Diffuse Tenosynovial Giant Cell Tumor (TGCT) of the Knee: Pathophysiology & Surgical Anatomy
Key Takeaway
Tenosynovial Giant Cell Tumor (TGCT), diffuse type, formerly PVNS, is a rare, locally aggressive proliferative disorder primarily affecting the knee. Characterized by synovial hypertrophy, it leads to cartilage destruction and pain. Its etiology involves a CSF1 gene translocation, overexpressing CSF1, which recruits macrophages driving tumor growth and joint damage.
Introduction and Epidemiology
Pigmented villonodular synovitis (PVNS), now formally classified by the World Health Organization (WHO) as Tenosynovial Giant Cell Tumor (TGCT), diffuse type, represents a complex, benign, yet locally aggressive proliferative disorder originating from the synovium. This pathology predominantly affects large diarthrodial joints, with the knee being the most common site, accounting for approximately 80% of all intra-articular cases. Despite its benign histological nature, the aggressive proliferation of synovial cells and subsequent inflammatory cascade lead to progressive destruction of articular cartilage and subchondral bone, ultimately resulting in debilitating pain, severe functional impairment, and often end-stage osteoarthritis if not effectively managed.
Epidemiologically, TGCT is a rare condition, with an estimated incidence ranging from 1.8 to 4.5 cases per million population per year. It typically presents in individuals between the third and fifth decades of life, exhibiting a slight female predominance. While TGCT is generally monoarticular, polyarticular involvement has been reported in a small percentage of cases, often correlating with a more aggressive disease course and presenting significant management challenges. The precise etiology remains largely undefined, with historical theories suggesting inflammatory, reactive, or traumatic origins.
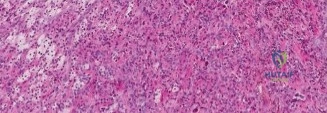
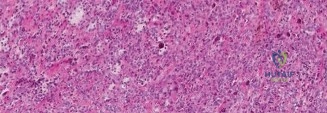
Current molecular understanding, however, strongly points towards a neoplastic clonal proliferation of synovial-like stromal cells. A pivotal discovery has been the identification of a specific chromosomal translocation, t(1;2)(p13;q37), involving the CSF1 gene. This translocation results in the overexpression of Colony Stimulating Factor 1 (CSF1) by a subset of tumor cells. Interestingly, these neoplastic cells comprise only a small minority (approximately 2% to 16%) of the total tumor volume. The secreted CSF1 acts as a potent chemoattractant and growth factor for CSF1 receptor-expressing macrophages, multinucleated giant cells, and other inflammatory cells, which constitute the vast majority of the tumor mass. This "landscape effect"—a self-perpetuating feedback loop between neoplastic stromal cells and reactive polyclonal macrophages—drives the characteristic proliferative, hypervascular, and destructive nature of diffuse TGCT.
Surgical Anatomy and Biomechanics
Effective surgical management of diffuse TGCT in the knee necessitates a profound understanding of the complex knee joint anatomy and the biomechanical implications of synovial proliferation. The knee, a modified hinge joint, is encased by a synovial membrane that invests all intra-articular structures save for the articular cartilage and menisci. In diffuse TGCT, this synovium undergoes widespread villous and nodular hypertrophy, extending into virtually all accessible synovial recesses and often demonstrating extra-articular extension through capsular weak points.
Key anatomical considerations for surgical planning include the intricate division of synovial compartments. The knee joint comprises several distinct synovial recesses: the suprapatellar pouch, medial gutter, lateral gutter, intercondylar notch, and the posterior compartment (inclusive of posteromedial and posterolateral recesses). Diffuse TGCT frequently involves multiple, if not all, of these compartments, rendering complete synovectomy a formidable surgical challenge. The suprapatellar pouch, bounded anteriorly by the quadriceps tendon and posteriorly by the prefemoral fat pad, is a large reservoir that can harbor massive volumes of hypertrophic tissue.
Involvement of the posterior compartment is common, critical, and notoriously difficult to eradicate. Proliferation in this area can directly impinge upon or encase vital neurovascular structures. The posterior capsule forms the anterior boundary of the popliteal fossa. The popliteal artery, popliteal vein, and tibial nerve lie in immediate proximity to the posterior capsule. In some anatomical variants, the popliteal artery rests mere millimeters from the posteromedial joint capsule. Extra-articular extension of TGCT often tracks along the popliteus tendon hiatus or through posterior capsular defects, enveloping these neurovascular bundles. Accessing this region requires advanced arthroscopic techniques, such as the trans-septal portal, or an open posterior arthrotomy, demanding meticulous anatomical dissection and precise tissue removal to avoid catastrophic iatrogenic injury.
Chronic synovial inflammation, exacerbated by the presence of hemosiderin deposits (a byproduct of recurrent microhemorrhages from the friable tumor neovasculature), exerts a direct toxic effect on chondrocytes. This biomechanically compromises the articular cartilage, leading to accelerated wear. Furthermore, the hypertrophic synovial mass can create mechanical blocks to terminal extension or flexion, altering normal knee kinematics and increasing focal contact pressures, which further accelerates joint degeneration.
Indications and Contraindications
The management of diffuse TGCT is highly individualized, dictated by the extent of disease, the degree of joint destruction, and the patient's functional demands. Surgical synovectomy remains the cornerstone of treatment, aiming to eradicate the macroscopic tumor burden, alleviate mechanical symptoms, and halt progressive joint destruction. However, the high recurrence rate associated with diffuse TGCT necessitates a careful evaluation of operative versus non-operative, or combined multimodal, approaches.
| Clinical Scenario | Operative Indications | Non Operative Indications |
|---|---|---|
| Primary Diffuse TGCT | Symptomatic presentation with mechanical blocks, pain, or recurrent effusions; impending cartilage destruction. | Truly asymptomatic incidental findings (exceedingly rare in diffuse type); severe medical comorbidities precluding anesthesia. |
| Extra Articular Extension | Localized extension amenable to complete en bloc resection via combined arthroscopic/open approaches. | Massive extra-articular involvement encasing major neurovascular structures where R0/R1 resection would cause unacceptable morbidity (consider neoadjuvant systemic therapy). |
| Recurrent Disease | Symptomatic recurrence causing functional impairment; progression of bone cysts or cartilage wear. | Multiple prior failed synovectomies with severe arthrofibrosis; consider systemic CSF1R inhibitors or radiation therapy. |
| End Stage Osteoarthritis | Advanced joint destruction requiring Total Knee Arthroplasty (TKA) combined with extensive synovectomy. | Active intra-articular infection; inadequate soft tissue envelope for arthroplasty. |
Contraindications to immediate surgical intervention include active localized or systemic infection, severe medical comorbidities, and massive, unresectable disease encasing the popliteal neurovascular bundle. In the latter scenario, primary surgical resection carries an unacceptably high risk of limb-threatening ischemia or neuropathy. For these patients, neoadjuvant treatment with CSF1R inhibitors (e.g., pexidartinib) may be indicated to downstage the tumor, rendering it more amenable to subsequent surgical resection.
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is the linchpin of successful surgical management for diffuse TGCT. Advanced imaging is mandatory to delineate the full extent of synovial involvement, identify extra-articular extension, and map the proximity of the tumor to critical neurovascular structures.
Magnetic Resonance Imaging (MRI) is the gold standard modality. The classic MRI appearance of TGCT is characterized by nodular or villous synovial thickening that demonstrates low signal intensity on both T1-weighted and T2-weighted sequences. This low signal is attributable to the dense hemosiderin deposition within the tumor. The hallmark imaging feature is the "blooming artifact" observed on gradient-echo (GRE) or T2* sequences, where the paramagnetic properties of hemosiderin cause a focal loss of signal and an apparent enlargement of the lesion. Gadolinium contrast enhancement is typically robust due to the highly vascular nature of the stroma. The surgeon must systematically review the MRI to evaluate the suprapatellar pouch, the deep gutters, the intercondylar notch, the posterior recesses, and the popliteus hiatus. Any extension beyond the capsule dictates the need for potential open arthrotomy.
Patient positioning must facilitate comprehensive access to all compartments of the knee. The procedure is typically performed under general or regional anesthesia. The patient is positioned supine on the operating table. A standard tourniquet is applied to the proximal thigh to provide a bloodless surgical field, which is critical given the hypervascularity of TGCT.
Two primary positioning strategies are employed based on surgeon preference and the planned approach. The use of a lateral post allows the knee to rest in extension for anterior compartment work and enables valgus stress to open the medial compartment. Alternatively, a circumferential leg holder can be utilized, allowing the knee to be positioned in varying degrees of flexion, which is particularly advantageous for accessing the posterior compartments and creating a trans-septal portal. If a formal open posterior approach is anticipated due to massive posterior extra-articular extension, the surgeon must be prepared to position the patient prone, or utilize a "floating" position that allows intraoperative repositioning.
Detailed Surgical Approach and Technique
The surgical objective in diffuse TGCT is a complete, total synovectomy. Leaving residual macroscopic disease significantly increases the risk of rapid recurrence. The procedure demands a systematic, compartmentalized approach, often combining advanced arthroscopic techniques with open arthrotomies when necessary.
Arthroscopic Anterior Compartment Synovectomy
The procedure begins with standard anterolateral (AL) and anteromedial (AM) portals. Upon joint entry, the surgeon is typically greeted by a characteristic reddish-brown, hyperplastic, villonodular synovium. A thorough diagnostic arthroscopy is performed to correlate intraoperative findings with preoperative MRI.
To access the extensive volume of the suprapatellar pouch, standard portals are often insufficient. Superolateral and superomedial portals are routinely established. Utilizing a 30-degree and, crucially, a 70-degree arthroscope, the surgeon systematically resects the abnormal synovium using an aggressive oscillating shaver and radiofrequency ablation wands. The dissection must proceed down to the capsule, stripping the hyperplastic tissue while meticulously preserving the underlying capsular integrity.
The medial and lateral gutters must be cleared completely. The 70-degree scope is passed down the gutters to ensure no residual tissue is hidden in the deep recesses adjacent to the meniscocapsular junctions. The intercondylar notch is then addressed. The hypertrophic tissue often encases the Anterior Cruciate Ligament (ACL) and Posterior Cruciate Ligament (PCL). Careful dissection is required to skeletonize the cruciates without causing iatrogenic injury to their synovial envelopes or structural fibers.
Posterior Compartment Access and Trans Septal Portal
The posterior compartment represents the most technically demanding portion of the synovectomy. Standard anterior portals provide inadequate visualization of the posteromedial and posterolateral recesses. Dedicated posterior portals are mandatory for diffuse TGCT.
With the knee flexed to 90 degrees, a posteromedial portal is established under direct visualization. The arthroscope is passed through the intercondylar notch (the Gillquist maneuver) to visualize the posteromedial capsule. A spinal needle is used to localize the portal, ensuring it is superior to the medial meniscus and posterior to the medial collateral ligament.
To achieve complete posterior access, a trans-septal portal is created. The posterior septum, a fold of synovial tissue separating the posteromedial and posterolateral compartments, must be breached. From the posteromedial portal, a blunt switching stick or motorized shaver (without suction) is gently pushed through the posterior septum, staying immediately posterior to the PCL to avoid the popliteal artery, which lies directly posterior to the capsule. Once the septum is perforated, a posterolateral portal is established using a spinal needle for localization, guided by the instrument protruding through the septum.
With both posteromedial and posterolateral portals established, the surgeon can freely pass the arthroscope and instruments between the two compartments. This allows for a comprehensive, 360-degree visualization and resection of the posterior synovium. Extreme caution must be exercised when resecting tissue along the posterior capsule. The use of radiofrequency ablation should be minimized or used with precise control in this region to prevent thermal injury to the adjacent popliteal vessels and tibial nerve.
Open Arthrotomy Considerations
While arthroscopic techniques have advanced significantly, open arthrotomy remains a critical tool in the surgeon's armamentarium, particularly for cases with extensive extra-articular extension or massive tumor volume that cannot be efficiently or safely managed arthroscopically.
If MRI indicates substantial posterior extra-articular extension encasing the neurovascular bundle, a formal open posterior approach is indicated. This is typically performed with the patient in the prone position. A classic "lazy-S" incision is utilized across the popliteal fossa. The deep fascia is incised, and the neurovascular bundle (tibial nerve, popliteal vein, popliteal artery) is meticulously identified, isolated with vessel loops, and retracted. The tumor mass is then carefully dissected away from the vessels and the posterior joint capsule. This dissection can be exceptionally tedious, as the hypervascular tumor often adheres densely to the adventitia of the vessels.
For massive anterior disease, a standard midline anterior incision with a medial parapatellar arthrotomy allows for rapid and complete macroscopic clearance of the suprapatellar pouch and anterior gutters. In cases where end-stage osteoarthritis has developed secondary to chronic TGCT, a single-stage total knee arthroplasty (TKA) combined with an open radical synovectomy is the treatment of choice.
Complications and Management
The surgical management of diffuse TGCT is fraught with potential complications, driven by the aggressive nature of the disease and the extensive surgical dissection required for eradication. Preoperative patient counseling regarding these risks is mandatory.
| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Disease Recurrence | 30% - 50% | Prevention: Meticulous total synovectomy (arthroscopic + open if needed); use of 70-degree scope and posterior portals. Salvage: Repeat synovectomy; adjuvant radiosynoviorthesis (Yttrium-90); external beam radiation; systemic CSF1R inhibitors (pexidartinib). |
| Arthrofibrosis and Stiffness | 15% - 25% | Prevention: Early, aggressive postoperative continuous passive motion (CPM) and physical therapy; meticulous hemostasis to prevent postoperative hemarthrosis. Salvage: Arthroscopic lysis of adhesions; manipulation under anesthesia (MUA). |
| Neurovascular Injury | < 2% | Prevention: Thorough MRI preoperative mapping; meticulous technique during posterior portal placement and trans-septal portal creation; avoiding deep thermal ablation on the posterior capsule. Salvage: Immediate intraoperative vascular/nerve repair; urgent vascular surgery consultation if ischemia is suspected. |
| Postoperative Hemarthrosis | 5% - 10% | Prevention: Thorough electrocautery of raw capsular beds prior to tourniquet deflation; use of intra-articular drains; compressive dressings. Salvage: Joint aspiration; rarely requires surgical evacuation unless causing severe pain or impending compartment syndrome. |
| Infection | 1% - 3% | Prevention: Strict sterile technique; appropriate perioperative prophylactic antibiotics; minimizing operating time. Salvage: Prompt arthroscopic irrigation and debridement; culture-directed intravenous antibiotics. |
Recurrence is the most daunting challenge in diffuse TGCT. Because the disease is diffuse and infiltrative, microscopic residual disease is almost inevitable, even following the most meticulous surgical clearance. When recurrence occurs, it often presents with a return of effusions, pain, and mechanical symptoms. Management of recurrent disease requires a multidisciplinary approach. Repeat surgical synovectomy is often necessary but yields diminishing returns and increases the risk of severe arthrofibrosis. Consequently, adjuvant therapies are frequently employed for recurrent or highly aggressive primary disease.
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following a total synovectomy for diffuse TGCT must balance the need for early mobilization to prevent arthrofibrosis against the need to protect the healing capsular tissues and manage postoperative swelling.
Immediate, aggressive range of motion (ROM) is the primary goal. The extensive denudation of the joint capsule creates a highly inflammatory environment prone to rapid adhesion formation. Continuous Passive Motion (CPM) machines are frequently utilized in the immediate postoperative period, beginning in the recovery room. Patients are instructed to use the CPM for several hours daily, gradually increasing the flexion parameters as tolerated.
Weight-bearing status is generally dictated by the extent of the procedure. For an isolated arthroscopic or open synovectomy without concurrent bone grafting for subchondral cysts, patients are typically allowed to weight-bear as tolerated (WBAT) with crutches for assistance. If extensive curettage and bone grafting of juxta-articular cysts were performed, a period of restricted weight-bearing (e.g., toe-touch weight-bearing for 4 to 6 weeks) may be necessary to protect the structural integrity of the subchondral bone.
Physical therapy focuses on active and active-assisted ROM, patellar mobilization to prevent patella infera or retinacular scarring, and progressive quadriceps strengthening. Cryotherapy and compressive wraps are heavily utilized to manage the inevitable postoperative hemarthrosis and effusion. Return to high-impact activities is generally delayed until full, painless ROM and symmetrical quadriceps strength are achieved, typically taking 3 to 6 months.
Summary of Key Literature and Guidelines
The management paradigm for diffuse TGCT has evolved significantly over the past decade, transitioning from a purely surgical approach to a multidisciplinary strategy, largely driven by advances in molecular oncology.
Historically, the literature emphasized the necessity of open radical synovectomy to minimize recurrence. However, contemporary studies have demonstrated that advanced, multi-portal arthroscopic techniques can achieve comparable local control rates with significantly lower morbidity and improved functional outcomes, provided the surgeon is highly skilled in posterior compartment access. Verspoor et al. conducted extensive reviews highlighting that while arthroscopy is preferred, the recurrence rate for diffuse TGCT remains unacceptably high (often exceeding 40%), underscoring the limitations of mechanical resection alone.
The most paradigm-shifting literature in recent years relates to targeted systemic therapy. The identification of the CSF1/CSF1R axis as the primary driver of TGCT pathogenesis led to the development of CSF1R inhibitors. The ENLIVEN trial, a landmark phase 3, randomized, double-blind, placebo-controlled study, evaluated the efficacy of pexidartinib (a novel CSF1R inhibitor) in patients with advanced, symptomatic TGCT for whom surgery was not recommended. The trial demonstrated a robust and durable overall response rate in the pexidartinib cohort compared to placebo, leading to its FDA approval.
Current clinical guidelines advocate for a multidisciplinary tumor board approach. Surgery remains the first-line treatment for resectable disease. For patients with massive, unresectable tumors, or those facing highly morbid resections (e.g., requiring vascular reconstruction), neoadjuvant pexidartinib is increasingly utilized to downstage the tumor. Furthermore, in cases of multiple recurrences where further surgery risks severe functional impairment, systemic therapy or adjuvant radiation modalities (such as intra-articular Yttrium-90 radiosynoviorthesis or moderate-dose external beam radiation) are strongly recommended to achieve disease control and preserve joint function.
