Master ABOS Orthopedic Board Review: Pediatric Infections, Tumors, & Skeletal Dysplasias | Part 6
20 Jun 2026
51 min read
24 Views
Key Takeaway
ABOS Pediatric Orthopedics Review Part 6 covers key topics in pediatric orthopedic pathology. It includes newborn septic coxitis, osteomyelitis, benign bone tumors like osteoblastoma, and a wide range of skeletal dysplasias such as achondroplasia, SED, and Morquio syndrome, focusing on their diagnosis, clinical features, and management strategies.
Master ABOS Orthopedic Board Review: Pediatric Infections, Tumors, & Skeletal Dysplasias | Part 6
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 16-year-old boy presents with back pain. Radiographs reveal an expansile lesion in the spine as shown.
Which of the following is the most likely location of this tumor?
Which of the following is the most likely location of this tumor?
Explanation
Osteoblastomas of the spine classically arise in the posterior elements. They are typically expansile and can cause painful scoliosis, requiring surgical excision for definitive treatment.
Question 2
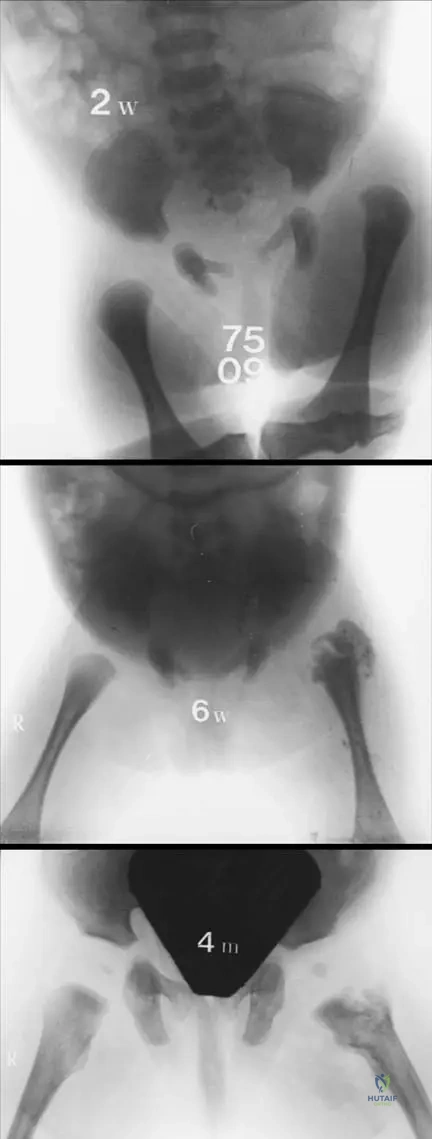
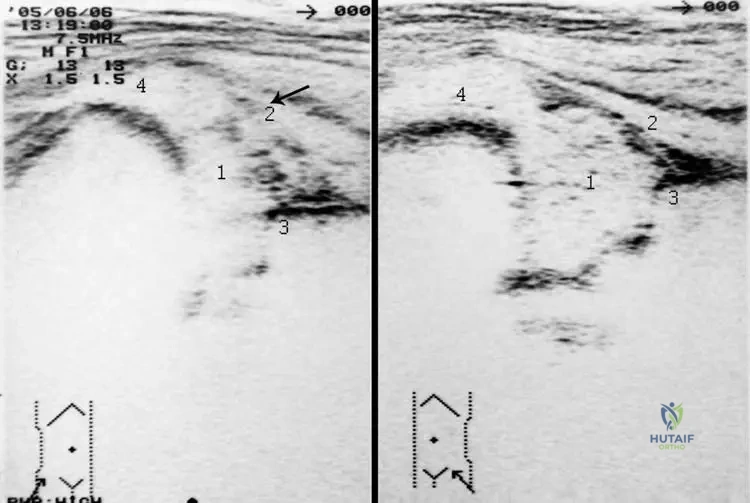
A 2-week-old neonate presents with pseudoparalysis of the right leg and irritability with diaper changes. Ultrasound shows a hip effusion and radiographs reveal subtle changes as shown.
Besides Staphylococcus aureus, which organism is a leading cause of septic arthritis in this age group?
Besides Staphylococcus aureus, which organism is a leading cause of septic arthritis in this age group?
Explanation
Group B Streptococcus and Staphylococcus aureus are the most common pathogens responsible for neonatal septic arthritis. Neonates often lack systemic signs like fever, presenting instead with pseudoparalysis.
Question 3
A 3-year-old boy is diagnosed with Kingella kingae septic arthritis of the knee. What is the most effective method for isolating this fastidious organism from synovial fluid?
Explanation
Kingella kingae is a fastidious, Gram-negative organism that is difficult to culture on standard solid media. Inoculating the synovial fluid directly into aerobic blood culture vials (BACTEC) significantly increases the diagnostic yield.
Question 4
A 14-year-old girl undergoes curettage of a 3.5 cm lytic bone lesion in the distal femur. The histology is shown.
Microscopy reveals loose fibrovascular connective tissue intermixed with irregular osteoid without atypical mitoses. Her pain was poorly relieved by NSAIDs. What is the diagnosis?
Microscopy reveals loose fibrovascular connective tissue intermixed with irregular osteoid without atypical mitoses. Her pain was poorly relieved by NSAIDs. What is the diagnosis?
Explanation
The size greater than 2 cm, incomplete response to NSAIDs, and classic histology of loose fibrovascular stroma with irregular osteoid distinguish osteoblastoma from osteoid osteoma. Atypical mitoses and permeative growth into normal bone are absent, differentiating it from osteosarcoma.
Question 5
Which of the following gene mutations is responsible for Achondroplasia, resulting in a gain-of-function that inhibits chondrocyte proliferation at the physis?
Explanation
Achondroplasia is caused by an activating (gain-of-function) mutation in the FGFR3 gene. This mutation over-inhibits chondrocyte proliferation in the proliferative zone of the growth plate, leading to rhizomelic dwarfism.
Question 6
A 7-year-old boy presents with fever, swelling, and pain in the midshaft of his femur. Radiographs show a permeative diaphyseal lesion with an onion-skin periosteal reaction. Cytogenetics reveal a t(11;22) translocation. Which fusion gene is associated with this condition?
Explanation
Ewing sarcoma is classically characterized by the t(11;22) chromosomal translocation. This translocation results in the EWS-FLI1 fusion protein, which acts as an aberrant transcription factor.
Question 7
A 6-year-old girl with severe short stature, genu valgum, and corneal clouding is evaluated. Radiographs reveal universal platyspondyly and hypoplasia of the odontoid. A urine test is positive for keratan sulfate. What is the most critical orthopedic concern prior to any surgical intervention involving general anesthesia?
Explanation
The patient has Morquio syndrome (Mucopolysaccharidosis Type IV), diagnosed by urinary keratan sulfate. Odontoid hypoplasia leads to severe atlantoaxial instability, necessitating meticulous cervical spine evaluation before intubation or general anesthesia.
Question 8
A 13-year-old boy presents with chronic knee pain. Radiographs show an eccentrically located, lytic epiphyseal lesion in the proximal tibia with a sclerotic margin. Biopsy shows mononuclear cells and chicken-wire calcifications. What is the diagnosis?
Explanation
Chondroblastoma is a benign, locally aggressive bone tumor that classically occurs in the epiphysis of skeletally immature patients. Histology characteristically demonstrates chondroblasts, multinucleated giant cells, and fine, pericellular chicken-wire calcifications.
Question 9
A 2-year-old boy with a history of anterolateral tibial bowing develops a pseudoarthrosis after a minor fall. He has multiple cafe-au-lait spots. The underlying genetic mutation affects a protein primarily involved in which of the following cellular pathways?
Explanation
Neurofibromatosis type 1 (NF1) is caused by a mutation in the NF1 gene, which encodes neurofibromin. Neurofibromin acts as a Ras-GTPase activating protein (Ras-GAP) that normally downregulates Ras signaling; its loss leads to cellular overproliferation.
Question 10
A 14-year-old boy presents with chronic, dull back pain. He states the pain is constant and does not significantly improve with ibuprofen. Radiographs are shown.
Which of the following describes the most likely diagnosis?
Which of the following describes the most likely diagnosis?
Explanation
Osteoblastoma is a benign but locally aggressive bone tumor typically >2 cm. It favors the posterior elements of the spine and, unlike osteoid osteoma, pain is usually not dramatically relieved by NSAIDs.
Question 11
A 14-year-old boy presents with progressive back pain that is poorly responsive to NSAIDs. Neurological examination is normal. Radiographs are shown below.
Which of the following characteristics best differentiates this lesion from an osteoid osteoma?
Which of the following characteristics best differentiates this lesion from an osteoid osteoma?
Explanation
The clinical and radiographic presentation is consistent with an osteoblastoma, which is classically >2 cm, progressively enlarging, and does not predictably respond to NSAIDs. Osteoblastomas have a higher rate of local recurrence and can cause neurological deficit due to expansile growth. Both tumors prefer the posterior elements of the spine.
Question 12
A 16-year-old girl undergoes intralesional curettage of an expansile 3.5 cm lytic lesion located in the posterior elements of C4. A photomicrograph of the specimen is shown.
What is the most likely diagnosis?
What is the most likely diagnosis?
Explanation
The histology demonstrates loose fibrovascular connective tissue intermixed with irregular osteoid, typical of osteoblastoma. The lesion size (3.5 cm) rules out osteoid osteoma, which has identical histology but is <2 cm.
Question 13
A 2-week-old neonate presents with asymmetric hip creases, fever, and pseudoparalysis of the right lower extremity. Ultrasound confirms a large hip effusion, and emergent surgical drainage is performed. The clinical image below demonstrates severe sequelae of a missed diagnosis in a similar patient.
What is the most devastating long-term complication of delayed diagnosis of neonatal septic arthritis of the hip?
What is the most devastating long-term complication of delayed diagnosis of neonatal septic arthritis of the hip?
Explanation
Delay in treating neonatal septic arthritis of the hip results in catastrophic destruction of the cartilaginous femoral head and neck due to infection and increased intra-articular pressure compromising the vascular supply. This results in the classic Choi type IV sequelae (destruction of head and neck).
Question 14
A 14-month-old child presents with refusal to bear weight and a knee effusion. Fluid analysis shows a WBC count of 65,000 cells/microL with a negative Gram stain. The suspected organism is a fastidious Gram-negative rod that is part of the normal pediatric respiratory flora. Which method is most critical for isolating the likely causative organism?
Explanation
Kingella kingae is the most common cause of septic arthritis in children aged 6 months to 4 years. It is notoriously difficult to culture on standard solid media, and diagnostic yield significantly increases when joint fluid is inoculated into blood culture vials (BACTEC).
Question 15
A 4-year-old boy presents with rhizomelic short stature, frontal bossing, and a depressed nasal bridge. The genetic mutation underlying his condition primarily disrupts normal bone growth through which of the following cellular mechanisms?
Explanation
The patient has achondroplasia, caused by a gain-of-function mutation in the FGFR3 gene. This constitutive activation inhibits normal chondrocyte proliferation and hypertrophy in the physis, particularly affecting endochondral ossification.
Question 16
An 11-year-old boy presents with severe, deep thigh pain and fever. Radiographs show a permeative diaphyseal lesion with an "onion-skin" periosteal reaction. A core biopsy demonstrates uniform small round blue cells. Which specific genetic translocation is most diagnostic of this malignancy?
Explanation
Ewing sarcoma is characterized by the t(11;22) translocation, resulting in the EWS-FLI1 fusion protein in about 85% of cases. It classically presents as a permeative, diaphyseal lesion in children.
Question 17
A 5-year-old girl with an established diagnosis of Spondyloepiphyseal Dysplasia congenita (SEDc) presents for a routine orthopedic evaluation. Because of her condition, she is at highest risk for which of the following potentially life-threatening complications?
Explanation
SEDc is caused by a COL2A1 mutation and is characterized by a short trunk, coxa vara, myopia, and odontoid hypoplasia. Atlantoaxial instability is a major risk and requires careful screening, particularly before any procedure involving general anesthesia or intubation.
Question 18
A 6-year-old boy presents with short-trunk dwarfism, corneal clouding, and normal intelligence. Radiographs demonstrate severe platyspondyly and odontoid hypoplasia. Urine tests reveal elevated levels of keratan sulfate. This clinical picture is most consistent with a deficiency in which enzyme?
Explanation
The presentation is classic for Morquio syndrome (MPS Type IV), which features normal intelligence, severe skeletal dysplasia, odontoid hypoplasia, and keratan sulfate in the urine. It is caused by a deficiency in N-acetylgalactosamine-6-sulfatase (Type IVA).
Question 19
A 15-year-old boy presents with a rapidly expanding, destructive metaphyseal lesion of the distal femur. MRI reveals large fluid-fluid levels. Histology shows highly pleomorphic, atypical spindle cells producing fine, lace-like osteoid within the septa separating blood-filled spaces. What is the most likely diagnosis?
Explanation
While aneurysmal bone cysts (ABCs) feature fluid-fluid levels and blood-filled spaces, the presence of atypical, highly pleomorphic spindle cells and malignant osteoid production within the septa is diagnostic of telangiectatic osteosarcoma. This distinction is critical as treatment requires neoadjuvant chemotherapy and wide resection.
Question 20
A 7-year-old girl from Massachusetts presents with a massive, painless effusion of her right knee. She is afebrile and inflammatory markers are minimally elevated. Joint aspiration yields 45,000 WBCs/microL. After sending synovial fluid for testing, what is the recommended initial management for this likely diagnosis?
Explanation
This is a classic presentation of Lyme arthritis (large, relatively painless effusion, low-grade inflammatory markers in an endemic area). For children under 8 years of age, a 28-day course of oral amoxicillin is the standard treatment to avoid the tooth-staining side effects of doxycycline.
Question 21
A 9-year-old boy sustains a minimally displaced pathologic fracture through a central, entirely lytic lesion in the proximal humerus metaphysis. A "fallen leaf" sign is present. The lesion abuts the physis. What is the most appropriate management after the fracture has initially healed?
Explanation
The presentation and "fallen leaf" sign are classic for an active Unicameral Bone Cyst (UBC). Following fracture union, active UBCs near the physis are typically treated with less invasive methods such as aspiration and injection (steroids or bone marrow aspirate) to avoid physeal injury.
Question 22
A 15-year-old boy presents with progressive back pain that awakens him at night and is not relieved by ibuprofen. Imaging shows a 3-cm expansile lytic lesion in the posterior elements of L3. Biopsy reveals the following histology.
What is the most likely diagnosis?
What is the most likely diagnosis?
Explanation
Osteoblastoma is typically larger than 2 cm, occurs frequently in the posterior elements of the spine, and causes pain that is classically not relieved by NSAIDs. Histology shows loose fibrovascular connective tissue intermixed with irregular osteoid.
Question 23
A 10-day-old neonate presents with fever, irritability, and decreased spontaneous movement of the right lower extremity. On examination, the infant cries with passive range of motion of the right hip. An ultrasound reveals a significant joint effusion. What is the most appropriate next step in management?
Explanation
Neonatal septic arthritis of the hip (coxitis) is a surgical emergency requiring urgent joint aspiration and surgical drainage. Delaying surgical decompression can lead to rapid destruction of the cartilaginous femoral head and permanent joint damage.
Question 24
A newborn is noted to have severe short limb dwarfism, rigid bilateral clubfeet, abducted "hitchhiker" thumbs, and cystic swelling of the pinnae. Mutations in which of the following genes or proteins are responsible for this condition?
Explanation
The clinical presentation is classic for diastrophic dysplasia, which is caused by a mutation in the SLC26A2 gene coding for a diastrophic dysplasia sulfate transporter (DTDST). It is inherited in an autosomal recessive pattern.
Question 25
An 18-month-old child presents with a limp and low-grade fever. Hip aspiration yields purulent fluid with a normal Gram stain. Routine cultures are initially negative, but growth is eventually achieved using aerobic blood culture vials (BACTEC). What is the most likely causative organism?
Explanation
Kingella kingae is a fastidious Gram-negative organism that is now recognized as the most common cause of septic arthritis in children younger than 4 years. It often requires inoculation into blood culture vials for successful growth.
Question 26
A 6-month-old infant with achondroplasia presents with poor feeding, hypotonia, and episodes of central apnea. Which of the following is the most critical screening study to perform?
Explanation
Infants with achondroplasia are at high risk for foramen magnum stenosis, which can cause cervicomedullary compression leading to central apnea, hypotonia, and sudden infant death. MRI is the modality of choice for evaluation.
Question 27
A 17-year-old male presents with chronic neck pain. Radiographs demonstrate an expansile lesion in the posterior elements of C4.
Histologically, the lesion consists of woven bone trabeculae lined by prominent osteoblasts. Which of the following strongly differentiates this lesion from an osteoid osteoma?
Histologically, the lesion consists of woven bone trabeculae lined by prominent osteoblasts. Which of the following strongly differentiates this lesion from an osteoid osteoma?
Explanation
Osteoblastoma and osteoid osteoma are histologically identical. They are differentiated primarily by size, with osteoblastoma defined as being larger than 2 cm.
Question 28
A 9-year-old boy presents with severe thigh pain, high fever, and a swollen, erythematous leg. MRI confirms osteomyelitis of the femur and an adjacent deep venous thrombosis (DVT). Blood cultures grow gram-positive cocci. Which of the following virulence factors is most strongly associated with this severe clinical presentation?
Explanation
Panton-Valentine leukocidin (PVL) is a cytotoxin frequently produced by community-acquired MRSA. It is associated with severe musculoskeletal infections, multifocal osteomyelitis, adjacent myositis, and deep venous thrombosis.
Question 29
A 4-year-old child with disproportionate short-trunk dwarfism is evaluated. Radiographs show delayed ossification of the femoral heads, severe coxa vara, and platyspondyly. Ocular examination reveals high myopia. A mutation in which of the following genes is the most likely cause?
Explanation
Spondyloepiphyseal dysplasia congenita (SEDC) presents with short-trunk dwarfism, coxa vara, platyspondyly, and ocular issues like high myopia or retinal detachment. It is caused by a mutation in the COL2A1 gene.
Question 30
A 6-year-old boy presents with localized back pain. Radiographs show a completely flattened C5 vertebral body (vertebra plana) with intact adjacent disc spaces. Biopsy of the lesion would most likely show cells positive for which of the following markers?
Explanation
The presentation of vertebra plana in a child is highly characteristic of Eosinophilic Granuloma (Langerhans Cell Histiocytosis). The Langerhans cells are characteristically positive for S100 and CD1a, and contain Birbeck granules on electron microscopy.
Question 31
A 12-year-old boy has a permeative lytic lesion in the femoral diaphysis with an associated "onion-skin" periosteal reaction. Biopsy reveals sheets of uniform small round blue cells. Which of the following chromosomal translocations is most characteristic of this tumor?
Explanation
Ewing sarcoma is a small round blue cell tumor that classically presents in the diaphysis of long bones with an onion-skin periosteal reaction. It is characterized by the t(11;22) translocation resulting in the EWS-FLI1 fusion gene.
Question 32
A 3-year-old child presents with a waddling gait and joint hyperlaxity. The child appeared normal at birth but developed disproportionate short-limb dwarfism over the last year. Facial features and intelligence are normal. Radiographs show small, irregular epiphyses and metaphyseal flaring. A mutation in which gene is responsible?
Explanation
Pseudoachondroplasia is caused by a mutation in Cartilage Oligomeric Matrix Protein (COMP). Unlike true achondroplasia, children appear normal at birth, develop symptoms in early childhood, have normal facies, and exhibit significant joint laxity.
Question 33
An 11-year-old girl presents with recurrent episodes of clavicular and tibial pain with mild swelling. Radiographs show lytic and sclerotic changes in the medial clavicle and proximal tibia. Multiple biopsies show chronic inflammation but all bacterial, fungal, and mycobacterial cultures remain sterile. What is the most appropriate initial treatment?
Explanation
Chronic Recurrent Multifocal Osteomyelitis (CRMO) is an autoinflammatory condition characterized by sterile inflammatory bone lesions. First-line treatment consists of nonsteroidal anti-inflammatory drugs (NSAIDs).
Question 34
A 14-year-old boy presents with progressive knee pain. Radiographs reveal a well-circumscribed, eccentrically located lytic lesion with a sclerotic margin, entirely contained within the proximal tibial epiphysis. Histology shows mononuclear cells, osteoclast-like giant cells, and areas of "chicken-wire" calcification. What is the diagnosis?
Explanation
Chondroblastoma is a rare, benign cartilaginous tumor that characteristically arises in the epiphysis or apophysis of long bones in children with open physes. Histology classically demonstrates "chicken-wire" calcifications.
Question 35
A 9-year-old girl from Connecticut presents with a massive, painless effusion of her right knee. She is afebrile and bears weight with a mild limp. Joint fluid aspiration yields 25,000 WBCs/mm3. Serology is positive for Borrelia burgdorferi. What is the most appropriate initial management?
Explanation
Lyme arthritis frequently presents as a massive, relatively painless knee effusion in an endemic area. The initial treatment for late Lyme arthritis in a child > 8 years old is a 28-day course of oral doxycycline.
Question 36
An 8-year-old boy sustains a minor twisting injury to his arm and complains of shoulder pain. Radiographs show a centrally located, completely radiolucent lesion in the proximal humeral metaphysis extending to the physis. A small fragment of bone is seen resting at the dependent portion of the cyst. What is the most likely diagnosis?
Explanation
The description is classic for a unicameral bone cyst (simple bone cyst). The "fallen leaf" or "fallen fragment" sign indicates a pathologic fracture through a fluid-filled cystic lesion, which is highly suggestive of a UBC.
Question 37
A 10-year-old boy presents with bilateral knee and hip pain, and a waddling gait. Radiographs show delayed, irregular, and fragmented ossification centers of the capital femoral epiphyses. Lateral knee radiographs demonstrate a "double-layer" patella. Spinal radiographs are entirely normal. What is the most likely diagnosis?
Explanation
Multiple epiphyseal dysplasia (MED) presents with delayed and irregular ossification of multiple epiphyses leading to early osteoarthritis, but uniquely leaves the spine relatively spared (differentiating it from SED). A "double-layer" patella is a classic radiographic sign.
Question 38
A 7-year-old girl with homozygous sickle cell disease (HbSS) presents with severe bone pain, high fever, and swelling over the midshaft of her radius. MRI confirms diaphyseal osteomyelitis. While Staphylococcus aureus is highly prevalent, this patient is uniquely at high risk for infection from which of the following organisms?
Explanation
While Staphylococcus aureus is still the most common cause of osteomyelitis in the general pediatric population and very common in sickle cell disease, patients with sickle cell hemoglobinopathies are at uniquely high risk for Salmonella osteomyelitis.
Question 39
A 15-year-old male presents with chronic back pain, which is worse at night and incompletely relieved by NSAIDs. Radiographs reveal an expansile, lytic lesion in the posterior elements of L3.
Based on the clinical presentation and typical radiographic findings shown, what is the most likely diagnosis?
Based on the clinical presentation and typical radiographic findings shown, what is the most likely diagnosis?
Explanation
Osteoblastoma typically presents as an expansile lytic lesion >2 cm in the posterior elements of the spine. Unlike osteoid osteoma, the pain is generally dull, aching, and less likely to be completely relieved by NSAIDs.
Question 40
A 2-week-old neonate presents with pseudoparalysis of the right leg. Ultrasound shows a large hip effusion, and aspiration yields frank pus.
What is the most appropriate surgical approach for emergency drainage of this joint?
What is the most appropriate surgical approach for emergency drainage of this joint?
Explanation
The anterior (Smith-Petersen) approach is the standard for pediatric hip arthrotomy to drain septic arthritis. It provides direct, safe access to the joint capsule while avoiding damage to the critical lateral epiphyseal vessels.
Question 41
A 5-year-old child with a known diagnosis of achondroplasia is being evaluated. What is the most common cause of early childhood mortality in patients with this condition?
Explanation
Foramen magnum stenosis leading to cervicomedullary compression and subsequent central apnea is the leading cause of mortality in infants and young children with achondroplasia. Careful neurologic monitoring is mandatory.
Question 42
A 14-year-old boy presents with distal femur pain. Radiographs demonstrate a mixed lytic and sclerotic lesion with a sunburst periosteal reaction. A core needle biopsy is performed. What histologic feature is mandatory for the diagnosis of osteosarcoma?
Explanation
The defining histologic characteristic of osteosarcoma is the production of malignant osteoid or immature bone directly by malignant mesenchymal cells. This distinguishes it from other high-grade sarcomas.
Question 43
A 10-year-old girl is diagnosed with a diaphyseal femur tumor characterized by onion-skin periosteal reaction and CD99-positive small round blue cells. What is the most common cytogenetic translocation associated with this tumor?
Explanation
Ewing sarcoma is characterized by the t(11;22)(q24;q12) translocation in approximately 85% of cases. This results in the EWS-FLI1 fusion protein, which drives tumor pathogenesis.
Question 44
An 18-month-old child presents with a limp, low-grade fever, and refusal to bear weight. Blood labs show CRP 25 mg/L and WBC 11,000/mm3. Standard synovial fluid culture is negative at 48 hours. To isolate the most likely causative organism in this age group, which laboratory technique should have been utilized?
Explanation
Kingella kingae is the most common cause of septic arthritis in children under 4 years old. It is a fastidious Gram-negative organism; inoculating synovial fluid into BACTEC aerobic blood culture vials or utilizing PCR significantly increases diagnostic yield.
Question 45
A 6-year-old child presents with short-trunk dwarfism, corneal clouding, normal intelligence, and marked atlantoaxial instability secondary to odontoid hypoplasia. Which enzyme deficiency is responsible for this condition?
Explanation
Morquio syndrome (Mucopolysaccharidosis Type IV) is caused by a deficiency in galactosamine-6-sulfatase (Type A) or beta-galactosidase (Type B). It classically presents with severe skeletal dysplasia, odontoid hypoplasia predisposing to cervical myelopathy, and normal intelligence.
Question 46
A newborn presents with short-limbed dwarfism, rigid equinovarus foot deformities, "hitchhiker" thumbs, and cystic swelling of the pinnae (cauliflower ears). What is the underlying genetic mutation for this condition?
Explanation
Diastrophic dysplasia is an autosomal recessive disorder caused by a mutation in the DTDST (SLC26A2) gene. This gene encodes a sulfate transporter, and its mutation leads to impaired sulfation of cartilage proteoglycans.
Question 47
A 19-year-old male with chronic neck pain undergoes biopsy of an expansile lesion in the C4 lamina. Histology is shown below.
Based on the photomicrograph and clinical presentation, what is the most appropriate definitive management?
Based on the photomicrograph and clinical presentation, what is the most appropriate definitive management?
Explanation
The image demonstrates osteoblastoma, characterized by loose fibrovascular connective tissue intermixed with irregular osteoid. Treatment consists of surgical excision, typically via thorough intralesional curettage and bone grafting or marginal en bloc resection.
Question 48
A 10-year-old girl is evaluated for a broad skull, delayed fontanelle closure, and the unusual ability to touch her shoulders together anteriorly. Which gene mutation is responsible for her condition?
Explanation
Cleidocranial dysplasia is an autosomal dominant condition caused by mutations in the RUNX2 (CBFA1) gene, which is a master transcription factor for osteoblast differentiation. Key features include hypoplastic or absent clavicles and delayed cranial suture closure.
Question 49
A 9-year-old girl presents with multiple recurrent episodes of bone pain and swelling in her clavicle and distal tibia. Labs show a mildly elevated ESR but normal WBC count. Multiple biopsies reveal sterile, non-infectious inflammation. What is the first-line treatment for this condition?
Explanation
Chronic Recurrent Multifocal Osteomyelitis (CRMO) is an autoinflammatory bone disorder characterized by sterile bone lesions. NSAIDs are the first-line treatment, successfully controlling symptoms in the majority of patients.
Question 50
A 7-year-old boy presents with a lytic skull lesion and back pain due to a collapsed vertebral body (vertebra plana). Biopsy reveals an abundance of distinct histiocytes with grooved nuclei. Which immunohistochemical markers are classically positive in the lesional cells?
Explanation
The presentation of vertebra plana and lytic skull lesions is classic for Eosinophilic Granuloma (Langerhans cell histiocytosis). The Langerhans cells are immunohistochemically positive for S-100 and CD1a, and show Birbeck granules on electron microscopy.
Question 51
A 6-year-old boy from Connecticut presents with an acute, massive right knee effusion and an intermittent limp. He is afebrile, and the joint aspirate yields 45,000 WBCs/mm3. What diagnostic test sequence is recommended to confirm the suspected diagnosis?
Explanation
Lyme arthritis typically presents with a large, minimally tender effusion in endemic areas. Diagnosis relies on two-tier serologic testing: an initial enzyme immunoassay (EIA) followed by a confirmatory Western blot.
Question 52
An 8-year-old boy presents with mild shoulder pain after throwing a baseball. X-rays reveal a centrally located, lytic, slightly expansile lesion in the proximal humerus metaphysis with a visible "fallen leaf" sign. Which of the following is true regarding the management of this lesion?
Explanation
The "fallen leaf" sign is pathognomonic for a Unicameral Bone Cyst (UBC). First-line treatment for active, symptomatic, or fracture-prone UBCs often includes minimally invasive techniques like corticosteroid or bone marrow aspirate injections.
Question 53
A 17-year-old male presents with persistent, dull aching pain in his mid-back that is not reliably relieved by NSAIDs. Imaging shows a 3.5 cm expansile radiolucent lesion in the posterior elements of T10. Biopsy is performed and reveals the following histology:
What is the most likely diagnosis?
What is the most likely diagnosis?
Explanation
The presentation of a spinal posterior element lesion >2 cm with histology showing loose fibrovascular stroma and irregular osteoid is characteristic of osteoblastoma. Unlike osteoid osteoma, the pain is often less responsive to NSAIDs and the lesion exceeds 1.5-2.0 cm.
Question 54
A 15-year-old girl presents with progressive back pain. Radiographs of her spine demonstrate an expansile, predominantly lytic lesion as shown in image A.
If this lesion is confirmed as an osteoblastoma, what is the most common spinal compartment initially involved?
If this lesion is confirmed as an osteoblastoma, what is the most common spinal compartment initially involved?
Explanation
Osteoblastomas most frequently arise in the posterior elements of the spine (lamina, spinous process, pedicles). They typically present as expansile lytic lesions with varying degrees of sclerosis and cortical thinning.
Question 55
A 3-week-old neonate presents with a swollen, erythematous right thigh and pseudoparalysis. An ultrasound confirms a hip effusion, and radiographs show early destructive changes in the proximal femur.
What anatomic factor strongly predisposes neonates to concurrent osteomyelitis and septic arthritis of the hip?
What anatomic factor strongly predisposes neonates to concurrent osteomyelitis and septic arthritis of the hip?
Explanation
In infants younger than 18 months, transphyseal blood vessels cross the physis. This allows hematogenous infection to easily spread between the metaphysis and the epiphysis or joint space, causing concurrent osteomyelitis and septic arthritis.
Question 56
A 4-year-old boy with achondroplasia presents for a routine orthopedic evaluation. His parents are concerned about his bowing legs and his occasional snoring. Which of the following is the most critical screening evaluation recommended to prevent sudden mortality in this patient population?
Explanation
Children with achondroplasia are at high risk for foramen magnum stenosis, which can cause cervicomedullary compression, central sleep apnea, and sudden death. Screening with sleep studies and a careful neurological exam is critical, often prompting MRI evaluation.
Question 57
A 9-year-old boy presents with a pathologic fracture of the proximal humerus following a minor fall. Radiographs show a centrally located, completely lytic lesion in the metaphysis that does not breach the cortex, with a small bony fragment settled at the bottom of the cyst. What is the most appropriate initial management after fracture healing?
Explanation
The presentation and the "fallen leaf" sign are classic for a unicameral bone cyst (UBC). First-line treatment for an active UBC after fracture healing typically involves observation or minimally invasive options like corticosteroid injections.
Question 58
A 6-year-old girl with blue sclerae and a history of multiple low-impact fractures is diagnosed with Osteogenesis Imperfecta (OI). Which underlying genetic defect is most commonly responsible for her condition?
Explanation
Osteogenesis imperfecta is most commonly caused by autosomal dominant mutations in the COL1A1 or COL1A2 genes. These genes encode the alpha chains of type I collagen, leading to brittle bones and varying degrees of connective tissue abnormalities.
Question 59
A 7-year-old boy from Connecticut presents with acute right knee swelling and a limp. He is afebrile with a WBC of 9,000/mm³ and an ESR of 30 mm/hr. Joint aspiration yields 45,000 WBCs/mm³ with a predominance of PMNs. What is the most appropriate next step in diagnosis?
Explanation
In a Lyme-endemic area, a child with monoarticular knee effusion, low inflammatory markers, and a moderate joint WBC count often has Lyme arthritis. Testing with two-tiered Lyme serology is indicated before considering surgical intervention.
Question 60
A 12-year-old boy presents with pain and swelling in his mid-thigh. Radiographs show a permeative diaphyseal lesion with an "onion skin" periosteal reaction. Genetic testing reveals a t(11;22) chromosomal translocation. What fusion protein is associated with this specific translocation?
Explanation
Ewing sarcoma is classically associated with the t(11;22) chromosomal translocation. This specific translocation results in the production of the aberrant EWS-FLI1 fusion protein.
Question 61
A 10-year-old girl is evaluated for short stature and delayed primary tooth eruption. On examination, she is able to bring her shoulders together anteriorly. Radiographs reveal absent clavicles and delayed skull ossification. Which transcription factor is mutated in this condition?
Explanation
Cleidocranial dysplasia is an autosomal dominant condition caused by mutations in the RUNX2 (CBFA1) gene, which is essential for osteoblast differentiation. It presents with hypoplastic clavicles, delayed cranial suture closure, and dental anomalies.
Question 62
A 5-year-old African American child with homozygous sickle cell disease presents with high fever and severe left arm pain. Radiographs show periosteal elevation of the radial diaphysis. While Staphylococcus aureus remains common, which of the following organisms is disproportionately frequent in this specific patient population?
Explanation
Children with sickle cell disease are particularly susceptible to Salmonella osteomyelitis due to functional asplenia and localized bone infarcts serving as a nidus. However, S. aureus is still an overall common cause in these patients.
Question 63
An 11-year-old boy presents with night-time right thigh pain that dramatically improves within 30 minutes of taking ibuprofen. Radiographs demonstrate a dense sclerotic lesion in the proximal femur with a 1-cm central radiolucent nidus. What is the most common definitive treatment currently utilized for this condition?
Explanation
The clinical presentation is classic for an osteoid osteoma. Percutaneous radiofrequency ablation (RFA) under CT guidance is the standard of care for definitive treatment, offering high success rates with minimal morbidity compared to open surgery.
Question 64
A 14-year-old boy with a family history of Multiple Hereditary Exostoses (MHE) is evaluated for a rapidly growing bump on his distal femur. What is the approximate lifetime risk of malignant transformation of an osteochondroma in patients with MHE?
Explanation
The risk of malignant transformation of an osteochondroma to a secondary chondrosarcoma is approximately 1-5% in patients with Multiple Hereditary Exostoses. This is significantly higher than the risk in patients with isolated, solitary osteochondromas (<1%).
Question 65
A 9-year-old girl presents with recurrent episodes of bone pain and swelling involving the clavicles and distal tibias. Blood cultures are repeatedly negative, and a bone biopsy reveals sterile, non-specific chronic inflammation. She also has palmoplantar pustulosis. What is the first-line treatment for this condition?
Explanation
The presentation is consistent with Chronic Recurrent Multifocal Osteomyelitis (CRMO), an autoinflammatory bone disease associated with dermatologic conditions. NSAIDs are the first-line therapy, while bisphosphonates or biologics are used for refractory cases.
Question 66
A 13-year-old girl presents with knee pain. MRI reveals a multiloculated, expansile metaphyseal lesion in the proximal tibia with prominent fluid-fluid levels. Biopsy confirms an Aneurysmal Bone Cyst (ABC). What primary genetic alteration is frequently associated with primary ABCs?
Explanation
Primary Aneurysmal Bone Cysts are now recognized as true neoplasms driven by USP6 gene rearrangements (typically t(16;17)). Fluid-fluid levels on MRI are characteristic, representing blood settling in cystic spaces.
Question 67
A 17-year-old male presents with dull, aching back pain that is not relieved by NSAIDs. Radiographs show a 3 cm expansile lesion in the posterior elements of L3. Biopsy reveals the following histology.
What is the most likely diagnosis?
What is the most likely diagnosis?
Explanation
The image shows loose fibrovascular connective tissue intermixed with irregular osteoid, typical of osteoblastoma. Unlike osteoid osteoma, osteoblastomas are larger than 2 cm and the pain is typically not relieved by NSAIDs.
Question 68
A 15-year-old girl presents with a painful scoliosis. Radiographs of the spine are obtained as shown.
If this lesion causes a scoliotic deformity, which of the following best describes the typical curve pattern?
If this lesion causes a scoliotic deformity, which of the following best describes the typical curve pattern?
Explanation
Osteoid osteomas and osteoblastomas in the spine typically cause a painful scoliosis with the apex of the curve directed away from the lesion. This creates a concavity on the side of the lesion due to asymmetric muscle spasm.
Question 69
A 3-week-old neonate presents with fever, irritability, and decreased movement of the left lower extremity. Imaging demonstrates a hip effusion.
What is the most appropriate empiric intravenous antibiotic regimen after obtaining aspirates?
What is the most appropriate empiric intravenous antibiotic regimen after obtaining aspirates?
Explanation
Neonatal septic arthritis requires broad coverage for S. aureus, Group B Streptococcus, and Gram-negative bacilli. Vancomycin and cefotaxime are preferred; ceftriaxone is avoided in neonates due to the risk of biliary sludging and kernicterus.
Question 70
An 8-year-old boy presents with a permeative lytic lesion in the diaphysis of the femur with a prominent periosteal reaction. Biopsy reveals sheets of uniform small round blue cells that are CD99 positive. Which specific chromosomal translocation is most characteristic of this tumor?
Explanation
Ewing sarcoma is a small round blue cell tumor characterized by strong CD99 positivity and the t(11;22)(q24;q12) translocation. This results in the EWS-FLI1 fusion protein, which acts as an aberrant transcription factor.
Question 71
A 14-year-old boy with distal femoral osteosarcoma completes neoadjuvant chemotherapy and undergoes limb-salvage surgery. Which of the following is the most important independent prognostic factor for his long-term survival?
Explanation
The degree of tumor necrosis following neoadjuvant chemotherapy is the most significant prognostic factor for overall survival in osteosarcoma. Greater than 90% necrosis indicates a good histological response to chemotherapy.
Question 72
A 6-year-old girl presents with a limp, precocious puberty, and large, irregular cafe-au-lait spots on her torso. Radiographs show ground-glass appearing expansile lesions in her proximal femur resulting in a "shepherd's crook" deformity. What is the underlying genetic mutation?
Explanation
McCune-Albright syndrome consists of polyostotic fibrous dysplasia, endocrinopathies (like precocious puberty), and cafe-au-lait spots with "coast of Maine" irregular borders. It is caused by a somatic activating mutation in the GNAS1 gene.
Question 73
A 9-year-old girl has had intermittent clavicle and distal tibial pain for 6 months. Inflammatory markers are mildly elevated. Multiple bone biopsies yield no bacterial growth and show chronic non-suppurative inflammation. What is the most appropriate first-line treatment?
Explanation
Chronic Recurrent Multifocal Osteomyelitis (CRMO) is an autoinflammatory bone disease presenting with sterile bony lesions. NSAIDs are the first-line treatment and effectively manage symptoms in the majority of patients.
Question 74
A 4-year-old boy with achondroplasia presents with progressive weakness in his upper and lower extremities and sleep apnea. What is the most likely anatomic cause of these new neurologic findings?
Explanation
In infants and young children with achondroplasia, foramen magnum stenosis can cause cervicomedullary compression leading to sleep apnea, hyperreflexia, and tetraparesis. It may require urgent suboccipital decompression.
Question 75
A 6-year-old boy with short-trunk dwarfism, corneal clouding, and normal intelligence is diagnosed with Morquio syndrome (MPS IV). He is at highest risk for developing which of the following orthopedic conditions?
Explanation
Morquio syndrome (MPS IV) is caused by an inability to degrade keratan sulfate. Patients are at exceptionally high risk for life-threatening cervical myelopathy secondary to atlantoaxial instability from severe odontoid hypoplasia.
Question 76
A 10-year-old boy is brought in for an abnormal shoulder appearance. He has excessive shoulder mobility and can touch his shoulders together anteriorly. Radiographs show complete absence of the clavicles. Which gene is primarily mutated in this condition?
Explanation
Cleidocranial dysplasia is an autosomal dominant condition characterized by absent or hypoplastic clavicles, delayed cranial suture closure, and dental anomalies. It is caused by a mutation in the RUNX2 (CBFA1) transcription factor, critical for osteoblast differentiation.
Question 77
A 7-year-old boy from Connecticut presents with a massive, painless right knee effusion. He is afebrile, weight-bearing, and has a WBC of 8,000 cells/mcL and an ESR of 25 mm/h. Joint aspiration reveals a WBC count of 45,000/mcL. Gram stain is negative. What is the most appropriate next step in diagnosis?
Explanation
A large, relatively painless joint effusion in a Lyme-endemic area without significant systemic toxicity strongly suggests Lyme arthritis. The diagnosis is confirmed via two-tiered serology (EIA/IFA followed by Western blot).
Question 78
A 16-year-old male presents with chronic, dull back pain that is not completely relieved by NSAIDs. Radiographs show a 3 cm expansile lesion in the posterior elements of the lumbar spine. A biopsy is obtained, revealing loose fibrovascular connective tissue intermixed with irregular woven bone trabeculae and active osteoblasts, with no nuclear atypia.
Which of the following statements is true regarding this lesion?
Which of the following statements is true regarding this lesion?
Explanation
Osteoblastomas are histologically identical to osteoid osteomas but are differentiated primarily by size (greater than 2 cm). Unlike osteoid osteomas, they do not produce proportional prostaglandin E2 levels, so they lack the classic dramatic pain relief with NSAIDs.
Question 79
A 3-week-old premature neonate presents with asymmetric hip creases, irritability, and decreased spontaneous movement of the right lower extremity. Ultrasound reveals a large right hip effusion.
Following diagnostic aspiration that yields purulent fluid, which of the following empiric antibiotic regimens is most appropriate for this patient?
Following diagnostic aspiration that yields purulent fluid, which of the following empiric antibiotic regimens is most appropriate for this patient?
Explanation
Neonatal septic arthritis empiric coverage must account for S. aureus, Group B Streptococcus, and gram-negative bacilli. Cefotaxime and Vancomycin are preferred; Ceftriaxone is contraindicated in neonates due to the risk of biliary sludging and kernicterus.
Question 80
A 4-year-old child presents with rhizomelic short stature, a prominent forehead, midface hypoplasia, and a diagnosis of achondroplasia. Genetic testing confirms a mutation in the FGFR3 gene. Which of the following spinal manifestations is most likely to become symptomatic and require surgical intervention in adulthood?
Explanation
In achondroplasia, narrowed interpedicular distances and congenitally short pedicles lead to absolute spinal canal stenosis. Lumbar spinal stenosis is the most common spinal complication requiring surgical decompression in adult patients with this dysplasia.
Question 81
A 12-year-old boy presents with severe, progressive knee pain. Radiographs reveal a mixed lytic and sclerotic lesion in the distal femoral metaphysis with a "sunburst" periosteal reaction and Codman's triangle. Core needle biopsy confirms high-grade, conventional osteosarcoma. Which of the following factors is most predictive of this patient's long-term survival?
Explanation
The most important prognostic factor for overall survival in high-grade osteosarcoma is the histologic response to neoadjuvant chemotherapy. A good response is defined as greater than 90% tumor necrosis in the resected specimen.
Question 82
A 6-year-old girl with blue sclerae, dentinogenesis imperfecta, and a history of multiple low-energy long bone fractures is diagnosed with Osteogenesis Imperfecta (OI). She is started on an intravenous bisphosphonate protocol. What is the primary cellular mechanism of action of this medication in the treatment of her condition?
Explanation
Bisphosphonates are taken up by osteoclasts during bone resorption, leading to inhibition of the mevalonate pathway, loss of osteoclast function, and subsequent apoptosis. This decreases the overall rate of bone turnover, increasing bone mineral density in OI patients.
Question 83
An 8-year-old boy presents to the emergency department after a minor fall onto his arm. Radiographs demonstrate a pathologic fracture through a centrally located, purely radiolucent lesion in the proximal humeral metaphysis. A radiopaque fragment is noted resting at the dependent portion of the cyst (the "fallen leaf" sign). What is the most appropriate initial management for this presentation?
Explanation
This presentation is pathognomonic for a fractured unicameral bone cyst (UBC). The initial management is nonoperative with closed reduction and immobilization to allow the fracture to heal; many UBCs will spontaneously consolidate during the fracture healing process.
Question 84
A 10-year-old girl presents with a 6-month history of intermittent, multifocal bone pain involving the medial clavicle and bilateral proximal tibias. Laboratory studies show a mildly elevated ESR, but multiple bone biopsies show sterile, non-suppurative inflammation. Radiographs reveal mixed lytic and sclerotic metaphyseal lesions. Which of the following is the most appropriate first-line treatment for this condition?
Explanation
This clinical picture describes Chronic Recurrent Multifocal Osteomyelitis (CRMO), an autoinflammatory bone disease. The first-line treatment for CRMO is the scheduled use of Nonsteroidal anti-inflammatory drugs (NSAIDs), which provide symptom relief and can induce remission.
Question 85
A 9-year-old boy is evaluated for unusual shoulder mobility. On examination, he is able to approximate his shoulders in the midline anteriorly. Physical exam also reveals a broad skull, delayed fontanelle closure, and multiple retained deciduous teeth. A mutation in which of the following genes is responsible for this patient's condition?
Explanation
The patient has Cleidocranial Dysplasia, characterized by hypoplastic/aplastic clavicles, delayed skull ossification, and dental anomalies. It is caused by an autosomal dominant mutation in the RUNX2 (also known as CBFA1) gene, which is essential for osteoblast differentiation.
Question 86
A 17-year-old male complains of chronic, dull back pain that is worse at night but has an inconsistent response to NSAIDs. A biopsy is obtained, and the histology demonstrates loose fibrovascular connective tissue intermixed with irregular osteoid and plump osteoblasts.
Which of the following clinical or radiographic features distinguishes this lesion from an osteoid osteoma?
Which of the following clinical or radiographic features distinguishes this lesion from an osteoid osteoma?
Explanation
Osteoblastomas are histologically identical to osteoid osteomas but are defined by a size greater than 2.0 cm. They typically have a varied response to NSAIDs and lack the massive reactive sclerosis often seen in osteoid osteomas.
Question 87
A 14-year-old male presents with painful scoliosis and back spasms. Radiographs demonstrate an expansile lytic lesion in the posterior elements of L3.
If this lesion is responsible for the patient's scoliosis, what is the expected curve pattern?
If this lesion is responsible for the patient's scoliosis, what is the expected curve pattern?
Explanation
Painful spinal lesions like osteoblastomas and osteoid osteomas provoke severe asymmetric muscle spasms on the side of the tumor. This causes concavity towards the lesion, meaning the apex of the scoliotic curve points away from it.
Question 88
A 4-week-old female is treated for culture-proven septic arthritis of the right hip.
Which unique anatomical factor makes the neonatal hip highly susceptible to permanent avascular necrosis and physeal destruction from this condition?
Which unique anatomical factor makes the neonatal hip highly susceptible to permanent avascular necrosis and physeal destruction from this condition?
Explanation
In neonates, the proximal femoral metaphysis is entirely intra-capsular. This allows metaphyseal osteomyelitis to decompress directly into the joint space, increasing intra-articular pressure and obliterating epiphyseal blood supply, leading to avascular necrosis.
Question 89
A 2-year-old boy with achondroplasia presents for a routine orthopedic evaluation. His parents are concerned about his prominent forehead and bowing legs. What is the most common spinal abnormality requiring surgical intervention in adulthood for patients with this condition?
Explanation
Lumbar spinal stenosis is the most common reason for spinal surgery in adult achondroplastic patients. It is caused by anatomically short pedicles and a pathognomonic decrease in interpedicular distance from the upper to lower lumbar spine.
Question 90
An 8-year-old boy presents with an aggressive, permeative diaphyseal lesion in his femur with a classic 'onion-skin' periosteal reaction. A core needle biopsy is performed to confirm the diagnosis. Which immunohistochemical marker is most consistently positive in this specific tumor?
Explanation
The clinical and radiographic presentation is classic for Ewing sarcoma. Ewing sarcoma strongly and diffusely expresses the CD99 (MIC2) surface antigen due to the characteristic t(11;22) translocation forming the EWS-FLI1 fusion protein.
Question 91
A 10-year-old girl complains of intermittent proximal tibial pain for 3 months. Laboratory tests show a normal WBC count and a slightly elevated ESR. Radiographs reveal a well-circumscribed lucency in the proximal tibial metaphysis surrounded by a thick sclerotic margin. What is the most likely diagnosis?
Explanation
A Brodie's abscess is a form of subacute osteomyelitis that presents with mild or absent systemic signs. Radiographically, it appears as a well-defined lytic lesion with a dense sclerotic rim, most commonly in the metaphysis of long bones.
Question 92
A 5-year-old child presents with a history of recurrent low-energy fractures, blue sclerae, and early-onset hearing loss. Genetic testing confirms Osteogenesis Imperfecta Type I. What is the underlying molecular defect?
Explanation
Osteogenesis Imperfecta Type I is characterized by a quantitative defect, meaning there is decreased production of structurally normal Type I collagen. Types II, III, and IV involve qualitative defects where abnormal collagen is produced.
Question 93
A 12-year-old boy presents with multiple painless, bony bumps over his knees and shoulders. Radiographs show sessile bony projections that are continuous with the medullary cavity of the host bone. Mutations in which of the following genes are responsible for this condition?
Explanation
Multiple Hereditary Exostoses (MHE) is an autosomal dominant condition caused by mutations in the tumor suppressor genes EXT1 and EXT2. These mutations disrupt heparan sulfate synthesis, leading to the formation of multiple osteochondromas.
Question 94
A 6-year-old boy presents with disproportionate short trunk dwarfism, normal intelligence, a barrel chest, and severe coxa vara. Radiographs show significant delay in epiphyseal ossification and platyspondyly. What is the molecular basis of this child's skeletal dysplasia?
Explanation
Spondyloepiphyseal dysplasia (SED) affects the spine and epiphyses, leading to a short trunk and coxa vara. It is caused by mutations in the COL2A1 gene, resulting in defective Type II collagen, the primary structural collagen in hyaline cartilage.
Question 95
A 7-year-old boy presents with high fever, chills, and an inability to bear weight on his left leg. Examination reveals severe focal tenderness over the distal femur. Which region of the bone is the initial nidus for bacterial seeding in acute hematogenous osteomyelitis in this age group?
Explanation
In children over the age of 1 year, the metaphysis is the most common site of acute hematogenous osteomyelitis. Sluggish blood flow in the metaphyseal venous sinusoids adjacent to the physis predisposes this area to bacterial settling and infection.
Question 96
A 9-year-old boy sustains a pathological fracture through a central, lytic lesion in the proximal humerus after throwing a baseball. Radiographs demonstrate the 'fallen leaf' sign. What is the recommended initial management if the cyst remains active and expansile after the fracture heals?
Explanation
The 'fallen leaf' sign is pathognomonic for a unicameral bone cyst (UBC). If the cyst remains active and prone to refracture after initial healing, intralesional aspiration and injection (corticosteroids, BMA, or DBM) is the first-line surgical treatment.
Question 97
A 6-year-old girl from Connecticut presents with a massive, painless effusion of the right knee. She had an uncharacterized rash several months prior. Joint aspiration yields 40,000 WBCs with predominantly mononuclear cells. What is the recommended initial serological test to confirm the suspected diagnosis?
Explanation
Lyme disease arthritis typically presents as a large, relatively painless effusion with mononuclear cell predominance. Diagnosis follows a two-tier protocol: an initial ELISA (or EIA), followed by a Western blot to confirm positive or equivocal ELISA results.
Question 98
A 4-year-old boy with Morquio syndrome (Mucopolysaccharidosis Type IV) presents for orthopedic evaluation. Before clearing this patient for general anesthesia for a hernia repair, which critical cervical spine abnormality must be urgently ruled out?
Explanation
Morquio syndrome is classically associated with severe odontoid hypoplasia and ligamentous laxity, resulting in life-threatening atlantoaxial instability. Flexion-extension cervical radiographs must be obtained before any procedure requiring intubation.
Question 99
A 14-year-old girl gets an ankle radiograph after a mild sprain. An incidental eccentric, lucent, cortically-based lesion with a scalloped sclerotic border is found in the distal tibial metaphysis. She has no pain at the site. What is the most appropriate management?
Explanation
The radiographic description is classic for a non-ossifying fibroma (NOF). Since the lesion is asymptomatic and incidentally found, reassurance and observation are appropriate as these lesions spontaneously ossify and resolve by skeletal maturity.
Question 100
A 4-year-old child presents with a waddling gait, short stature, and significant joint laxity. Unlike classic achondroplasia, the child has normal facial features and head circumference. Radiographs show delayed epiphyseal ossification and irregular, fragmented epiphyses. A mutation in which gene is responsible for this condition?
Explanation
Pseudoachondroplasia is clinically distinguished from achondroplasia by normal facial features and intelligence. It is caused by mutations in the Cartilage Oligomeric Matrix Protein (COMP) gene, leading to accumulation of abnormal protein in the chondrocyte rER.
None
Previous ChapterEllis–Van Creveld’s Syndrome: Orthopedic Board Review
Next Chapter ABOS Board Review: Pediatric Orthopedics, Bone Tumors & Ske…

Medically Verified Content by
Prof. Dr. Mohammed Hutaif Clinic
Consultant Orthopedic & Spine Surgeon