumor with nests of basaloid epithelial cells surrounded by an osteofibrous stroma. Immunohistochemistry is positive for broad-spectrum cytokeratins. What is the most likely diagnosis?
Explanation
Question 51
A 5-year-old boy presents with anterior bowing of the tibia. Imaging shows a radiolucent, intracortical lesion along the anterior tibial diaphysis. Biopsy reveals fibroblastic tissue with trabeculae of woven bone that are characteristically rimmed by active, plump osteoblasts. Cytokeratin staining is negative. Patients with this condition require clinical follow-up primarily to monitor for progression into which of the following entities?
Explanation
Question 52
A 40-year-old man presents with hip pain. Radiographs reveal a well-defined lytic lesion in the epiphysis of the proximal femur. Biopsy demonstrates sheets of cells with abundant, clear cytoplasm and distinct cell membranes, interspersed with areas of woven bone and chondroid matrix. What is the most appropriate management for this lesion?
Explanation
Question 53
A 12-year-old boy is found to have an incidental eccentric, multiloculated, radiolucent lesion with a sclerotic rim in the distal femoral metaphysis following minor trauma. A biopsy of a similar lesion would characteristically demonstrate spindle cells in a storiform pattern, multinucleated giant cells, and lipid-laden foamy macrophages. Multiple such lesions, combined with café-au-lait spots, are associated with which of the following syndromes?
Explanation
Question 54
A 68-year-old man presents with severe back pain and fatigue. Radiographs show multiple punched-out lytic lesions in his skull and vertebrae. Laboratory studies reveal hypercalcemia and a monoclonal spike on serum protein electrophoresis. A bone marrow biopsy confirms the diagnosis. Which immunohistochemical marker is characteristically strongly positive on the neoplastic cells?
Explanation
Question 55
An 18-year-old male presents with persistent night pain in his thigh that is dramatically relieved by aspirin. Radiographs show a 1 cm radiolucent nidus surrounded by dense reactive cortical sclerosis in the proximal femoral diaphysis. The profound pain experienced by the patient is primarily due to local production of which of the following mediators?
Explanation
Question 56
A 70-year-old man presents with increasing head size, hearing loss, and anterior bowing of the tibiae. Laboratory testing reveals a markedly elevated serum alkaline phosphatase with normal calcium and phosphorus levels. A biopsy of the tibia would most likely show a mosaic pattern of lamellar bone. Mutations in which gene are most strongly implicated in the familial form of this condition?
Explanation
Question 57
A 35-year-old woman presents with chronic knee swelling, pain, and catching. MRI demonstrates a large, nodular intra-articular mass with dark signal intensity on T1 and T2-weighted images due to hemosiderin deposition. A biopsy confirms tenosynovial giant cell tumor (pigmented villonodular synovitis). What is the underlying molecular pathogenesis driving the proliferation of this lesion?
Explanation
Question 58
A 40-year-old male with a history of numerous cutaneous neurofibromas and café-au-lait spots presents with a rapidly enlarging, painful mass in his sciatic nerve. Biopsy reveals a highly cellular, pleomorphic spindle cell tumor with brisk mitotic activity and geographic necrosis. Immunohistochemistry shows patchy, weak S-100 positivity. The malignant transformation in this patient is most closely linked to loss of heterozygosity in which of the following?
Explanation
Question 59
A 4-year-old boy presents with a painful, lytic lesion in the skull vault. Biopsy demonstrates a proliferation of mononuclear histiocyte-like cells with grooved, 'coffee-bean' nuclei, admixed with eosinophils. Electron microscopy identifies characteristic tennis-racket-shaped cytoplasmic organelles. Recent targeted therapies for this disease successfully inhibit which of the following commonly mutated kinases?
Explanation
Question 60
A 6-year-old girl presents with a rapidly expanding soft tissue mass in her forearm. Biopsy reveals sheets of primitive small round blue cells with prominent fibrovascular septa lacking central cellularity, creating an 'alveolar' pattern. Strong desmin and myogenin positivity is noted. Which specific chromosomal translocation is most frequently identified in this malignancy?
Explanation
Question 61
A 28-year-old male presents with a slowly enlarging, painless mass around his ankle. MRI shows a soft tissue mass adjacent to the Achilles tendon. Core biopsy reveals a biphasic tumor with both epithelial-like glandular structures and uniform spindle cells. Which of the following cytogenetic abnormalities is pathognomonic for this tumor?
Explanation
Question 62
A 65-year-old man presents with dull pelvic pain. Radiographs reveal a bulky, destructive lesion in the ilium with 'ring-and-arc' calcifications. Biopsy demonstrates atypical chondrocytes with binucleation and permeation of the host trabecular bone. Mutations in which of the following genes are most frequently implicated in the pathogenesis of this primary bone tumor?
Explanation
Question 63
A 12-year-old girl is evaluated for a leg length discrepancy and a 'shepherd's crook' deformity of her proximal femur. Radiographs show an expansile, ground-glass intramedullary lesion. Histological analysis demonstrates irregular trabeculae of woven bone lacking prominent osteoblastic rimming, set in a fibrous stroma. This condition is driven by an activating mutation in a gene encoding which of the following?
Explanation
Question 64
A 55-year-old woman complains of chronic sacral pain and bowel dysfunction. MRI shows a midline, destructive sacral mass. Biopsy reveals lobules of large, vacuolated cells with bubbly cytoplasm arranged in a myxoid stroma. Immunohistochemistry is positive for S100, cytokeratin, and a highly specific nuclear transcription factor. What is this specific immunohistochemical marker?
Explanation
Question 65
A 6-year-old boy presents with back pain. Radiographs demonstrate vertebra plana of T8. A biopsy of the vertebral body shows a proliferation of mononuclear cells with folded, 'coffee-bean' nuclei, admixed with numerous eosinophils. These neoplastic cells are most likely to harbor a mutation in which of the following?
Explanation
Question 66
A 30-year-old male presents with chronic anterior knee pain and intermittent swelling. MRI reveals a nodular intra-articular mass with low signal intensity on both T1 and T2 weighted sequences, along with blooming artifact on gradient-echo imaging. Histology shows mononuclear cells, multinucleated giant cells, and hemosiderin-laden macrophages. Which of the following drives the pathogenesis of this lesion?
Explanation
Question 67
A 35-year-old male presents with an anterior shin mass. Radiographs show a multiloculated, expansile, eccentric radiolucency in the anterior cortex of the tibial diaphysis. Histology exhibits a biphasic pattern of uniform epithelial cells forming nests and tubules within a bland spindle-cell fibrous stroma. Which immunohistochemical stain will best differentiate the prominent cell nests in this tumor from surrounding osteofibrous tissue?
Explanation
Question 68
A 68-year-old woman presents with severe back pain. Radiographs reveal multiple 'punched-out' lytic lesions in her skull and spine. Bone marrow biopsy shows sheets of eccentric cells with abundant basophilic cytoplasm, a perinuclear halo (hof), and clock-face chromatin. Which cytokine is primarily responsible for the osteoclast activation and subsequent lytic bone destruction in this disease?
Explanation
Question 69
A 25-year-old woman presents with a deep, firm mass in her plantar fascia. Excisional biopsy reveals nests of pale, uniform cells separated by delicate fibrous septa. Immunohistochemistry is strongly positive for S100, HMB-45, and Melan-A. Cytogenetics reveals a t(12;22)(q13;q12) translocation. What is the diagnosis?
Explanation
Question 70
A 22-year-old male presents with a slowly growing, ulcerating nodule on his volar wrist. It was initially excised at an outside clinic under the assumption it was a necrotizing granuloma, but it rapidly recurred. Histology shows epithelioid cells arranged in nodules with central necrosis. Which immunohistochemical finding is a diagnostic hallmark of this malignancy?
Explanation
Question 71
A 35-year-old female presents with a painless mass on the posterior aspect of her distal femur. Imaging shows a densely ossified mass attached to the cortex with a broad base, showing no medullary involvement. Biopsy reveals well-formed trabeculae of mature woven bone within a bland, low-grade spindle cell stroma. Which genetic alteration is characteristic of this lesion?
Explanation
Question 72
A 16-year-old boy presents with pain in his shoulder. Radiographs show an epiphyseal lytic lesion in the proximal humerus with subtle internal calcifications. Biopsy demonstrates mononuclear cells with longitudinal nuclear grooves and areas of eosinophilic matrix with a 'chicken-wire' pattern of calcification. What genetic mutation is specifically associated with this tumor?
Explanation
Question 73
A 45-year-old man presents with a large, painless mass in his deep thigh musculature. MRI demonstrates a lipomatous tumor with thick, nodular septations. Histologic examination reveals mature adipocytes alongside atypical, hyperchromatic spindle cells. Which molecular finding confirms the diagnosis of Atypical Lipomatous Tumor/Well-Differentiated Liposarcoma?
Explanation
Question 74
A 15-year-old male presents with a rapidly enlarging mass in his forearm. Biopsy reveals a primitive malignant neoplasm with small round blue cells arranged in clusters separated by dense fibrous septa, forming cleft-like spaces. Immunohistochemistry is strongly positive for desmin and myogenin. Which translocation is most likely present?
Explanation
Question 75
A 10-year-old girl is evaluated for multiple bony deformities and multiple dark, compressible soft tissue masses on her hands. Radiographs reveal numerous cartilaginous lesions within the medullary canals of the phalanges, and multiple phleboliths in the adjacent soft tissues. This patient is at a significantly increased risk for which of the following complications?
Explanation
Question 76
A 19-year-old male complains of severe, throbbing pain in his proximal tibia that is worse at night and dramatically relieved by ibuprofen. Imaging shows a cortical lucency measuring 8 mm, surrounded by dense reactive sclerosis. The intense pain associated with this lesion is primarily mediated by which of the following mechanisms?
Explanation
Question 77
A 24-year-old female presents with a destructive, lytic lesion in her distal femur. Biopsy shows an intraosseous proliferation of uniform, bland spindle cells with abundant collagen bundles, resembling a soft-tissue desmoid tumor. There is no cytological atypia or pleomorphism. This lesion is most commonly associated with mutations in which of the following genes?
Explanation
Question 78
A 70-year-old man with advanced prostate cancer develops new, diffuse osteoblastic metastases in his lumbar spine and pelvis. The mechanism of this profound osteoblastic response is primarily mediated by the secretion of which of the following factors by the metastatic tumor cells?
Explanation
Question 79
A 40-year-old male presents with a deep mass in his thigh. Histology reveals a pattern of atypical spindle cells arranged in a 'staghorn' or hemangiopericytoma-like vascular pattern, interspersed with thick bands of collagen. Immunohistochemistry demonstrates strong nuclear expression of STAT6. What is the most likely diagnosis?
Explanation
Question 80
A 68-year-old man presents with progressively increasing hat size, hearing loss, and bowing of his tibiae. Radiographs show thickened cortices and a coarse trabecular pattern. Bone biopsy reveals a mosaic pattern of lamellar bone with prominent cement lines. Which of the following gene mutations is most strongly associated with the familial form of this condition?
Explanation
Question 81
A 25-year-old male presents with a deep, painless mass in his posterior thigh. MRI shows a well-circumscribed soft tissue mass adjacent to the knee joint. Biopsy reveals a biphasic tumor consisting of epithelial cells forming glandular structures and a spindle cell stromal component. Which of the following chromosomal translocations is diagnostic for this malignancy?
Explanation
Question 82
A 14-year-old boy presents with chronic shoulder pain. Radiographs reveal a well-defined, lytic epiphyseal lesion in the proximal humerus with a sclerotic margin. Biopsy shows mononuclear cells with grooved nuclei and areas of "chicken-wire" calcification. Which of the following genetic mutations is most characteristic of this lesion?
Explanation
Question 83
A 40-year-old male undergoes excision of a large thigh mass. Histopathological examination demonstrates a multinodular tumor with a myxoid stroma, scattered lipoblasts, and a prominent "chicken-wire" capillary network. Which translocation drives the pathogenesis of this tumor?
Explanation
Question 84
A 10-year-old girl is evaluated for a limp. Radiographs show a "shepherd's crook" deformity of the proximal femur with a ground-glass appearance. Biopsy reveals curvilinear woven bone trabeculae lacking osteoblastic rimming set in a fibrous stroma. A mutation in which of the following genes is responsible for this condition?
Explanation
Question 85
A 22-year-old male presents with a firm, ulcerating nodule on the volar aspect of his right wrist. Biopsy demonstrates nodular proliferations of epithelioid and spindle cells with central areas of necrosis, mimicking a granuloma. Which of the following immunohistochemical or molecular findings is most specific for this diagnosis?
Explanation
Question 86
A 15-year-old boy presents with progressive distal femur pain. Radiographs show a sclerotic metaphyseal lesion with a "sunburst" periosteal reaction. Biopsy confirms pleomorphic cells producing malignant osteoid. The patient's family history is significant for multiple early-onset cancers. A germline mutation in which gene is most likely present?
Explanation
Question 87
A 60-year-old male presents with progressive constipation and urinary incontinence. Imaging reveals a large, destructive midline mass involving the sacrum. Biopsy demonstrates lobules of vacuolated cells with a bubbly appearance embedded in a myxoid stroma. Which of the following immunohistochemical markers is most specific for this tumor?
Explanation
Question 88
A 30-year-old female presents with a slowly enlarging mass on her plantar foot deep to the plantar fascia. Biopsy shows nests of uniform cells with clear cytoplasm and prominent nucleoli, divided by fibrous septa. Immunohistochemistry is strongly positive for HMB-45 and S-100. Which chromosomal abnormality is diagnostic?
Explanation
Question 89
A 35-year-old male presents with a dull ache in his lower leg. Radiographs show a well-circumscribed, multilobular, osteolytic lesion in the anterior diaphysis of the tibia. Biopsy reveals a biphasic pattern consisting of nests of basaloid cells surrounded by a bland fibrous stroma. Which of the following markers will the epithelial-like cells express?
Explanation
Question 90
A 28-year-old female presents with a painless mass in her abdominal wall. Excision is performed, and pathology shows a proliferation of uniform spindle cells in a collagenous stroma with deep infiltration into adjacent skeletal muscle. Immunohistochemistry shows nuclear beta-catenin accumulation. Patients with multiple such tumors should be screened for which of the following syndromes?
Explanation
Question 91
A 18-year-old male presents with severe, progressive thigh pain that awakens him at night but is dramatically relieved by ibuprofen.
Imaging reveals a thick area of cortical sclerosis containing a 7-millimeter central radiolucent nidus. The intense pain experienced by this patient is primarily mediated by excessive local production of which substance?
Explanation
Question 92
An 8-year-old boy presents with back pain. Radiographs demonstrate vertebra plana of T8. Biopsy reveals a proliferation of mononuclear cells with indented, "coffee-bean" shaped nuclei mixed with eosinophils. Electron microscopy identifies tennis-racket shaped Birbeck granules. Which genetic mutation is most frequently identified in this disease?
Explanation
Question 93
A 65-year-old male presents with hypercalcemia, renal insufficiency, anemia, and low back pain. Radiographs of the skull reveal multiple "punched-out" lytic lesions. Bone marrow biopsy demonstrates sheets of cells with an eccentric nucleus, clumped "clock-face" chromatin, and a perinuclear halo. These neoplastic cells will strongly express which of the following surface markers?
Explanation
Question 94
A 55-year-old male presents with deep groin pain. Radiographs of the proximal femur show a poorly marginated radiolucent lesion with stippled "rings and arcs" calcifications and endosteal scalloping. Biopsy demonstrates malignant cartilage permeating between preexisting host bone trabeculae. Which of the following gene mutations is most commonly implicated in this primary bone tumor?
Explanation
Question 95
A 12-year-old boy is evaluated for multiple painless, bony bumps around his knees and shoulders. Radiographs show multiple pedunculated excrescences pointing away from the joint line. Genetic testing reveals a loss-of-function mutation in EXT1. The normal product of this gene is essential for which of the following cellular processes?
Explanation
Question 96
A 14-year-old girl presents with a rapidly enlarging mass deep in her calf. Biopsy reveals a proliferation of small round blue cells with eosinophilic cytoplasm, separated by fibrous septa into spaces resembling pulmonary alveoli. Which translocation is diagnostic and confers an unfavorable prognosis in this sarcoma?
Explanation
Question 97
A 35-year-old male undergoes wide local excision of a slow-growing, multi-nodular mass on his trunk. Histology reveals bland spindle cells arranged in a "storiform" or cartwheel pattern, deeply infiltrating the subcutaneous fat in a "honeycomb" pattern. The tumor cells are strongly positive for CD34. Which cytogenetic abnormality is characteristic of this lesion?
Explanation
None
