Medial Cuneiform and Proximal Phalangeal Osteotomies in Hallux Valgus Surgery

Key Takeaway
Medial cuneiform and proximal phalangeal (Akin) osteotomies are powerful adjunctive procedures for correcting complex hallux valgus deformities. The medial cuneiform opening wedge osteotomy is particularly indicated in adolescents with open physes and severe metatarsus primus varus. Conversely, the Akin closing wedge osteotomy effectively addresses hallux valgus interphalangeus and provides residual deformity correction. Both require meticulous preoperative radiographic planning, precise surgical execution, and rigid fixation to optimize biomechanical alignment and clinical outcomes.
INTRODUCTION TO ADJUNCTIVE FOREFOOT OSTEOTOMIES
The surgical management of hallux valgus is highly nuanced, requiring a tailored approach that addresses the specific anatomical apex of the deformity. While distal, diaphyseal, and proximal metatarsal osteotomies form the cornerstone of bunion correction, certain complex presentations necessitate adjunctive procedures. The medial cuneiform opening wedge osteotomy and the proximal phalangeal closing wedge (Akin) osteotomy serve as critical tools in the orthopedic surgeon’s armamentarium.
The medial cuneiform osteotomy is uniquely positioned to address severe metatarsus primus varus in the skeletally immature patient, avoiding the catastrophic complication of physeal arrest associated with proximal metatarsal osteotomies. Conversely, the Akin osteotomy is a powerful adjunctive procedure utilized to correct hallux valgus interphalangeus or to fine-tune residual valgus alignment following a primary first ray correction. This comprehensive guide details the biomechanics, indications, preoperative planning, and step-by-step surgical execution of both procedures.
MEDIAL CUNEIFORM OSTEOTOMY
Historical Context and Biomechanics
First described by Riedel in 1996, the medial cuneiform osteotomy was originally conceptualized for the correction of isolated primus varus. Over time, its application has evolved. Today, it is predominantly utilized to treat severe hallux valgus deformities in adolescent patients who present with an abnormally wide intermetatarsal angle (IMA) but possess open proximal metatarsal physes.
Biomechanically, the first tarsometatarsal (TMT) joint and the medial cuneiform dictate the spatial orientation of the first ray. An opening wedge osteotomy of the medial cuneiform effectively plantarflexes and adducts the first metatarsal, reducing the IMA without violating the proximal metatarsal physis. This osteotomy is routinely combined with the removal of the medial eminence and imbrication of the medial capsule to achieve a comprehensive soft-tissue and bony correction.
Clinical Pearl: Performing a proximal metatarsal osteotomy in an adolescent with an open physis carries a high risk of premature physeal closure, leading to a shortened first ray and subsequent transfer metatarsalgia. The medial cuneiform osteotomy safely bypasses this risk while providing powerful correction at the apex of the deformity.
Indications and Patient Selection
Patient selection is paramount for the success of the medial cuneiform osteotomy. The primary indications include:
* Adolescent Hallux Valgus: Specifically, patients with open proximal metatarsal physes.
* Severe Metatarsus Primus Varus: Patients exhibiting an abnormally wide intermetatarsal angle (typically >15 degrees).
* Hypermobility of the First Ray: When combined with a Lapidus-type fusion, though the isolated cuneiform osteotomy preserves TMT joint motion.
* Revision Surgery: In cases where previous distal osteotomies have failed to correct a severe proximal deformity.
Preoperative Planning and Imaging
Standard weight-bearing anteroposterior (AP), lateral, and sesamoid axial radiographs are mandatory. The surgeon must carefully evaluate the IMA, the hallux valgus angle (HVA), and the status of the proximal metatarsal physis.

Anteroposterior projection of the medial cuneiform osteotomy before distraction, illustrating the planned osteotomy line.

Lateral view of the cuneiform osteotomy, demonstrating the trajectory required to avoid joint penetration.
Surgical Technique: Medial Cuneiform Opening Wedge Osteotomy
The procedure is typically performed under regional anesthesia (popliteal block) with a calf or thigh tourniquet.
Step 1: Surgical Approach
* Center a 3 to 4 cm medial longitudinal incision directly over the first cuneiform.
* Carefully dissect through the subcutaneous tissues, protecting the medial dorsal cutaneous nerve.
* The medial cuneiform is approximately 2 cm long. Identify the naviculocuneiform (NC) joint proximally and the metatarsocuneiform (MTC) joint distally using fluoroscopy or by inserting surgical needles into the joint spaces.
Step 2: The Osteotomy
* The osteotomy must be perfectly centered in the middle of the medial cuneiform to avoid violating the adjacent articular surfaces.
* Using an oscillating microsaw, direct the osteotomy in a mediolateral plane.
* Carry the saw blade to a depth of approximately 1.5 cm.
* Surgical Warning: It is critical to ensure that both the dorsal and the plantar cortices are completely transected to allow for symmetric opening of the wedge. Failure to release the plantar cortex will result in dorsal opening only, inadvertently elevating the first ray and causing postoperative transfer metatarsalgia.
Step 3: Graft Preparation and Insertion
* Distract the osteotomy site gently using a small lamina spreader.
* The medial eminence of the metatarsal head (resected during the bunionectomy phase) can be utilized as an interposition autograft. However, in adolescents, the medial eminence is often insufficient in volume.
* In such cases, harvest a wedge-shaped piece of tricortical bone from the ipsilateral iliac crest, or utilize a lyophilized, freeze-dried iliac bicortical allograft.
* Graft Dimensions: Because of the height of the first cuneiform, a 3-cm-long graft is typically required. The base of the graft should measure 1 cm or less, tapering to a fine point at the apex. All cortical bone on the interfacing surfaces of the graft should be removed or aggressively fenestrated to promote rapid osteointegration.
* Impact the bone graft securely into the distracted osteotomy site.

Osteotomy site distracted with a lamina spreader, and the wedge bone graft impacted into position.
Step 4: Fixation and Closure
* Fix the osteotomy and the impacted graft using crossed 0.062-inch Kirschner wires. Alternatively, a 3.5-mm or 4.5-mm fully threaded cortical or cancellous screw can be utilized for more rigid compression.
* Perform a layered closure, ensuring meticulous repair of the medial capsule if imbrication was performed simultaneously.
Postoperative Protocol
The incorporation of a structural graft in the midfoot requires strict adherence to postoperative offloading.
* Weeks 0-6: The patient is placed in a short-leg, well-padded, strictly non-weight-bearing cast.
* Weeks 6-12: Transition to a removable controlled ankle motion (CAM) walking boot. Progressive weight-bearing is initiated based on radiographic evidence of callus formation.
* Long-term: Full incorporation of both ends of the graft may take 4 to 6 months. High-impact activities are restricted until trabecular bridging is completely visible on radiographs.
PROXIMAL PHALANGEAL (AKIN) OSTEOTOMY
Historical Context and Biomechanics
In 1925, Truslow popularized the term metatarsus primus varus and advocated for its correction in hallux valgus surgery. That same year, Akin introduced a medially based closing wedge osteotomy at the base of the proximal phalanx, combined with the excision of the medial eminence. Akin also recommended the removal of the medial condylar flare at the base of the proximal phalanx.
Today, the Akin procedure is rarely indicated as an isolated, primary operation for hallux valgus. Instead, it has proven exceptionally valuable as an adjunctive procedure to a primary first metatarsal osteotomy or Lapidus fusion. Its primary biomechanical function is to correct hallux valgus interphalangeus (HVI) or to provide an additional 5 to 10 degrees of clinical valgus correction when the primary metatarsal procedure falls short of perfect clinical alignment.
Radiographic Evaluation and Decision Making
The degree of deformity must be meticulously measured on weight-bearing AP radiographs. The surgeon must evaluate the intermetatarsal angle (IMA), the metatarsophalangeal (MTP) angle, and the interphalangeal (IP) joint angle.
Pitfall: Persistent lateral displacement of the sesamoids after the completion of a primary bunion procedure strongly predisposes the patient to recurrence. The Akin procedure is of highly limited value—and generally contraindicated—if the sesamoid apparatus remains subluxed. It cannot compensate for an uncorrected IMA or a laterally translated metatarsal head.
Measuring the Phalangeal Articular Angle (PAA):
The PAA and the degree of hallux valgus interphalangeus are determined by drawing lines parallel to the proximal and distal articular surfaces of the proximal phalanx. A perpendicular line is then drawn to assess the angular deviation.

Measurement of the phalangeal articular angle (PAA) to assess the baseline severity of hallux valgus interphalangeus.

Postoperative measurement demonstrating the amount of angular correction achieved following the Akin closing wedge osteotomy.
Correction Ratio:
As a general surgical rule, an Akin osteotomy corrects approximately 8 degrees of clinical valgus for every 2.5 to 3.0 mm of medially based bone wedge removed at the base of the proximal phalanx.
Distal Metatarsal Articular Angle (DMAA):
Measurement of the DMAA is highly recommended when considering an Akin osteotomy. If the DMAA is greater than 10 to 15 degrees, and a basilar metatarsal osteotomy has already been utilized to correct an excessive IMA, the Akin procedure can safely gain additional valgus correction of the hallux without disrupting the congruity of the MTP joint.
Indications and Patient Profile
While originally described without an adductor tenotomy or lateral capsulotomy, combining the Akin with a lateral release is highly attractive for elderly patients whose primary goal is the prevention of impingement between the hallux and the second toe.
Patient Profile for an Isolated Akin Procedure:
1. Patient older than 55 years with lower functional demands.
2. Excessive hallux valgus interphalangeus (applicable in patients of any age).
3. Mild hallux valgus (HVA of no more than 25 degrees).
4. Normal intermetatarsal angle (IMA of less than 13 degrees).
5. Excellent MTP joint motion without localized intra-articular pain.
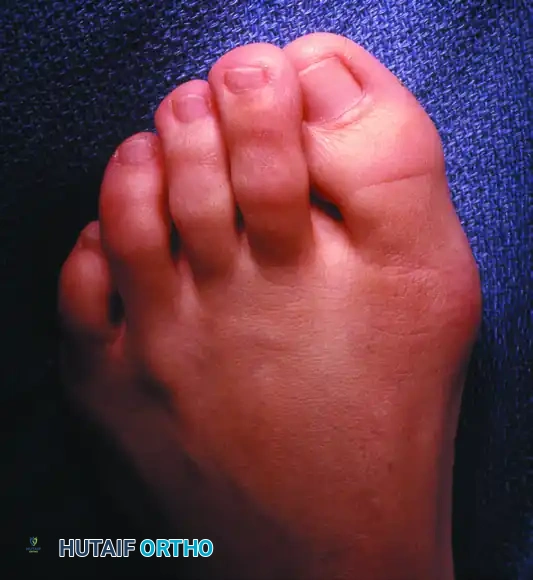
Clinical presentation of mild hallux valgus combined with significant hallux valgus interphalangeus. This specific deformity profile is highly appropriate for correction with an Akin osteotomy.
Contraindications
The Akin osteotomy is strictly contraindicated in the following scenarios:
1. Rheumatoid Arthritis: Due to poor bone quality and the progressive, destructive nature of the disease at the MTP joint.
2. Moderate-to-Severe Osteoarthritis: Degenerative changes at the MTP joint will not be addressed by a phalangeal osteotomy and may be exacerbated by altered joint mechanics.
3. Severe Metatarsus Primus Varus: An IMA greater than 13 degrees requires a metatarsal-based correction.
4. Severe Hallux Valgus: An HVA greater than 30 degrees cannot be adequately corrected by an Akin alone.
5. Sesamoid Subluxation: Lateral subluxation of the tibial sesamoid greater than 50% of its width indicates uncorrected proximal pathology.
6. Open Physis: An open physis at the base of the proximal phalanx is an absolute contraindication for a basilar Akin.
Clinical Pearl: If an adolescent with an open proximal phalangeal physis requires correction for severe hallux valgus interphalangeus, the osteotomy must be translated distally to the neck of the phalanx to avoid growth arrest.
Clinical presentation of a severe hallux valgus deformity with significant metatarsus primus varus and overriding toes. This deformity is entirely inappropriate for an isolated Akin osteotomy and requires comprehensive first ray reconstruction.
Surgical Technique: Akin Closing Wedge Osteotomy
Step 1: Approach and Exposure
* Utilize a medial longitudinal incision over the proximal phalanx, often an extension of the primary bunionectomy incision.
* Reflect the periosteum minimally to expose the metaphyseal-diaphyseal junction of the proximal phalanx. Excessive periosteal stripping can compromise the vascular supply and lead to delayed union.
Step 2: The Osteotomy
* The osteotomy is typically performed 5 to 10 mm distal to the MTP joint line to ensure the basilar articular surface and capsular attachments remain undisturbed.
* Using a microsaw, make the first cut perpendicular to the longitudinal axis of the phalanx.
* Make the second cut obliquely to create a medially based wedge. The size of the wedge (usually 2-4 mm) is dictated by the preoperative templating (remembering the 8 degrees per 3 mm rule).
* Crucial Step: The lateral cortex must be preserved intact to act as a tension-band hinge. If the lateral cortex is inadvertently breached, the construct loses its inherent stability, and more robust fixation (such as a plate) will be required.
Step 3: Closure and Fixation
* Gently close the osteotomy site by applying a varus force to the distal phalanx, compressing the medial wedge.
* Fixation can be achieved using a variety of implants based on surgeon preference and bone quality. Options include:
* A single oblique 0.062-inch K-wire.
* A memory-compression staple.
* A 2.0-mm or 2.4-mm headless compression screw.
* Heavy non-absorbable transosseous sutures (in cases of osteopenic bone).
Postoperative Protocol and Outcomes
The Akin procedure is highly effective when utilized correctly. It is often combined with adductor release, medial eminence removal, and medial capsular imbrication in elderly patients with moderate deformities.
- Weight-Bearing: Because the Akin is inherently stable (if the lateral hinge is preserved), patients can typically bear weight immediately in a rigid postoperative shoe or CAM boot.
- Bone Healing: Radiographic union is generally observed between 4 to 6 weeks.
- Patient Counseling: It is imperative to manage patient expectations. The surgeon must emphasize that while the hallux will fit into footwear much more comfortably and will no longer impinge upon the second toe, the cosmetic appearance of the toe itself (specifically the width of the IP joint) may not be appreciably changed.
By mastering both the medial cuneiform opening wedge and the Akin closing wedge osteotomies, the orthopedic surgeon is equipped to handle the full spectrum of complex, multi-apical hallux valgus deformities, ensuring optimal biomechanical restoration and superior patient outcomes.
