Orthopedic Case Study: Diagnosing Pigmented Villonodular Synovitis (PVNS) of the Knee
Key Takeaway
PVNS in the knee is diagnosed through a comprehensive approach. Key indicators include chronic knee pain and effusion, specific MRI findings like diffuse synovitis and hemosiderin deposition ('blooming artifact'), serosanguinous synovial fluid, and confirmed by arthroscopic synovial biopsy demonstrating characteristic villous proliferation with hemosiderin-laden macrophages.
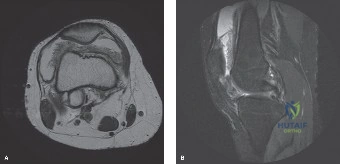
A 38-year-old male presents with 2 years of insidious left knee pain and mechanical symptoms. He has a 'boggy' joint effusion and repeat aspirations yield dark, serosanguinous fluid. MRI is ordered. Based on the provided image, what is your primary diagnosis and the underlying pathophysiological mechanism?
Candidate: The diagnosis is Pigmented Villonodular Synovitis (PVNS), now called diffuse-type Tenosynovial Giant Cell Tumor (TGCT). It's caused by synovial proliferation leading to hemosiderin deposition. The MRI shows blooming artifacts due to this iron content.
Failing to mention the updated WHO classification (TGCT), or omitting the genetic basis (CSF1 overexpression/translocation). Candidates often describe the imaging but fail to discuss the necessity of distinguishing it from other causes of recurrent hemarthrosis, such as hemophilia or synovial chondromatosis.
The diagnosis is Diffuse-type Tenosynovial Giant Cell Tumor (TGCT). Pathophysiologically, it is driven by a t(1;2)(p13;q37) translocation leading to overexpression of Colony Stimulating Factor 1 (CSF1). This recruits non-neoplastic macrophages/giant cells, resulting in the characteristic exuberant synovial proliferation. The MRI findings of 'blooming' on gradient-echo sequences reflect paramagnetic hemosiderin deposition, which distinguishes it from other synovial proliferative disorders.
The patient is booked for an all-arthroscopic synovectomy. How do you justify this approach over an open procedure, and what specific steps are required during the surgery to mitigate the risk of recurrence, which is notably high in this condition?
Candidate: Arthroscopic synovectomy is less morbid with faster rehab. To prevent recurrence, I must perform a complete synovectomy, specifically addressing the posterior compartments using trans-notch portals to clear the gutters and the suprapatellar pouch.
Missing the importance of the posterior compartments. Many candidates treat the anterior disease adequately but fail to describe the technical necessity of dedicated posteromedial and posterolateral portals to clear the recesses, which is the primary site of residual disease leading to recurrence.
Arthroscopic synovectomy is preferred due to reduced arthrofibrosis and superior visualization of the joint compartments. To minimize recurrence, one must ensure a 'total' synovectomy. Key steps include: 1) Meticulous resection in the gutters and suprapatellar pouch using motorized shavers and radiofrequency. 2) Essential visualization and resection of posterior recesses via specialized posteromedial and posterolateral portals—not just trans-notch. 3) Copious lavage to remove microscopic debris. Finally, long-term monitoring with MRI is required, with consideration for adjuvant therapies (e.g., Pexidartinib or synoviorthesis) if the disease is aggressive or recurs.
