Mau Osteotomy: A Masterclass in Hallux Valgus Correction

Key Takeaway
This masterclass provides an exhaustive guide to the Mau osteotomy for hallux valgus correction. Fellows will learn intricate surgical anatomy, meticulous operative techniques, and critical decision-making. We cover patient positioning, precise osteotomy execution, fixation strategies, and comprehensive postoperative management, ensuring a deep understanding of this inherently stable and reproducible procedure for moderate to severe bunion deformities.
Comprehensive Introduction and Patho-Epidemiology
Etiology and Pathogenesis of Hallux Valgus
Hallux valgus is a complex, progressive deformity that represents far more than a simple osseous prominence. At its core, it is a static subluxation of the first metatarsophalangeal (MTP) joint, characterized by the medial deviation of the first metatarsal and the lateral, or valgus, rotation of the hallux. This geometric derangement invariably presents with a prominent medial or dorsomedial eminence, colloquially referred to as a "bunion." As orthopedic surgeons, we must recognize that the visible eminence is merely the clinical manifestation of a profound underlying biomechanical failure of the first ray. The exact genesis of hallux valgus remains a subject of ongoing biomechanical debate, but it is almost exclusively observed in shod populations, implicating constrictive footwear as a primary extrinsic catalyst.
However, the pathogenesis is multifactorial, with intrinsic anatomical and genetic factors playing an equally critical role. A strong hereditary predisposition is frequently observed, often following an autosomal dominant transmission pattern with incomplete penetrance. Patients with a family history typically present at a younger age with more rapid progression. Furthermore, biomechanical anomalies such as pes planus (flatfoot) significantly contribute to the deformity. The collapse of the medial longitudinal arch leads to excessive pronation of the midfoot during the stance phase of gait, which in turn unlocks the transverse tarsal joint, hypermobilizes the first ray, and alters the ground reaction forces acting on the first metatarsal head, driving it medially.
Metatarsus primus varus, defined as an abnormally increased intermetatarsal angle between the first and second rays, is both a precursor to and a consequence of hallux valgus. Systemic inflammatory conditions, such as rheumatoid arthritis, osteoarthritis, and crystalline arthropathies like gout, can severely compromise the capsuloligamentous integrity of the MTP joint, predisposing it to rapid subluxation. Additionally, neuromuscular disorders that induce spasticity or flaccidity can disrupt the delicate balance of the intrinsic musculature, leading to relentless progressive deformity. Anatomical variations, including an excessively convex metatarsal head or abnormal obliquity of the first metatarsocuneiform (TMT) joint, further exacerbate the mechanical instability of the medial column.
Natural History and Deforming Forces
The natural history of hallux valgus is typically characterized by a gradual, insidious progression, though the rate of deterioration can accelerate exponentially when multiple causative factors converge. The intrinsic and extrinsic musculature of the foot play a definitive role in this pathological cascade. Under normal physiological conditions, the abductor hallucis muscle plantarflexes, adducts, and inverts the proximal phalanx, while the adductor hallucis plantarflexes, abducts, and everts it. When balanced, these forces neutralize transverse and frontal plane moments, producing a stable, straight plantarflexion force during toe-off.
In the setting of hallux valgus, this delicate equilibrium is catastrophically lost. As the first metatarsal drifts medially, the adductor hallucis gains a distinct mechanical advantage. This imbalance is often exacerbated by iatrogenic factors, such as the overzealous resection of the tibial sesamoid during previous surgeries, or by the chronic stretching of the medial capsular structures due to excessive foot pronation. The sesamoid apparatus, tethered by the transverse intermetatarsal ligament, remains relatively stationary relative to the second metatarsal, meaning the first metatarsal head effectively subluxates medially off its own sesamoids. This abnormal articulation erodes the crista, the cartilaginous ridge separating the sesamoid grooves.
As the deformity advances, the abductor hallucis muscle progressively slides plantarly beneath the metatarsal head, losing its abductory vector and instead contributing to the pronation of the hallux. Once the proximal phalanx deviates laterally, the powerful extrinsic tendons—the extensor hallucis longus (EHL) and flexor hallucis longus (FHL)—shift laterally to the mechanical axis of the MTP joint. They effectively become dynamic bowstrings, relentlessly driving the hallux further into valgus and the metatarsal further into varus with every step. Ultimately, the hallux may override or underlap the second digit, precipitating crossover toe deformities, second MTP joint dislocation, and debilitating transfer metatarsalgia beneath the lesser metatarsal heads.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Configuration
A profound understanding of the complex functional anatomy of the first ray is paramount before undertaking a powerful diaphyseal correction like the Mau osteotomy. The first MTP joint is functionally bipartite. The primary articulation is a shallow ball-and-socket joint between the convex first metatarsal head and the concave base of the proximal phalanx. The secondary, yet equally vital, articulation comprises the dual grooves on the plantar aspect of the first metatarsal head that articulate with the dorsal chondral surfaces of the tibial and fibular sesamoids. These two functional joints share a common, continuous synovial capsule.
The sesamoid apparatus is integral to the biomechanical efficiency of the first ray. The medial (tibial) and lateral (fibular) sesamoids are embedded within the medial and lateral slips of the flexor hallucis brevis (FHB) tendon, respectively. They are separated by the crista, which acts as a tracking guide during sagittal plane motion. The intersesamoidal ligament firmly connects the two ossicles, while the lateral sesamoid is robustly tethered to the plantar plate of the second metatarsal head via the deep transverse intermetatarsal ligament. These sesamoids serve a dual purpose: they act as a dynamic fulcrum to increase the mechanical advantage of the FHB, and they elevate the metatarsal head to protect the FHL tendon as it glides through the intersesamoidal groove during the propulsive phase of gait.
When executing a Mau osteotomy, the surgeon must be acutely aware of the diaphyseal geometry of the first metatarsal. The bone is not a simple cylinder; it possesses a distinct dorsal concavity and a plantar convexity, with a complex cross-sectional anatomy that transitions from a triangular base proximally to a more cylindrical shape distally. The Mau osteotomy—a proximal-dorsal to distal-plantar oblique cut—capitalizes on this geometry to create an inherently stable construct under axial loading, distinguishing it from other diaphyseal osteotomies.
Ligamentous and Musculotendinous Stabilizers
The static stability of the first MTP joint relies heavily on the collateral ligament complex. These fan-shaped ligaments originate from the medial and lateral epicondyles of the first metatarsal head. They bifurcate into the metatarsophalangeal (proper collateral) ligaments, which insert into the base of the proximal phalanx, and the metatarsosesamoid (accessory collateral) ligaments, which insert into the plantar plate and sesamoids. These vertical, horizontal, and oblique fibers provide critical multiplanar stability, resisting abnormal valgus, varus, and rotational forces.
The musculotendinous structures dictate the dynamic stability of the joint. The intrinsic muscles include the abductor hallucis, which inserts plantar-medially on the proximal phalanx and blends with the medial head of the FHB to invest the tibial sesamoid. The adductor hallucis, comprising an oblique and a transverse head, inserts plantar-laterally on the proximal phalanx, blending with the lateral head of the FHB to invest the fibular sesamoid. The FHB itself encapsulates the sesamoids and inserts into the proximal phalanx, playing a crucial role in plantarflexion.
The extrinsic muscles, the FHL and EHL, are powerful motors for the hallux. The FHL traverses the plantar groove between the sesamoids to insert on the distal phalanx. The EHL runs dorsally, tethered over the MTP joint by the extensor sling, which anchors it to the plantar plate and sesamoids. During a Mau osteotomy and the associated lateral soft tissue release, the surgeon must carefully navigate these structures, specifically targeting the contracted lateral structures (adductor hallucis and lateral capsuloligamentous complex) while preserving the dynamic stabilizers necessary for post-operative function.
Neurovascular Considerations
Iatrogenic neurovascular injury is a devastating complication that can compromise the entire reconstructive effort. The medial dorsal cutaneous nerve, a terminal branch of the superficial fibular nerve, courses dorsally and medially over the first metatarsal. The surgical incision must be meticulously planned to avoid direct transection or aggressive retraction of this nerve, which can result in intractable neuritic pain or neuroma formation. Similarly, the plantar cutaneous branches of the medial plantar nerve must be protected during plantar dissection.
The vascular anatomy demands absolute respect, particularly when performing diaphyseal osteotomies combined with distal soft tissue releases. The first dorsal metatarsal artery runs dorsally through the first web space, often in close proximity to the medial dorsal cutaneous nerve. However, the most critical vascular structure is the principal nutrient artery to the first metatarsal head. This vessel typically arises from the first plantar metatarsal artery and enters the metatarsal head at the lateral plantar aspect of the surgical neck.
When performing a medial eminence resection and a lateral release simultaneously, the blood supply to the capital fragment is rendered highly tenuous. It is absolutely critical to preserve the plantar periosteum and the soft tissue attachments on the plantar-lateral aspect of the metatarsal neck. Aggressive stripping of the capsule or disruption of this vascular leash during the execution of the Mau osteotomy can reliably precipitate avascular necrosis (AVN) of the metatarsal head, a catastrophic complication leading to joint collapse and severe arthrosis.
Exhaustive Indications and Contraindications
Patient Selection Criteria
The Mau osteotomy is a highly versatile and powerful technique, but it is not a panacea for all hallux valgus deformities. It is primarily indicated for moderate to severe hallux valgus deformities, typically characterized by an intermetatarsal (IM) angle between 13 and 20 degrees, and a hallux valgus angle (HVA) exceeding 30 degrees. Unlike distal chevron osteotomies, which are limited in their corrective potential by the width of the metatarsal head, the diaphyseal nature of the Mau allows for significant lateral translation and angular correction of the capital fragment.
Furthermore, the Mau osteotomy is an excellent choice for patients requiring simultaneous correction of a sagittal plane deformity. By altering the angle of the osteotomy cut relative to the longitudinal axis of the metatarsal, the surgeon can intentionally plantarflex or dorsiflex the distal fragment. This is particularly useful in patients with a concomitant elevatus of the first ray or those at high risk for postoperative transfer metatarsalgia. The inherent biomechanical stability of the Mau cut—where ground reaction forces actively compress the osteotomy site—makes it highly suitable for heavier patients or those in whom prolonged non-weight-bearing is undesirable.
Patient compliance is an equally critical selection criterion. While the Mau osteotomy is structurally robust, the success of the procedure relies heavily on the patient's adherence to postoperative weight-bearing restrictions and rehabilitation protocols. The ideal candidate is a physiologically optimized adult with realistic expectations regarding postoperative shoe wear and activity modifications, who experiences daily pain that is refractory to conservative measures such as shoe modification, orthotics, and non-steroidal anti-inflammatory drugs.
Absolute and Relative Contraindications
Despite its power, the Mau osteotomy is contraindicated in several distinct clinical scenarios. Recognizing these contraindications is essential to prevent intraoperative disasters and postoperative failures. The presence of significant degenerative joint disease (osteoarthritis) of the first MTP joint is an absolute contraindication; realigning an arthritic joint will not relieve pain and may exacerbate stiffness. In such cases, an MTP joint arthrodesis is the gold standard.
Hypermobility of the first tarsometatarsal (TMT) joint is a critical relative, if not absolute, contraindication. If a diaphyseal osteotomy is performed in the presence of profound TMT instability, the deformity is highly likely to recur as the medial column continues to splay under load. For these patients, a Lapidus procedure (first TMT arthrodesis) is the biomechanically appropriate choice. Additionally, an excessively narrow first metatarsal diaphysis precludes the use of a Mau osteotomy, as there will be insufficient bone stock to allow for adequate lateral translation and secure internal fixation, drastically increasing the risk of iatrogenic fracture or nonunion.
Active infection, severe peripheral vascular disease, and uncontrolled diabetes mellitus are absolute contraindications to any elective forefoot reconstruction. Furthermore, an abnormally high distal metatarsal articular angle (DMAA) must be carefully evaluated. While the Mau can be modified (e.g., a biplanar cut) to address a deviated articular surface, severe DMAA deformities are often better managed with a double osteotomy (e.g., proximal Mau combined with a distal Reverdin-Isham) to ensure a congruent joint postoperatively.
| Category | Mau Osteotomy Indications | Mau Osteotomy Contraindications |
|---|---|---|
| Deformity Severity | Moderate to Severe (IM Angle 13°-20°, HVA > 30°) | Mild Deformity (IM < 13°), Extreme Deformity (IM > 20°) |
| Joint Status | Congruent or Deviated, without severe arthrosis | Severe Osteoarthritis (Rigidus), Rheumatoid joint destruction |
| Biomechanical Factors | Stable 1st TMT joint, adequate bone stock | 1st TMT Hypermobility, excessively narrow metatarsal diaphysis |
| Vascular/Systemic | Intact pedal pulses, controlled comorbidities | Peripheral Arterial Disease, Active Infection, Uncontrolled Diabetes |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Vascular Assessment
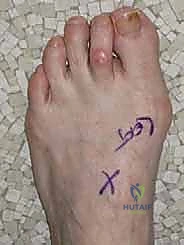
Meticulous preoperative planning forms the bedrock of a successful Mau osteotomy. The clinical evaluation must be exhaustive. The chief complaint usually centers on pain over the medial eminence, but the surgeon must also probe for pain over the dorsal MTP joint (suggesting impingement or early arthrosis), the sesamoids, or the lesser toes. A thorough history must screen for systemic conditions, and a realistic discussion regarding postoperative expectations—specifically that the goal is pain relief and functional restoration, not necessarily the ability to wear narrow, high-heeled fashion footwear—must be documented.
The physical examination begins with a weight-bearing assessment to evaluate the dynamic nature of the bunion, arch collapse, and lesser toe deformities. Vascular status is paramount; the posterior tibial and dorsalis pedis arteries must be palpable. If capillary refill is delayed or pulses are diminished, non-invasive vascular studies (Ankle-Brachial Index, transcutaneous oximetry) are mandatory before proceeding. Range of motion (ROM) of the first MTP joint must be assessed with the hallux held in the corrected position to accurately gauge soft tissue contractures. Normal dorsiflexion is 70 to 90 degrees.
Crucially, the surgeon must evaluate the transverse plane mobility of the first ray and the excursion of the first TMT joint. By stabilizing the midfoot and translating the first metatarsal head dorsally and plantarly, the surgeon can assess for hypermobility. Excursion greater than 15 mm strongly suggests TMT instability, which might warrant a Lapidus procedure instead of a Mau. Finally, the plantar forefoot must be inspected for intractable plantar keratomas (IPKs), particularly beneath the second metatarsal head, which indicates transfer loading and necessitates careful sagittal plane planning of the osteotomy to prevent worsening the metatarsalgia.
Radiographic Analysis and Deformity Quantification
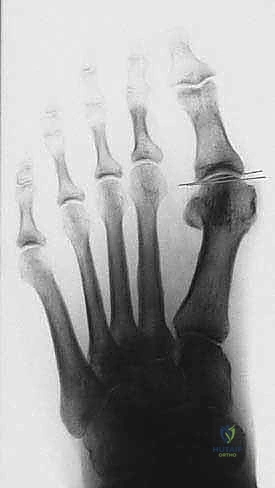
Standardized, weight-bearing radiographs are indispensable. Non-weight-bearing films are virtually useless for planning bunion surgery as they vastly underestimate the splay of the forefoot. The AP, lateral, and oblique views must be systematically analyzed.

The Intermetatarsal 1-2 (IM1-2) Angle is calculated by bisecting the longitudinal axes of the first and second metatarsals. An angle greater than 9 degrees is abnormal, and the Mau is typically reserved for angles between 13 and 20 degrees.

The Hallux Valgus Angle (HVA), formed by the bisection of the first metatarsal and the proximal phalanx, quantifies the lateral drift of the toe. Normal is less than 15 degrees.

The Tibial Sesamoid Position is graded (1 to 7) based on its relationship to the bisection of the first metatarsal. A laterally subluxated sesamoid (grades 4-7) indicates significant coronal plane rotation of the metatarsal and severe soft tissue contracture, necessitating a thorough lateral release.

The Distal Metatarsal Articular Angle (DMAA) evaluates the orientation of the articular cartilage. If the DMAA is significantly increased (greater than 10-15 degrees), translating the metatarsal head laterally with a standard Mau will result in a laterally facing articular surface, leading to a severe, iatrogenic hallux valgus recurrence. In such cases, a derotational component must be added to the osteotomy. Preoperative digital templating is highly recommended to determine the exact starting point, angle, and required translation of the osteotomy to achieve the desired IM angle reduction without shortening the ray excessively.
Anesthesia, Positioning, and Tourniquet Application
The procedure is typically performed under regional anesthesia (e.g., a popliteal sciatic nerve block combined with a saphenous nerve block) or general anesthesia, depending on patient preference and comorbidities. A regional block provides excellent intraoperative muscle relaxation and profound postoperative analgesia, significantly reducing the need for systemic opioids.
The patient is positioned supine on the operating table. A bump may be placed under the ipsilateral hip to internally rotate the leg, bringing the medial aspect of the foot directly facing the surgeon, which vastly improves ergonomics during the medial approach and osteotomy execution. The foot is prepped and draped in a standard sterile fashion up to the mid-calf.
Hemostasis is critical for visualizing the complex anatomical planes and protecting the neurovascular structures. An ankle tourniquet or a calf tourniquet is applied over generous padding. The limb is exsanguinated using an Esmarch bandage, and the tourniquet is inflated to approximately 250 mmHg. The surgeon must be mindful of tourniquet time, aiming to complete the procedure and release the tourniquet within 90 to 120 minutes to minimize the risk of ischemic nerve injury or deep vein thrombosis.
Step-by-Step Surgical Approach and Fixation Technique
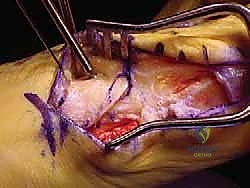
Incision, Dissection, and Lateral Release
The operation commences with a meticulously planned dorsal-medial or direct medial incision. A dorsal-medial approach, approximately 6 to 8 cm in length, is often preferred as it allows access to both the medial eminence and the first web space for the lateral release. The incision is deepened through the subcutaneous tissue, taking extreme care to identify and retract the medial dorsal cutaneous nerve and the dorsal venous arch.
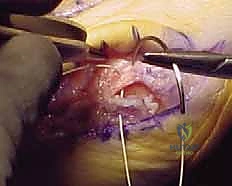
Once the extensor hallucis longus (EHL) is identified and retracted laterally, the first web space is entered to perform the lateral release. This step is non-negotiable in severe deformities. The deep transverse intermetatarsal ligament is identified and transected, releasing the tether between the first and second rays. The adductor hallucis tendon is identified at its insertion on the base of the proximal phalanx and the fibular sesamoid, and is carefully released.

Attention is then directed to the medial aspect of the joint. A longitudinal or inverted-L capsulotomy is performed. The medial eminence is exposed by sharply elevating the capsule, preserving the plantar-medial periosteum to protect the vascular supply.
The medial eminence (the "bunion") is resected using an oscillating saw. The cut should be made parallel to the medial border of the foot, preserving the sagittal groove for the tibial sesamoid. Over-resection must be strictly avoided, as it can compromise the tibial sesamoid articulation and lead to postoperative hallux varus.
Execution of the Mau Osteotomy
The defining feature of the Mau osteotomy is its geometric orientation. Unlike the Ludloff osteotomy (which runs dorsal-distal to plantar-proximal), the Mau osteotomy is initiated dorsally at the proximal metaphysis and directed plantarly toward the distal metaphysis.
Using a sagittal saw, the cut begins approximately 1.5 to 2 cm distal to the first TMT joint on the dorsal cortex. The blade is directed distally and plantarly, aiming to exit the plantar cortex just proximal to the metatarsal neck and the sesamoid apparatus.

The angle of this cut is critical. In the sagittal plane, a steeper angle allows for greater lateral translation but less structural stability, while a shallower angle provides a massive surface area for healing but limits translation.

Furthermore, the surgeon can manipulate the saw blade in the frontal plane to address DMAA or to intentionally plantarflex the metatarsal head. If the blade is tilted slightly plantarly, lateral translation will simultaneously result in plantarflexion of the capital fragment, a highly desirable outcome to prevent transfer metatarsalgia.

During the osteotomy, continuous saline irrigation is mandatory to prevent thermal necrosis of the bone, which could precipitate nonunion.
Deformity Correction and Rigid Internal Fixation
Once the osteotomy is complete, the crucial step of deformity correction begins. The distal fragment is translated laterally along the plane of the osteotomy cut.

Because of the proximal-dorsal to distal-plantar orientation, ground reaction forces during weight-bearing will actually push the distal fragment proximally and dorsally, firmly compressing the osteotomy surfaces together. This inherent biomechanical stability is the hallmark of the Mau procedure.
The capital fragment is translated laterally until the intermetatarsal angle is clinically reduced to near zero. A bone clamp (e.g., a point-to-point reduction clamp) is applied to provisionally hold the reduction.

At this stage, fluoroscopy must be utilized to confirm the reduction of the IM angle, the restoration of the sesamoid station (the tibial sesamoid should sit squarely beneath the metatarsal head), and the alignment of the MTP joint.

Rigid internal fixation is typically achieved using two or three cortical lag screws (typically 2.7 mm or 3.0 mm). The first screw is placed perpendicular to the osteotomy plane to provide interfragmentary compression.

A second, and optionally a third, screw is placed to resist rotational forces. The screw heads must be carefully countersunk to prevent dorsal cortical stress risers and to minimize hardware prominence, which can irritate extensor tendons or footwear.

Following secure fixation, the medial overhanging bone shelf on the proximal fragment is resected flush with the translated distal fragment.

The medial capsule is then meticulously plicated to correct the valgus rotation of the hallux and restore tension to the medial collateral ligaments.

The skin is closed in layers, and a robust, compressive dressing is applied to hold the hallux in a neutral to slightly plantarflexed and adducted position.
Complications, Incidence Rates, and Salvage Management
Intraoperative Complications
Despite meticulous technique, intraoperative complications can occur and must be managed decisively. Iatrogenic fracture of the metatarsal, either the dorsal proximal cortex or the plantar distal hinge, is a significant risk. This often results from an excessively steep osteotomy cut, a narrow diaphysis, or
Clinical & Radiographic Imaging Archive