Open Lateral Release, Medial Reefing, and MPFL Reconstruction: A Comprehensive Surgical Guide
Key Takeaway
Open lateral release and mini-open medial reefing are foundational procedures for addressing patellofemoral maltracking and instability. This guide details the Nam and Karzel technique, emphasizing precise retinacular release, superolateral geniculate artery hemostasis, and anatomic medial reefing using mattress sutures. Proper execution restores patellar kinematics, while concurrent MPFL reconstruction provides robust stabilization for chronic cases, preventing recurrent dislocation and patellofemoral arthrosis.
Comprehensive Introduction and Patho-Epidemiology
Patellofemoral instability and maltracking present a profoundly complex biomechanical challenge that demands a nuanced, patient-specific, and highly anatomical surgical approach. Historically, isolated lateral retinacular release was egregiously overutilized as a panacea for undifferentiated anterior knee pain and presumed instability. This non-specific application often led to suboptimal functional outcomes, persistent pain, or, most devastatingly, iatrogenic medial patellar subluxation—a complication that is notoriously difficult to salvage. In contemporary orthopedic practice, the indications for patellofemoral interventions have been rigorously refined. Open lateral release is now strictly reserved for documented lateral patellar compression syndrome with a structurally tight lateral retinaculum, or it is utilized as an essential, carefully titrated adjunct to medial-sided stabilization procedures. The paradigm has shifted irrevocably from isolated release to comprehensive, a la carte patellofemoral reconstruction.
The pathophysiology of patellofemoral instability is multifactorial, encompassing a spectrum from acute traumatic dislocations in patients with normal anatomy to recurrent subluxations in patients with severe underlying dysplasia. When lateral retinacular tightness is coupled with medial-sided incompetence—a scenario frequently encountered following acute or recurrent lateral patellar dislocations—a combined surgical approach is unequivocally mandated. The structural failure of the medial patellofemoral ligament (MPFL), which ruptures in over 90% of lateral patellar dislocations, drastically alters the kinematic equilibrium of the extensor mechanism. If left unaddressed, the lateral vector forces perpetually overpower the deficient medial restraints, leading to recurrent instability, progressive chondral sheer injury, and eventual patellofemoral arthrosis.
Epidemiologically, patellofemoral instability predominantly affects a young, active demographic, with a notable predilection for adolescent females. The incidence of primary patellar dislocation is estimated at 23 to 77 per 100,000 person-years, with the highest rates observed in females aged 10 to 17 years. Following a primary dislocation, the risk of recurrence is alarmingly high, ranging from 15% to 44% with conservative management, and escalating to over 50% if a second dislocation occurs. This high recurrence rate underscores the critical necessity for precise surgical intervention in appropriately selected candidates. The decision to proceed with surgery must account for the patient's physiological age, activity level, and the presence of pathoanatomic risk factors, including trochlear dysplasia, patella alta, and an elevated tibial tubercle-trochlear groove (TT-TG) distance.
To address these complex pathologies, modern surgical techniques have evolved significantly. The mini-open medial reefing combined with an arthroscopic or open lateral release (as popularized by Nam and Karzel) provides a powerful, anatomically respectful method to restore the delicate soft-tissue balance of the patellofemoral joint in cases of mild to moderate tissue attenuation. However, in cases of chronic, recurrent instability with severe MPFL attenuation or complete absence of robust medial tissue, formal MPFL reconstruction using a semitendinosus autograft or allograft has emerged as the definitive gold standard. This comprehensive guide details the biomechanical rationale, precise surgical steps, and evidence-based postoperative protocols for open lateral release, mini-open medial reefing, and MPFL reconstruction.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Geometry
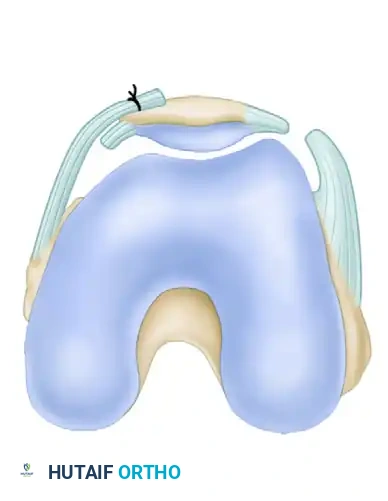
The stability of the patellofemoral joint relies on a highly sophisticated interplay of static and dynamic restraints, heavily dependent on the joint's flexion angle. The bony architecture of the trochlear groove provides the primary static stability at flexion angles greater than 30 degrees. The patella, the largest sesamoid bone in the human body, articulates with the femoral trochlea, a complex geometric surface characterized by a deeper central groove and a more prominent lateral facet. This lateral prominence acts as a critical bony buttress against lateral patellar translation. Dysplasia of the trochlea, classified by Dejour into types A through D, fundamentally compromises this bony stability. In severe dysplasia (Types B, C, and D), the loss of the lateral buttress or the presence of a convex trochlear floor renders the patella entirely dependent on soft-tissue restraints, predisposing the joint to recurrent catastrophic failure.
Medial Soft-Tissue Restraints
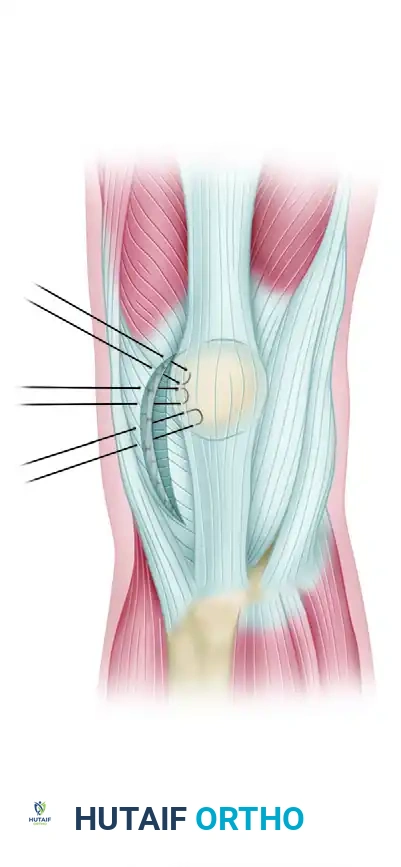
The medial soft-tissue architecture is complex, classically described by Warren and Marshall in three distinct layers. The MPFL, situated in layer 2, is the primary soft-tissue restraint to lateral patellar translation. Biomechanical studies conclusively demonstrate that the MPFL contributes 50% to 60% of the total restraining force against lateral displacement from 0 to 30 degrees of knee flexion, the critical arc of motion before the patella fully engages the trochlear groove. The MPFL originates from a highly specific anatomic footprint on the medial femur, located in a saddle-shaped depression between the medial epicondyle and the adductor tubercle, extending distally to insert on the proximal half of the medial patellar border. The ligament is relatively thin, with an average tensile strength of only 208 Newtons, explaining its high susceptibility to rupture during a lateral dislocation event. Secondary medial restraints include the medial patellomeniscal ligament (MPML) and the medial patellotibial ligament (MPTL), which provide restraint at higher degrees of flexion.
Lateral Soft-Tissue Restraints
Conversely, the lateral soft-tissue restraints exert a continuous laterally directed vector force on the patella. The lateral retinaculum is composed of superficial and deep layers. The superficial layer includes the oblique fibers of the vastus lateralis and the iliotibial (IT) band expansion. The deep layer comprises the transverse epicondylopatellar ligament, the deep transverse retinaculum, and the patellotibial band. Pathologic contracture of these lateral structures, often secondary to chronic maltracking or prior trauma, results in lateral patellar compression syndrome. This contracture not only exacerbates lateral subluxation but also dramatically increases contact pressures on the lateral patellar facet, leading to accelerated chondromalacia and anterior knee pain. An intimate understanding of these layers is imperative during an open lateral release to ensure adequate decompression without violating the essential dynamic stabilizers.
Dynamic Muscle Vectors and Joint Kinematics
The dynamic restraints of the patellofemoral joint are governed by the quadriceps musculature. The vastus medialis obliquus (VMO) dynamically pulls the patella medially and proximally, with its fibers orienting at approximately 50 to 55 degrees relative to the femoral shaft. This medial vector is essential for countering the lateral forces generated by the vastus lateralis (VL) and the IT band. In patients with patellofemoral instability, VMO dysplasia or delayed neuromuscular firing patterns are frequently observed, further exacerbating lateral maltracking. The overall vector of the extensor mechanism is clinically estimated by the Q-angle, formed by a line from the anterior superior iliac spine (ASIS) to the center of the patella, intersecting with a line from the tibial tubercle to the center of the patella. An exaggerated Q-angle increases the lateralizing force on the patella during quadriceps contraction, predisposing the patient to instability and necessitating meticulous evaluation prior to any soft-tissue stabilization procedure.
Exhaustive Indications and Contraindications
The decision-making algorithm for patellofemoral surgery is highly complex and must be strictly individualized. Soft-tissue procedures (lateral release, medial reefing, MPFL reconstruction) are highly effective when the primary pathology is soft-tissue incompetence or imbalance. However, these procedures are doomed to failure if utilized in isolation to treat severe underlying bony deformities. An isolated lateral release is now rarely indicated; it is reserved almost exclusively for patients with pure lateral patellar compression syndrome who have failed exhaustive conservative management, demonstrating a negative patellar tilt test and normal medial restraints.
Medial reefing (imbrication) is indicated in patients with mild to moderate recurrent instability who possess sufficient, viable medial capsular tissue. It is particularly useful in younger patients or those with a history of recurrent subluxations rather than frank, high-energy dislocations that obliterate the MPFL. MPFL reconstruction, utilizing an autograft or allograft, is the definitive procedure for patients with recurrent dislocations, a grossly incompetent or absent MPFL on MRI, and a positive apprehension sign at low flexion angles. It is considered the gold standard for restoring the medial check-rein function in the chronic dislocator.
Crucially, soft-tissue procedures are contraindicated in the presence of severe bony malalignment. If a patient exhibits a TT-TG distance greater than 20 mm, a concurrent tibial tubercle osteotomy (TTO) must be performed to medialise the extensor mechanism. Similarly, severe patella alta (Caton-Deschamps index > 1.2) requires a distalizing TTO to allow the patella to engage the trochlea at earlier flexion angles. Performing an isolated MPFL reconstruction in a patient with a TT-TG of 24 mm will inevitably lead to graft stretching, failure, and recurrent dislocation due to the overwhelming lateral vector forces.
| Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Open Lateral Release | Documented lateral patellar compression syndrome; adjunct to medial stabilization; rigid, untiltable patella. | Hypermobility syndromes; normal or hypermobile lateral glide; isolated anterior knee pain without compression. | Mild patellofemoral osteoarthritis; active intra-articular infection. |
| Mini-Open Medial Reefing | Recurrent subluxation with viable medial tissue; mild instability; adjunct to lateral release in balanced realignment. | Complete MPFL avulsion with tissue retraction; severe trochlear dysplasia (Dejour C/D); TT-TG > 20 mm. | Chronic dislocations with obliterated medial tissue; extreme obesity. |
| MPFL Reconstruction | Recurrent frank dislocations; absent/incompetent MPFL on MRI; failure of prior medial reefing; positive apprehension test. | Uncorrected TT-TG > 20 mm (requires TTO); uncorrected severe patella alta; severe tricompartmental osteoarthritis. | Open physes (requires specific physeal-sparing techniques); active infection. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Examination Under Anesthesia
A meticulous examination under anesthesia (EUA) is the absolute critical first step in the operating room, serving as the final confirmation of the preoperative surgical plan. With muscle guarding eliminated, the surgeon must systematically document the baseline range of motion, patellar tilt, and the degree of medial and lateral glide. The patellar glide test is performed at 0 and 30 degrees of flexion. A normal lateral glide is 1 to 2 quadrants of the patellar width. A lateral glide of 3 or more quadrants lacking a firm endpoint indicates gross MPFL incompetence and mandates medial-sided reconstruction. Conversely, an inability to evert the patella past the horizontal plane (a negative patellar tilt test) or a medial glide of less than 1 quadrant indicates severe lateral retinacular tightness, justifying a concomitant lateral release.
Radiographic Evaluation and Advanced Imaging
Preoperative imaging must be exhaustive. Standard weight-bearing anteroposterior (AP), true lateral, and axial (Merchant or skyline) radiographs are mandatory. The true lateral radiograph is scrutinized to assess patellar height using the Caton-Deschamps or Insall-Salvati indices, and to identify signs of trochlear dysplasia, such as the crossing sign, double contour sign, or a supratrochlear spur. Axial views provide insight into dynamic patellar tilt and lateral subluxation.
Advanced imaging with Magnetic Resonance Imaging (MRI) is non-negotiable in the modern era. MRI evaluates the structural integrity of the MPFL, precisely locating the site of tearing (femoral, mid-substance, or patellar). It is also critical for identifying osteochondral shear fractures, which occur in up to 40% of acute dislocations and may require concurrent fixation or cartilage restoration. Furthermore, axial MRI or Computed Tomography (CT) scans are utilized to calculate the TT-TG distance. The surgeon must template the femoral origin of the MPFL (Schöttle's point) preoperatively, utilizing the true lateral radiographic view to ensure precise intraoperative tunnel placement.
Patient Positioning and Operating Room Setup
The patient is placed supine on a standard radiolucent operating table. A proximal thigh tourniquet is applied but typically not inflated unless visualization becomes critically compromised, as tourniquet inflation can artificially tether the quadriceps mechanism and alter intraoperative kinematic assessments. A lateral post and a foot piece are positioned to allow full, unhindered knee flexion to 120 degrees and full extension. The contralateral leg is placed in a well-padded gynecologic stirrup or allowed to rest flat, depending on surgeon preference and fluoroscopy access. The limb is prepped and draped in a standard sterile fashion. It is imperative that the draping allows for the unimpeded introduction of a C-arm fluoroscope from the contralateral side to confirm the physiometric point for MPFL femoral fixation.
Step-by-Step Surgical Approach and Fixation Technique
Diagnostic Arthroscopy and Open Lateral Release
An open lateral release allows for precise, controlled division of the lateral retinaculum while minimizing the risk of postoperative hemarthrosis—a notorious and highly morbid complication of purely arthroscopic releases.
The procedure commences with a comprehensive diagnostic arthroscopy via standard inferolateral and inferomedial portals. The surgeon evaluates patellar tracking dynamically from the superolateral portal, observing the patella as it enters the trochlea during knee flexion. Any concomitant chondral lesions are treated with judicious chondroplasty, and meniscal pathology is addressed prior to the extra-articular work.
For the open lateral release, a dedicated superior anterolateral 2-cm incision is made, starting just lateral to the proximal pole of the patella. This specific superior approach is critical for direct visualization. Using Metcalf-type scissors, the retinacular release is extended distally to the level of the tibial tuberosity, dividing the deep transverse retinaculum. The release is then carefully extended proximally to the superolateral edge of the patella. Crucially, the surgeon must release only the lateral third of the vastus lateralis tendon. This release is extended obliquely, strictly in line with the vastus lateralis muscle fibers superiorly and laterally. Over-release of the vastus lateralis is a catastrophic technical error that destroys the dynamic lateral stabilizer, leading to profound quadriceps weakness and iatrogenic medial instability. The lateral capsule is released down to, but preserving where possible, the underlying synovium to maintain a barrier against intra-articular bleeding. The superolateral genicular artery is directly visualized and meticulously coagulated using bipolar electrocautery.
Mini-Open Medial Reefing Technique
When lateral release alone is insufficient due to medial incompetence, the Nam and Karzel mini-open medial reefing technique provides an anatomic, robust imbrication of the medial structures.
A 4-cm longitudinal incision is made starting at the level of the superior pole of the patella, positioned 2 cm medial and parallel to the medial border of the patella, extending distally. The dissection is carried sharply down through the subcutaneous tissues to expose the extensor mechanism. The vastus medialis and the medial retinaculum are identified and carefully inspected for any areas of traumatic detachment or interstitial tearing. The integrity of the tissue at the adductor tubercle attachment site is assessed by grasping the medial structures with a Kocher clamp and applying lateral traction.
The surgeon carefully incises the vastus medialis and medial retinaculum along the medial border of the patella down to, but not through, the level of the synovium. Preserving the synovium prevents intra-articular extravasation of extra-articular hematoma.
Using heavy, non-absorbable braided sutures (e.g., No. 2 Ethibond), the medial retinaculum is advanced to the medial border of the patella. A minimum of four horizontal mattress sutures are placed to ensure a broad, secure area of tissue imbrication. The mattress configuration is vital as it prevents tissue pull-through under the high tensile loads generated by the extensor mechanism during early rehabilitation.
Before the sutures are permanently tied, a trial tensioning is performed. The knee is taken through a full range of motion.
The surgeon must ensure congruent tracking of the patella within the trochlear groove. The knee must be able to achieve at least 90 degrees of flexion without excessive, unyielding tension on the medial repair. The arthroscope is reintroduced to directly visualize the patellofemoral articulation, confirming the centralization of the patella. The final fixation is achieved by tying the sutures securely with the knee held in full extension. Closing in extension is a critical step; it prevents over-constraining the medial compartment, which would otherwise lead to a devastating loss of flexion and elevated patellofemoral contact pressures.
Medial Patellofemoral Ligament Reconstruction
For patients with chronic instability or an extensively damaged MPFL that cannot be primarily reefed, formal reconstruction using a semitendinosus hamstring tendon autograft is indicated.
The ipsilateral semitendinosus tendon is harvested using a standard open tendon stripper technique via a 3-cm incision over the pes anserinus. The graft is prepared by whipstitching both ends with high-strength non-absorbable suture and doubled to create a robust, two-strand construct.
Femoral fixation is arguably the most critical step of the procedure. A 3-cm incision is made over the site of the MPFL femoral origin. Using strict fluoroscopic guidance on a true lateral image, Schöttle's point is identified: 1 mm anterior to the posterior cortical line extension, 2.5 mm distal to the posterior articular border of the medial femoral condyle, and proximal to the level of the posterior point of Blumensaat's line. A guide pin is placed, and a femoral socket is drilled.
For patellar fixation, the medial border of the patella is exposed. Two transverse drill holes or two suture anchors are placed along the proximal half of the medial patellar border, replicating the native broad insertion of the MPFL. The free ends of the doubled graft are secured to the patella.
The most critical technical aspect of MPFL reconstruction is isometry and tensioning. The graft must act as a check-rein, not a dynamic medializer. With the graft fixed to the patella and passed into the femoral tunnel, the knee is cycled. The graft is tensioned at 30 degrees of flexion with only enough force to eliminate lateral laxity (typically 2-10 Newtons). The surgeon must ensure that a lateral glide of 1 to 2 quadrants is still possible. Once optimal tension is confirmed, the graft is secured in the femur using an interference screw.
Complications, Incidence Rates, and Salvage Management
While highly successful when meticulously indicated and executed, patellofemoral stabilization procedures carry specific, potentially severe risks. The surgeon must be intimately familiar with these complications and possess the technical armamentarium to manage them.
Hemarthrosis is the most frequent complication following lateral release, historically reported in up to 10% of arthroscopic procedures. The open technique significantly mitigates this risk by allowing direct visualization and cauterization of the superolateral genicular artery. If a massive hemarthrosis occurs, it causes severe capsular distension, excruciating pain, and profound quadriceps inhibition. Early, sterile aspiration in the clinical setting may be required to evacuate the hematoma and facilitate early rehabilitation.
Iatrogenic medial subluxation is a devastating complication caused by an over-aggressive lateral release that excessively violates the vastus lateralis tendon or the lateral capsule. Patients present with medial-sided knee pain, a sensation of instability when turning inward, and a positive medial apprehension sign. Salvage management is highly complex, often requiring a formal lateral retinacular reconstruction using an IT band slip or an allograft to restore the lateral tether.
Loss of knee flexion is a frequent complication following medial reefing or MPFL reconstruction, almost exclusively due to technical errors in tensioning. Over-tensioning the medial structures or placing the femoral tunnel in a non-anatomic (non-physiometric) position results in the graft acting as a rigid tether during flexion. If aggressive, supervised physical therapy fails to restore motion by 12 weeks, arthroscopic lysis of adhesions and potential open graft release or revision may be necessary.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Postoperative Hemarthrosis | 2% - 10% | Use open technique; meticulously cauterize superolateral genicular artery; utilize intra-articular drain. | Sterile joint aspiration; compressive bracing; rarely requires arthroscopic washout. |
| Iatrogenic Medial Subluxation | 1% - 3% | Avoid releasing vastus lateralis tendon; preserve deep capsule where possible; never perform isolated release for generalized instability. | Lateral retinacular reconstruction (IT band autograft or allograft); intensive VMO inhibition therapy. |
| Loss of Knee Flexion (< 90°) | 5% - 15% | Tension MPFL graft at 30° flexion with minimal force (2-10N); tie medial reefing sutures in full extension; ensure anatomic femoral tunnel placement. | Aggressive physical therapy; manipulation under anesthesia (MUA); arthroscopic lysis of adhesions; graft revision. |
| Recurrent Lateral Instability | 5% - 20% | Recognize and address bony abnormalities (TT-TG >20mm, patella alta); ensure robust graft fixation. | Revision MPFL reconstruction; concurrent Tibial Tubercle Osteotomy (TTO) or trochleoplasty. |
Phased Post-Operative Rehabilitation Protocols
A meticulously executed surgery can be easily, and rapidly, undone by an inappropriate or overly aggressive rehabilitation protocol. The postoperative care must delicately balance the protection of the healing soft tissues with the prevention of arthrofibrosis and the restoration of dynamic quadriceps control. The protocol is divided into four distinct, criterion-based phases.
Phase 1: Protection and Healing (Weeks 0-2)
The immediate postoperative phase focuses on edema control, wound healing, and protecting the surgical repair. The intra-articular drain (if utilized during the open lateral release) is removed after 24 hours. The patient is placed in a hinged knee brace locked in full extension for approximately 48 hours to reduce initial swelling and protect the medial repair from sudden flexion forces. The patient is allowed to bear weight as tolerated (WBAT) while locked in the knee immobilizer, utilizing crutches for balance. After 48 hours, the immobilizer is unlocked for seated, passive range-of-motion (ROM) exercises (0 to 90 degrees). Early, controlled motion is critical to prevent intra-articular adhesions and nourish the articular cartilage. Active quadriceps sets and straight-leg raises (SLR) are initiated, but must be performed with the brace locked in extension to prevent extensor lag and undue stress on the patellofemoral joint.
Phase 2: Early Strengthening and Neuromuscular Control (Weeks 2-6)
As the soft tissues begin to heal and quadriceps control improves, the focus shifts to restoring normal gait and initiating early strengthening. At 2 to 3 weeks postoperatively, the locked brace is gradually weaned as the patient demonstrates a straight-leg raise without an extensor lag. A formal physical therapy program is intensified. Exercises progress to gentle, closed-kinetic-chain strengthening (e.g., mini-squats, leg presses) strictly limited to 0-45 degrees of flexion. This limited arc minimizes patellofemoral joint reaction forces while effectively recruiting the quadriceps. Open-chain knee extensions (e.g., seated leg extension machines) are strictly and universally avoided during this phase, as they generate massive shear forces on the patellofemoral joint and place catastrophic tensile loads on the healing medial repair or MPFL graft.
Phase 3: Advanced Strengthening and Proprioception (Weeks 6-12)
By week 6, the graft or reefed tissue has achieved significant biological incorporation. The goal of Phase 3 is to restore full, symmetrical range of motion and advance muscular strength. Closed-chain exercises are progressed in depth and resistance. Proprioceptive training is heavily emphasized, utilizing balance boards and unstable surfaces to retrain the dynamic stabilizing reflexes of the lower extremity. Core stability and hip abductor/external rotator strengthening are integrated, as proximal control is essential for preventing functional valgus collapse of the knee, a primary mechanism for lateral patellar subluxation.
Phase 4: Return to Play and Functional Milestones (Weeks 12-16+)
The final phase prepares the athlete for a safe return to unrestricted activities. Progression to running, cutting, and sport-specific drills is permitted only when strict clinical criteria are met. Patients must achieve full, painless range of motion, absence of effusion, and symmetric quadriceps strength. Isokinetic testing is frequently utilized; the patient must demonstrate a Limb Symmetry Index (LSI) of at least 85% to 90% compared to the contralateral limb before clearance for contact sports. Return to play is typically achieved between 4 to 6 months postoperatively, contingent entirely on the individual's progression through the functional milestones.
Summary of Landmark Literature and Clinical Guidelines
The evolution of patellofemoral surgery is deeply rooted in landmark biomechanical and clinical literature. Historically, the work of Fulkerson established the foundation for understanding patellofemoral malalignment and the distinct entities of instability versus compression syndrome. His classification systems remain integral to preoperative planning. The monumental contributions of Henri Dejour and the Lyon school revolutionized the understanding of trochlear dysplasia, shifting the global perspective to recognize bony architecture as the primary dictator of high-grade instability.
The biomechanical rationale for MPFL reconstruction was solidified by the seminal in vitro studies of Amis et al., which definitively quantified the MPFL as the primary restraint to lateral patellar translation in early flexion. This work directly catalyzed the shift away from non-anatomic medial reefing towards anatomic ligament reconstruction in chronic cases. The identification of the precise femoral isometric point by Philip Schöttle (Schöttle's point) provided surgeons with a reliable, reproducible fluoroscopic landmark, drastically reducing the incidence of graft over-tensioning and subsequent joint stiffness.
For patients with less severe instability, the clinical outcomes of the mini-open medial reefing technique, as published by Nam and Karzel, demonstrated excellent mid-to-long-term results when appropriately indicated. Their work highlighted the efficacy of preserving the synovial layer and utilizing robust mattress sutures to achieve a balanced, dynamic repair without the morbidity of graft harvest.
Current clinical practice guidelines, including consensus statements from the American Academy of Orthopaedic Surgeons (AAOS) and the European Society for Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA), strongly advocate for a pathoanatomic approach. Isolated lateral release is universally condemned for the treatment of instability. Surgical intervention must be tailored to correct the specific anatomical deficits identified on advanced imaging, utilizing soft-tissue reconstructions for ligamentous incompetence and bony osteotomies for severe structural malalignment.
