Orthopaedic Oncology Generic: Ace Tumor Staging for Oral Exams
Key Takeaway
Discover the latest medical recommendations for Orthopaedic Oncology Generic: Ace Tumor Staging for Oral Exams. Orthopaedic oncology generic tumor staging primarily uses the Musculoskeletal Tumour Society (Enneking/MSTS) system. This method classifies musculoskeletal sarcomas based on tumor grade (G), local extent (T, intracompartmental or extracompartmental), and presence of distant metastases (M). Stage III is assigned if any metastasis exists, irrespective of grade or local spread, guiding crucial treatment decisions.
A 28-year-old patient presents with a high-grade sarcoma of the mid-humerus. You are planning a core needle biopsy. As an FRCS candidate, demonstrate your understanding of the surgical approach in relation to subsequent limb salvage.
Candidate: I would perform a longitudinal core needle biopsy. I'd ensure the tract is placed so it can be excised entirely during the definitive resection. I would avoid transverse incisions and ensure the biopsy is taken from the most representative, vascular part of the tumor, usually guided by MRI findings, while avoiding contamination of adjacent compartments or the neurovascular bundle.
Failing to mention the "excision of the biopsy tract." Candidates often focus only on the diagnostic aspect and ignore the fact that the skin entry point and the soft tissue track are considered "contaminated." If the definitive surgery doesn't remove this track, the patient faces a significant increase in local recurrence risk. Also, choosing an incorrect approach (e.g., axillary approach for a mid-shaft lesion) that makes definitive reconstruction difficult.
A high-scoring answer is structured as follows: 1. Pre-planning: State that the biopsy must be planned in consultation with the surgeon who will perform the definitive resection. 2. Tract Placement: The biopsy must be longitudinal (never transverse) and placed directly over the tumor so that the entire skin incision and the underlying soft tissue track can be excised en-bloc during the final surgery. 3. Anatomical Consideration: Avoid contamination of neurovascular planes (e.g., radial nerve in the posterior approach) and adjacent uninvolved compartments. 4. Technique: Use a core needle to minimize the volume of contaminated tissue compared to an open biopsy, and ensure haemostasis to prevent tracking of tumor cells via haematoma.
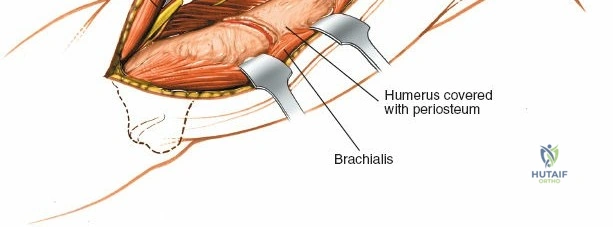
The patient's MRI shows the tumor is deep to the deep fascia, involving the medullary canal but not crossing the elbow or shoulder joint. How do you categorize the Enneking local extent (T-stage), and why is this distinction critical?
Candidate: This would be categorized as T2 (extracompartmental) if it has breached the natural anatomical boundaries or T1 (intracompartmental) if it remains contained. In this case, since it is deep to the deep fascia and contained, it is T1. This is critical because T2 tumors carry a significantly higher risk of local recurrence and often necessitate wider surgical margins or more complex reconstruction.
Ignoring the "compartment" concept. Failing to explicitly define what a compartment is (bone, cartilage, fascial boundaries) and assuming all sarcomas are automatically Stage IIB. Many candidates forget that T1/T2 status is the primary driver of the "A" or "B" suffix in the Enneking staging.
Structure the response by first defining the Enneking MSTS Staging criteria. Explain that T1 (Intracompartmental) tumors are contained within a defined anatomical space (bone, joint, or specific muscle compartment), which provides a natural barrier. T2 (Extracompartmental) tumors have breached these barriers, placing neurovascular structures and adjacent tissues at risk. Conclude by noting that the T-stage dictates the difficulty of achieving a "Wide" surgical margin—the goal for all Stage II (high-grade) sarcomas—and directly influences the local recurrence-free survival rate.
