Opening Wedge Osteotomy and Surgical Management of the Delta Phalanx
Key Takeaway
The opening wedge osteotomy of the terminal phalanx is a highly effective surgical intervention for correcting progressive angular deformities, such as clinodactyly and delta phalanx. This procedure restores digital alignment by utilizing a dorsal periosteal hinge and precise diaphyseal cuts. When combined with physiolysis or fat interposition in pediatric patients, it prevents progressive deformity, optimizes biomechanics, and ensures excellent long-term functional and aesthetic outcomes in the hand.
INTRODUCTION TO TERMINAL PHALANX DEFORMITIES
Angular deformities of the digits in the frontal plane, clinically referred to as clinodactyly, present a unique reconstructive challenge in pediatric and adult hand surgery. While mild angulation is frequently observed and often asymptomatic, severe progressive deformity can lead to profound functional impairment and unacceptable aesthetic outcomes.
The most common pathoanatomic etiology for severe, progressive clinodactyly is the presence of a delta phalanx—more accurately termed a longitudinally bracketed epiphysis (LBE). This anomaly most frequently manifests in the middle phalanx of the small finger and the proximal phalanx of the thumb (often in association with a triphalangeal thumb). The next most frequent location is the proximal phalanx of the ring finger. In border digits, the presence of a delta phalanx invariably causes the finger to deviate toward the midline of the hand.
Because progressive angulation is inevitable in the presence of a true delta phalanx, nonoperative management is ineffective. Operative intervention is mandated for moderate to severe cases, with the primary surgical goals being to narrow the digit, straighten the phalanx, and ablate the abnormal tethering portion of the epiphysis.
This comprehensive guide details the Opening Wedge Osteotomy of the Terminal Phalanx as described by Carstam and Eiken, alongside the contemporary management of the delta phalanx utilizing physiolysis and osteotomy techniques pioneered by Vickers, and further refined by Strauss and Goldfarb.
PATHOANATOMY AND BIOMECHANICS
Understanding the biomechanical tethering caused by the delta phalanx is critical for successful surgical correction.
A normal phalanx possesses a single transverse proximal physis. In contrast, a delta phalanx is characterized by a continuous, C-shaped physis that brackets the diaphysis longitudinally. This abnormal physeal bracket restricts longitudinal growth on the affected side while allowing continued growth on the contralateral side. The result is a progressive, trapezoidal or triangular (delta) shaping of the bone, leading to severe angular deviation.
💡 Clinical Pearl: The Tethering Effect
The longitudinally bracketed epiphysis acts as an unyielding tether. As the normal side of the physis continues to grow, the bracketed side acts as a hinge, forcing the digit into progressive clinodactyly. Surgical intervention must either destroy this tether (physiolysis) or correct the established bony deformity (osteotomy).
If the delta phalanx is associated with central polydactyly, the abnormal phalanx should be excised entirely along with the extra digit, followed by a syndactyly-type reconstruction. In cases associated with a triphalangeal thumb, the delta phalanx is typically excised, necessitating meticulous reconstruction of the joint ligaments to restore stability.
PREOPERATIVE EVALUATION AND SURGICAL TIMING
Radiographic Assessment
Standard posteroanterior (PA), true lateral, and oblique radiographs of the affected digit are mandatory. The PA radiograph will clearly demonstrate the trapezoidal shape of the phalanx and the continuous C-shaped epiphysis.
Age-Based Treatment Algorithm
The timing of surgical intervention dictates the choice of procedure. Strauss and Goldfarb recommend a distinct age-based algorithm for the correction of clinodactyly caused by a delta phalanx:
* Children < 5 Years Old: A Vickers-type procedure (physiolysis with fat interposition) is recommended. Resecting the abnormal physeal bracket early allows for spontaneous angular correction and normalized longitudinal growth of the phalanx.
* Children > 5 Years Old and Adults: An opening wedge osteotomy (with or without bone grafting) is required, as the remaining growth potential is insufficient for spontaneous correction following physiolysis alone.
SURGICAL TECHNIQUE: OPENING WEDGE OSTEOTOMY OF THE TERMINAL PHALANX
The opening wedge osteotomy, originally popularized by Carstam and Eiken, is a powerful technique for correcting established angular deformities of the terminal phalanx. Reverse wedge osteotomies, as described by Carstam and Theander, have been shown to eliminate or markedly reduce clinodactyly with a lower recurrence rate compared to simple closing wedge osteotomies.
1. Patient Positioning and Preparation
- The patient is placed supine with the affected upper extremity extended on a radiolucent hand table.
- General anesthesia or a regional block is administered.
- A well-padded pediatric or digital tourniquet is applied to ensure a bloodless surgical field.
- Loupe magnification (2.5x to 3.5x) is highly recommended to protect the delicate neurovascular structures.
2. Surgical Approach
- Under tourniquet control, make a precise radial midlateral incision over the distal phalanx of the involved finger.
- Carefully dissect through the subcutaneous tissues. Identify and protect the terminal branches of the digital nerve and artery, retracting them volarly.
- Incise the periosteum longitudinally and expose the distal phalanx subperiosteally. Meticulous subperiosteal dissection is critical to preserve the soft tissue envelope and the vascularity of the bone.
3. Execution of the Osteotomy
- Perform two transverse osteotomies through the volar three-fourths of the diaphysis using a fine oscillating saw or a sharp micro-osteotome.
- CRITICAL STEP: Leave the dorsal periosteum and the dorsal one-fourth of the bony cortex intact. This creates a periosteal hinge.
⚠️ Surgical Warning: The Periosteal Hinge
The dorsal periosteal hinge must remain intact. This hinge is the biomechanical cornerstone of the procedure—it acts as a tension band during the opening of the wedge, prevents catastrophic displacement of the distal fragment, and provides absolute control over the rotation of the fragments.
- Gently apply an opening force to correct the angular deformity. The intact dorsal hinge will guide the correction.
- Note: Complete correction of the deformity may occasionally be blocked by a severe, curved nail deformity. In such cases, the nail matrix may require partial elevation or release from the underlying periosteum to permit full bony correction.
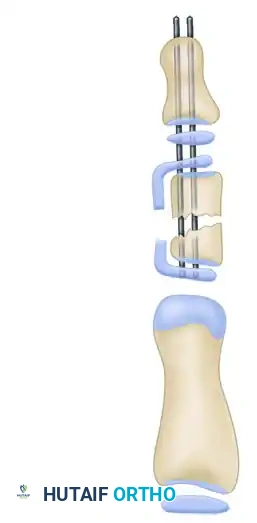
4. Fixation and Closure
- Once anatomic alignment is achieved, place a longitudinal Kirschner wire (K-wire) (typically 0.028 or 0.035 inch) retrograde through the tip of the distal phalanx, across the osteotomy site, and across the distal interphalangeal (DIP) joint to hold the correction rigidly.
- Alternative for Extremely Small Phalanges: If the phalanx is too small to accommodate an intramedullary wire without shattering, insert a K-wire extraperiosteally along the volar aspect of the phalanx. This acts as an internal splint to maintain alignment without violating the diminutive medullary canal.
- Deflate the tourniquet, obtain meticulous hemostasis, and close the skin incisions in a routine fashion using non-absorbable monofilament sutures.
- Apply a sterile, non-adherent dressing followed by a protective long-arm or short-arm splint, depending on the patient's age and compliance level.
SURGICAL TECHNIQUE: MANAGEMENT OF THE DELTA PHALANX (STRAUSS & GOLDFARB PROCEDURE)
For patients presenting with a true delta phalanx, the surgical approach must address the abnormal physeal bracket. The following sequence illustrates the Strauss and Goldfarb technique, which incorporates the principles of the Vickers physiolysis for younger children, and osteotomy for older patients.
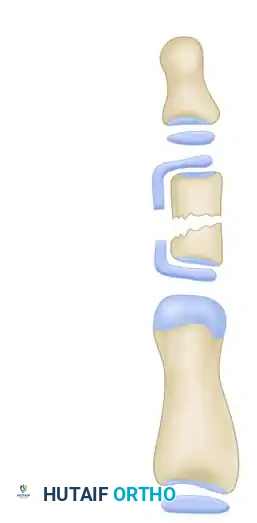
Phase 1: Identification of the Deformity
The initial exposure reveals the classic delta phalanx. The longitudinally bracketed epiphysis is clearly visible, tethering the diaphysis and preventing normal longitudinal growth on the affected side.

This tethering results in the characteristic angular deformity (clinodactyly) in the frontal plane. The apex of the deformity points away from the tethered side.
Phase 2: Physiolysis (The Vickers Procedure)
In children under 5 years of age, resection of the abnormal physeal bracket (physiolysis) is the treatment of choice. Caouette-Laberge et al. and Vickers have both reported excellent spontaneous angular correction and resumption of normal longitudinal growth following this technique.

Using a sharp scalpel or a fine micro-osteotome, the surgeon begins the resection of the isthmus of the continuous epiphysis. The goal is to completely ablate the abnormal physeal tissue that bridges the proximal and distal ends of the bone.

The resection is carried deeply into the bone to ensure no residual physeal cells remain. Incomplete resection will inevitably lead to the reformation of a physeal bar and recurrence of the deformity.

Once the bracket is fully excised, a distinct gap is created in the lateral aspect of the phalanx. The tethering effect is now released, allowing the bone the potential to remodel and grow symmetrically.
Phase 3: Fat Interposition
To prevent the bone from healing across the resection gap and reforming the tethering bar, an interpositional material must be placed.

A free fat graft is harvested—typically from the hypothenar eminence or the proximal forearm—and meticulously packed into the resection defect. This fat interposition acts as a biologic spacer, permanently preventing the reformation of the bony/physeal bridge.
Phase 4: Osteotomy and Fixation (For Older Children)
If the patient is older (> 5 years), physiolysis alone is insufficient because the remaining growth potential cannot spontaneously correct the established angular deformity. In these cases, an opening wedge osteotomy is performed concurrently.
Following the osteotomy, the phalanx is straightened. The correction is rigidly stabilized using longitudinal K-wires. If a large opening wedge is created, structural bone graft (autograft or allograft) may be inserted into the void to promote rapid osseous union and maintain the corrected length and alignment.
POSTOPERATIVE CARE AND REHABILITATION
Meticulous postoperative care is essential to ensure bony union and prevent stiffness in the adjacent joints.
- Immobilization: The digit is immobilized in a protective splint immediately following surgery. For pediatric patients, a long-arm cast extending to include the affected digit is often preferred to prevent accidental removal or trauma to the K-wires.
- Pin Management: The K-wires and the splint are typically left in place for 4 to 6 weeks postoperatively. Pin sites must be kept clean and dry to prevent superficial tract infections.
- Radiographic Follow-up: Serial radiographs are obtained at 2 weeks and 4 weeks to assess the maintenance of alignment and the progression of bony healing at the osteotomy site.
- Pin Removal: Once clinical and radiographic signs of healing are evident (bridging callus or obliteration of the osteotomy line), the K-wires are removed in the clinic.
- Rehabilitation: Usually, no specific, intensive postoperative hand therapy is necessary for isolated terminal phalanx osteotomies. Active and passive range of motion exercises are initiated immediately upon pin removal. Full activities are permitted gradually, guided by the radiographic consolidation of the osteotomy.
COMPLICATIONS AND PITFALLS
While generally highly successful, surgeons must be prepared to manage potential complications:
- Recurrence of Deformity: The most common complication, particularly if the physeal bracket is incompletely resected during a Vickers procedure, or if the fat interposition fails, leading to the reformation of a physeal bar. Recurrence may necessitate a revision osteotomy at skeletal maturity.
- Nonunion or Delayed Union: Rare in the pediatric population but can occur if the periosteal hinge is completely violated or if the fixation is unstable.
- Nail Bed Deformity: Aggressive dissection dorsally or failure to address a pre-existing curved nail deformity can lead to ridging or splitting of the nail plate.
- Joint Stiffness: Prolonged transarticular K-wire fixation across the DIP joint can lead to temporary or permanent stiffness. Pins should be removed promptly at 4 to 6 weeks once clinical union is achieved.
CONCLUSION
The management of clinodactyly and the delta phalanx requires a nuanced understanding of pediatric physeal anatomy and precise surgical execution. The opening wedge osteotomy of the terminal phalanx, utilizing a dorsal periosteal hinge, provides reliable correction of angular deformities. By adhering to age-specific algorithms—employing physiolysis with fat interposition in young children and definitive osteotomies in older patients—orthopedic surgeons can achieve excellent, long-lasting functional and cosmetic outcomes.
📚 Medical References
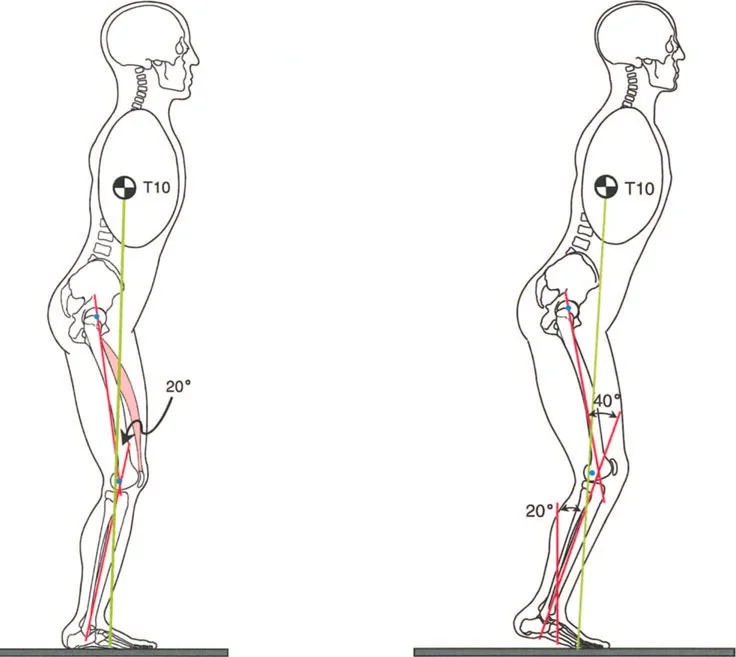
- opening wedge osteotomy in ankylosing spondylitis with thoracolumbar kyphotic deformity, Spine 30:1584, 2005.
- Chen IH, Chien JT, Yu TC: Transpedicular wedge osteotomy for correction of thoracolumbar kyphosis in ankylosing spondylitis: experience with 78 patients, Spine 26:E354, 2001.
- Collie DA, Smith GW, Merrick MV: 99mTc-MDP scintigraphy in ankylosing spondylitis, Clin Radiol 48:392, 1993.
- Danisa OA, Turner D, Richardson WJ: Surgical correction of lumbar kyphotic deformity: posterior reduction “eggshell” osteotomy, J Neurosurg 92(suppl 1):50, 2000.
- Detwiler KN, Loftus CM, Godersky JC, et al: Management of
You Might Also Like