ABOS Board Review: Bone Tumors, Mucopolysaccharidoses, & Dysplasias | Part 11
20 Jun 2026
49 min read
24 Views

Key Takeaway
ABOS Board Review Part 11 covers critical topics in orthopedic pathology, including primary bone lymphoma, mucopolysaccharidoses (MPS), chondromyxoid fibroma (CMF), and Progressive Diaphyseal Dysplasia. This section provides high-yield questions and rationales on clinical presentation, imaging characteristics, gross and histopathological features, and genetic inheritance patterns for comprehensive exam preparation.
ABOS Board Review: Bone Tumors, Mucopolysaccharidoses, & Dysplasias | Part 11
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 4-year-old boy presents with coarse facial features, joint stiffness, and hepatosplenomegaly but NO corneal clouding. Laboratory testing confirms a diagnosis of a specific mucopolysaccharidosis.
What is the mode of inheritance and deficient enzyme for this patient's condition?
What is the mode of inheritance and deficient enzyme for this patient's condition?
Explanation
Hunter syndrome (MPS II) is the only mucopolysaccharidosis with an X-linked recessive inheritance pattern and lacks corneal clouding. It is caused by a deficiency in iduronate-2-sulfatase.
Question 2
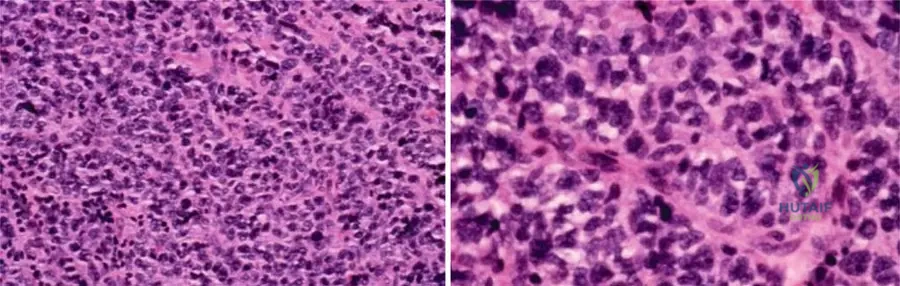
A 55-year-old male presents with thigh pain. Radiographs show a permeative diaphyseal lesion with minimal periosteal reaction. Biopsy reveals sheets of small round blue cells expressing CD20 and CD45.
What is the most appropriate initial management?
What is the most appropriate initial management?
Explanation
Primary bone lymphoma typically presents as a permeative lesion in older adults and stains positive for CD45 (LCA) and CD20 (B-cell marker). Treatment is primarily medical, utilizing systemic chemotherapy (e.g., R-CHOP) combined with localized radiation therapy.
Question 3
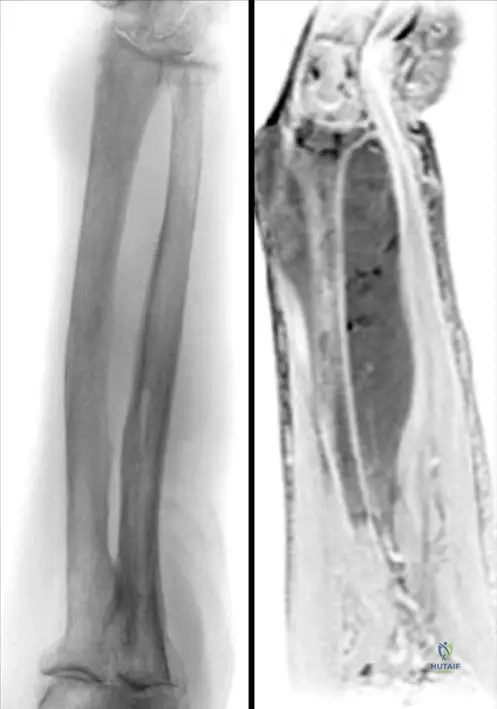
A 9-year-old boy presents with severe leg pain, muscle weakness, and a waddling gait. Radiographs show bilateral symmetric cortical thickening of the femoral and tibial diaphyses, sparing the epiphyses.
What is the underlying genetic mutation associated with this disorder?
What is the underlying genetic mutation associated with this disorder?
Explanation
Progressive Diaphyseal Dysplasia (Camurati-Engelmann disease) is characterized by symmetric diaphyseal cortical thickening. It is caused by an autosomal dominant mutation in the TGFB1 gene.
Question 4
A 22-year-old male presents with chronic knee pain. Radiographs show an eccentric, lytic, bubbly lesion with a sclerotic margin in the proximal tibial metaphysis.
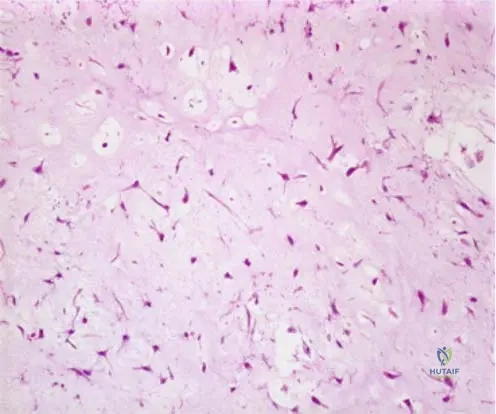
Histology shows stellate cells in a myxoid background with multinucleated giant cells at the lobular periphery. What is the diagnosis?
Histology shows stellate cells in a myxoid background with multinucleated giant cells at the lobular periphery. What is the diagnosis?
Explanation
Chondromyxoid fibroma is a rare benign cartilage tumor presenting as an eccentric metaphyseal lesion. Histologically, it features a lobular architecture with central myxoid tissue and peripheral hypercellularity with giant cells.
Question 5
A 6-year-old girl with normal intelligence presents with short trunk dwarfism, knock-knees, and a barrel chest. Flexion-extension cervical spine radiographs reveal significant atlantoaxial instability. Which of the following accumulated substances is most directly related to her condition?
Explanation
Morquio syndrome (MPS IV) uniquely features normal intelligence with severe skeletal dysplasia, notably atlantoaxial instability due to odontoid hypoplasia. It is characterized by the accumulation of keratan sulfate.
Question 6
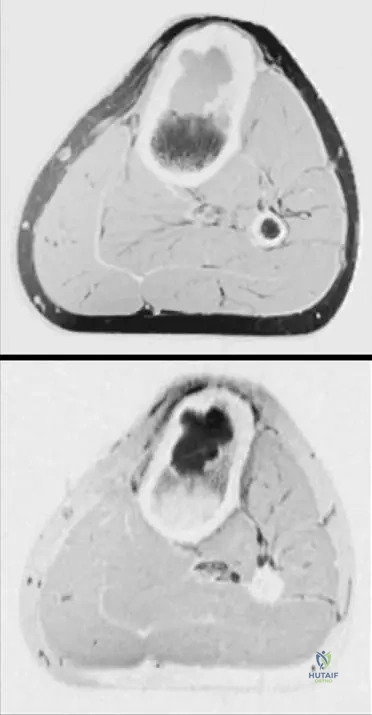
A 60-year-old female presents with shoulder pain. MRI reveals a large soft tissue mass surrounding the proximal humerus with diffuse marrow signal changes, but remarkably intact cortical bone on T1-weighted images.
What is the most likely diagnosis?
What is the most likely diagnosis?
Explanation
A classic imaging hallmark of primary bone lymphoma is a massive soft tissue mass associated with extensive marrow involvement but with relatively preserved or intact cortical bone.
Question 7
A 12-year-old girl is diagnosed with Camurati-Engelmann disease. She complains of severe bone pain and debilitating fatigue. Which of the following medical therapies is considered the most effective for relieving her symptoms?
Explanation
Systemic corticosteroids (glucocorticoids) are the mainstay of medical treatment for Progressive Diaphyseal Dysplasia (Camurati-Engelmann). They help relieve bone pain, improve muscle weakness, and can correct the waddling gait.
Question 8
A 4-year-old boy presents with a painless, asymmetric, hard mass on the medial aspect of his right ankle. Radiographs show an irregular, lobulated, ossifying mass arising from the medial aspect of the distal tibial epiphysis. What is the most likely diagnosis?
Explanation
Trevor disease (dysplasia epiphysealis hemimelica) involves asymmetrical cartilage overgrowth at the epiphysis, most commonly affecting the medial side of the knee or ankle in young children.
Question 9
A 28-year-old female undergoes a biopsy of a painful, eccentric, lytic lesion in the distal femur which confirms chondromyxoid fibroma.
Which of the following is the most appropriate definitive management?
Which of the following is the most appropriate definitive management?
Explanation
Chondromyxoid fibroma is a locally aggressive benign tumor. The gold standard treatment is extended intralesional curettage using a high-speed burr, followed by bone grafting or cementation.
Question 10
A 2-year-old child presents with severe developmental delay, corneal clouding, and flexion contractures of the fingers. Radiographs of the spine demonstrate anterior beaking of the lumbar vertebral bodies.
Deficiency of which of the following enzymes is responsible for this condition?
Deficiency of which of the following enzymes is responsible for this condition?
Explanation
Hurler syndrome (MPS I) features severe cognitive decline, corneal clouding, trigger digits, and anterior vertebral beaking. It is caused by an autosomal recessive deficiency of alpha-L-iduronidase.
Question 11
A 7-year-old boy presents to the orthopedic clinic with a waddling gait. Examination reveals hypermobility of his shoulders, allowing them to be approximated anteriorly in the midline. Pelvic radiographs show bilateral coxa vara and widened pubic symphysis. What is the genetic mutation associated with this syndrome?
Explanation
Cleidocranial dysplasia is characterized by absent or hypoplastic clavicles, delayed skull suture closure, supernumerary teeth, and coxa vara. It is caused by a mutation in the RUNX2 (CBFA1) gene, essential for osteoblast differentiation.
Question 12
A biopsy of a destructive diaphyseal lesion in the femur of a 16-year-old boy shows small round blue cells. Immunohistochemistry is strongly positive for CD45 and CD20, but negative for CD99 and FLI-1. What is the most appropriate systemic treatment for this condition?
Explanation
The immunohistochemistry profile (CD45+, CD20+, CD99-) indicates a primary diffuse large B-cell lymphoma of bone, not Ewing sarcoma. The standard systemic chemotherapy regimen is R-CHOP.
Question 13
A 10-year-old girl complains of bilateral knee and hip pain after activity. Radiographs reveal delayed, irregular ossification of the capital femoral epiphyses and a double-layered appearance of the patellae on a lateral knee radiograph. Intelligence and facial features are normal. What gene mutation is most commonly responsible?
Explanation
Multiple Epiphyseal Dysplasia (MED) presents with irregular epiphyses and classic 'double-layered' patellae, without spine involvement or cognitive deficits. It is most commonly caused by a mutation in the Cartilage Oligomeric Matrix Protein (COMP) gene.
Question 14
A newborn is noted to have rhizomelic shortening of the limbs, frontal bossing, and midface hypoplasia. Radiographs show decreasing interpedicular distances from the upper to the lower lumbar spine. The mutation responsible for this condition primarily affects which specific zone of the physis?
Explanation
Achondroplasia is caused by a gain-of-function mutation in FGFR3, which inhibits normal chondrocyte proliferation. This directly leads to a defect in the proliferative zone of the growth plate.
Question 15
An 18-year-old male presents with bilateral lower extremity aching pain and fatigue with walking. Radiographs demonstrate marked symmetric cortical thickening of the diaphyseal regions of the femur and tibia, with obliteration of the medullary canal.
Which of the following is true regarding his condition?
Which of the following is true regarding his condition?
Explanation
Progressive diaphyseal dysplasia (Camurati-Engelmann disease) is an autosomal dominant disorder characterized by thickened diaphyses and muscle weakness. It is associated with a mutation in the TGFB1 gene.
Question 16
A 19-year-old patient presents with pain in the proximal tibia. Imaging demonstrates a sharply demarcated, eccentric, radiolucent lesion in the metaphysis extending towards the diaphysis, without true epiphyseal involvement.
Histology reveals a lobular architecture with central myxoid tissue and hypercellular peripheries containing multinucleated giant cells. Which is the most likely diagnosis?
Histology reveals a lobular architecture with central myxoid tissue and hypercellular peripheries containing multinucleated giant cells. Which is the most likely diagnosis?
Explanation
The location (eccentric, metaphyseal) and histology (lobular pattern with myxoid centers and hypercellular peripheries with giant cells) are classic for Chondromyxoid Fibroma.
Question 17
A 45-year-old male presents with deep, aching thigh pain. Imaging shows a permeative lesion in the femoral diaphysis with a large soft tissue mass. Biopsy reveals sheets of atypical lymphoid cells. Which immunohistochemical marker is most likely positive in this primary bone tumor?
Explanation
Primary bone lymphoma is most commonly a Diffuse Large B-Cell Lymphoma (DLBCL). These tumor cells strongly express B-cell markers such as CD20 and CD79a, alongside CD45 (LCA). CD99 is typically associated with Ewing sarcoma, which presents in a younger demographic.
Question 18
A 6-year-old boy presents with short stature, severe genu valgum, and corneal clouding, but displays normal intelligence. Radiographs reveal generalized platyspondyly and marked odontoid hypoplasia. Which of the following is the specific enzyme deficient in this patient's condition?
Explanation
This patient has Morquio syndrome A (MPS IV A), characterized by normal intelligence, severe skeletal dysplasia, and profound cervical instability due to odontoid hypoplasia. It is caused by a deficiency in N-acetylgalactosamine-6-sulfatase.
Question 19
Unlike most other mucopolysaccharidoses, which typically follow an autosomal recessive inheritance pattern, which of the following is inherited in an X-linked recessive manner?
Explanation
Hunter syndrome (MPS II) is the only mucopolysaccharidosis with an X-linked recessive inheritance pattern. All other major MPS types are inherited in an autosomal recessive fashion.
Question 20
A 55-year-old male presents with thigh pain. Radiographs show a permeative diaphyseal lesion with minimal cortical destruction. MRI reveals a massive soft tissue component. Biopsy confirms CD20+ atypical lymphoid cells. What is the most appropriate primary management?
Explanation
Primary lymphoma of bone typically presents with a large soft tissue mass despite relatively subtle destructive changes on radiographs. The mainstay of treatment is systemic multi-agent chemotherapy combined with local external beam radiation.
Question 21
A 9-year-old child presents with a waddling gait and aching leg pain. Radiographs show bilateral, symmetric cortical thickening of the femoral and tibial diaphyses with sparing of the epiphyses. Genetic testing is most likely to reveal a mutation in which gene?
Explanation
The clinical and radiographic presentation is classic for progressive diaphyseal dysplasia (Camurati-Engelmann disease). This autosomal dominant condition is caused by mutations in the TGFB1 gene.
Question 22
A 20-year-old male presents with chronic knee pain. Radiographs demonstrate an eccentric, well-circumscribed, lytic lesion with a sclerotic margin in the proximal tibial metaphysis. Biopsy reveals lobules of spindle or stellate cells in a myxoid background separated by highly cellular fibrous bands containing osteoclast-like giant cells. What is the most likely diagnosis?
Explanation
Chondromyxoid fibroma typically presents as an eccentric, lytic metaphyseal lesion. The classic histologic appearance consists of lobules of myxoid and chondroid tissue separated by fibrous septa containing multinucleated giant cells.
Question 23
Regarding the surgical treatment of a large, symptomatic chondromyxoid fibroma of the proximal tibia in a young adult, what is the most appropriate definitive management?
Explanation
Chondromyxoid fibroma has a high recurrence rate (up to 25%) if treated with simple curettage alone. Extended intralesional curettage with a high-speed burr and local adjuvants (phenol, cryotherapy) followed by grafting or PMMA is the standard of care.
Question 24
A 45-year-old woman is evaluated for a destructive diaphyseal lesion in the humerus. Histology reveals a diffuse infiltrate of small to medium-sized round blue cells. Immunohistochemistry is positive for CD45 (LCA) and CD20, but negative for CD99 and cytokeratin. Which diagnosis is confirmed?
Explanation
Primary lymphoma of bone is a round blue cell tumor that stains positive for CD45 (Leukocyte Common Antigen) and B-cell markers like CD20. It is negative for CD99 (Ewing sarcoma) and cytokeratin (metastatic carcinoma).
Question 25
A 2-year-old presents with coarse facial features, hepatosplenomegaly, and a progressive thoracolumbar kyphosis. Radiographs reveal thick, paddle-shaped ribs and hypoplastic "bullet-shaped" vertebral bodies. Enzyme analysis shows a deficiency of alpha-L-iduronidase. Which of the following best describes this syndrome?
Explanation
Hurler syndrome (MPS I) is characterized by coarse facies, dysostosis multiplex, intellectual disability, and alpha-L-iduronidase deficiency. Bullet-shaped vertebrae and paddle-shaped ribs are classic radiographic findings of dysostosis multiplex.
Question 26
A 5-year-old with Morquio syndrome (MPS IV) is scheduled for elective bilateral lower extremity osteotomies for severe genu valgum. Prior to intubation and anesthesia, which of the following is the most critical radiographic screening required?
Explanation
Patients with Morquio syndrome have severe odontoid hypoplasia and ligamentous laxity, leading to atlantoaxial instability. Flexion-extension C-spine radiographs are mandatory prior to any procedure requiring intubation to prevent catastrophic spinal cord injury.
Question 27
A 12-year-old boy is diagnosed with Camurati-Engelmann disease based on classic radiographic findings of bilateral femoral diaphyseal thickening and a confirmed TGFB1 mutation. He reports severe, debilitating leg pain and progressive muscle weakness. Which of the following is the most effective medical therapy for his symptoms?
Explanation
Systemic corticosteroids are the mainstay of medical treatment for symptomatic Camurati-Engelmann disease. They have been shown to significantly decrease bone pain, improve muscle strength, and in some cases, reverse the abnormal radiographic findings.
Question 28
A 4-year-old boy presents with a painless, asymmetric swelling on the medial aspect of his ankle. Radiographs show an irregular, ossified mass arising from the medial epiphysis of the distal tibia. Histologically, the lesion strongly resembles an osteochondroma. What is the most likely diagnosis?
Explanation
Dysplasia epiphysealis hemimelica (Trevor disease) is characterized by an osteochondroma-like outgrowth arising from the epiphysis, most commonly on the medial side of the knee or ankle. It results in asymmetric epiphyseal enlargement and joint deformity.
Question 29
When differentiating a chondromyxoid fibroma from a chondroblastoma based on standard radiographic presentation in a skeletally immature patient, which of the following features most strongly favors a diagnosis of chondroblastoma?
Explanation
In a skeletally immature patient, a chondroblastoma is classically located within the epiphysis (or apophysis). Chondromyxoid fibroma, conversely, is almost always found in the metaphysis.
Question 30
A 48-year-old male presents with severe right thigh pain. Plain radiographs appear largely unremarkable except for a very subtle permeative radiolucency in the diaphysis. MRI demonstrates extensive marrow replacement and a massive soft tissue mass surrounding the bone. Which of the following is the most likely diagnosis?
Explanation
The combination of minimal cortical destruction on plain radiographs with an extensive soft tissue mass on MRI is a hallmark presentation of primary lymphoma of bone. The tumor permeates through the Haversian canals without completely destroying the cortex.
Question 31
A 4-year-old girl with Hurler syndrome presents with bilateral stiffness and contractures of her fingers. On examination, she has multiple trigger digits. What is the primary pathophysiologic cause of the trigger digits in this patient population?
Explanation
Trigger digits in patients with mucopolysaccharidoses (like Hurler syndrome) are caused by the direct infiltration and accumulation of glycosaminoglycans within the flexor tendons and tenosynovium, causing an intrinsic size mismatch with the pulley system.
Question 32
A 6-year-old girl is noted to have early breast development and vaginal bleeding. She complains of left hip pain, and radiographs reveal a ground-glass, expansile lytic lesion in the proximal femur with a "shepherd's crook" deformity. Physical exam reveals large, irregular hyperpigmented skin macules. A mutation in which of the following genes is responsible for this condition?
Explanation
This patient has McCune-Albright syndrome, characterized by polyostotic fibrous dysplasia, precocious puberty, and cafe-au-lait spots. It is caused by an activating post-zygotic mutation in the GNAS1 gene, resulting in persistent adenylyl cyclase activity.
Question 33
A newborn presents with micromelic shortening of the limbs, severe clubfeet, rigid "hitchhiker" thumbs, and cystic swelling of the pinnae. Radiographs show a first metacarpal that is short and oval-shaped. Which of the following is the defective cellular process in this dysplasia?
Explanation
The clinical description is pathognomonic for diastrophic dysplasia (hitchhiker thumb, cauliflower ear, severe clubfeet). This is caused by a mutation in the SLC26A2 gene, which encodes a transmembrane sulfate transporter essential for cartilage matrix sulfation.
Question 34
A 14-year-old boy presents for evaluation of shoulder hypermobility. He is able to touch his shoulders together anteriorly. Examination reveals a large, open anterior fontanelle and retained deciduous teeth. He is at increased risk for developing which of the following orthopedic conditions?
Explanation
This patient has cleidocranial dysplasia (RUNX2 mutation), characterized by hypoplastic/absent clavicles, delayed fontanelle closure, and delayed dental eruption. Orthopedically, these patients have a high incidence of progressive developmental coxa vara.
Question 35
A 5-year-old boy presents with progressive joint stiffness, coarse facial features, and hepatosplenomegaly. An ophthalmologic exam reveals clear corneas. His maternal uncle had similar clinical features and died of cardiac failure in his twenties. Which of the following enzyme deficiencies is most likely responsible for this condition?
Explanation
This patient has Hunter syndrome (MPS II), which is unique among mucopolysaccharidoses because it is inherited in an X-linked recessive pattern and features clear corneas. It is caused by a deficiency in iduronate-2-sulfatase.
Question 36
A 6-year-old girl with Morquio syndrome (MPS IV) presents with progressive weakness and clumsiness in her hands. Cervical spine flexion-extension radiographs demonstrate severe atlantoaxial instability. What is the primary anatomic cause of this instability in Morquio syndrome?
Explanation
Atlantoaxial instability in Morquio syndrome (MPS IV) is driven by a combination of severe odontoid hypoplasia and profound ligamentous laxity. This places patients at high risk for fatal cervicomedullary compression if not addressed with surgical fusion.
Question 37
An 8-year-old boy presents with a waddling gait and severe, deep, aching bone pain in both legs. Radiographs demonstrate symmetrical, dense cortical thickening of the bilateral femoral and tibial diaphyses, sparing the epiphyses.
Genetic testing would most likely reveal a mutation in which of the following genes?
Genetic testing would most likely reveal a mutation in which of the following genes?
Explanation
The clinical and radiographic presentation is classic for Progressive Diaphyseal Dysplasia (Camurati-Engelmann disease). This condition is inherited in an autosomal dominant fashion and is caused by mutations in the TGFB1 gene.
Question 38
A 22-year-old male presents with persistent left knee pain. Radiographs reveal an eccentric, purely lytic lesion in the proximal tibial metaphysis with a distinct sclerotic inner margin.
A biopsy demonstrates lobules of myxoid and chondroid tissue with hypercellular peripheries. What is the most likely diagnosis?
A biopsy demonstrates lobules of myxoid and chondroid tissue with hypercellular peripheries. What is the most likely diagnosis?
Explanation
Chondromyxoid fibroma (CMF) is a rare, benign cartilage tumor that classically presents as an eccentric metaphyseal radiolucency with a sclerotic inner margin. Histologically, it features biphasic lobules with hypocellular centers and hypercellular peripheries containing stellate cells.
Question 39
A 55-year-old male presents with thigh pain. Radiographs show a large permeative, 'moth-eaten' lesion in the femoral diaphysis with minimal cortical expansion.
Biopsy confirms primary diffuse large B-cell lymphoma of bone. What is the standard definitive treatment?
Biopsy confirms primary diffuse large B-cell lymphoma of bone. What is the standard definitive treatment?
Explanation
Primary bone lymphoma is highly responsive to non-operative treatment. The standard of care is systemic multidrug chemotherapy (e.g., CHOP-R) combined with localized external beam radiotherapy, reserving surgery strictly for impending or actual pathologic fractures.
Question 40
A 3-year-old child presents with coarse facies, corneal clouding, and a thoracolumbar kyphosis. Radiographs of the hands demonstrate proximal pointing of the metacarpals.
Which enzyme is most likely deficient in this patient?
Which enzyme is most likely deficient in this patient?
Explanation
The clinical features and 'bullet-shaped' (proximally pointed) metacarpals are classic for Hurler syndrome (MPS I). This disorder is caused by a deficiency in the enzyme alpha-L-iduronidase.
Question 41
A 10-year-old girl is diagnosed with Progressive Diaphyseal Dysplasia (Camurati-Engelmann disease). She complains of debilitating bone pain in her bilateral lower extremities. Which of the following is the most appropriate first-line medical therapy to alleviate her symptoms?
Explanation
Systemic corticosteroids are the mainstay of medical treatment for the severe bone pain associated with Camurati-Engelmann disease. They decrease bone turnover, reduce pain, and can improve the characteristic waddling gait.
Question 42
Which histologic feature is considered the hallmark of a chondromyxoid fibroma, aiding in differentiating it from chondrosarcoma?
Explanation
Chondromyxoid fibroma exhibits a distinct pseudo-lobular pattern with central hypocellular myxoid tissue and hypercellular peripheries containing multinucleated giant cells. Chondrosarcomas typically lack this organized lobular zonation and show permeation of native bone.
Question 43
A classic imaging characteristic that strongly suggests primary bone lymphoma over other aggressive sarcomas (such as Ewing sarcoma or osteosarcoma) is:
Explanation
Primary bone lymphoma often presents with a massive soft-tissue component that seems disproportionately large compared to the relatively preserved cortical bone structure. The tumor typically spreads through Haversian canals without completely destroying the cortex.
Question 44
In a patient with achondroplasia, what is the most common cause of sudden death in infancy or early childhood?
Explanation
Infants with achondroplasia have a narrowed foramen magnum due to abnormal endochondral ossification of the skull base. This stenosis can cause cervicomedullary compression, leading to central apnea and sudden death if not decompressed surgically.
Question 45
A newborn is diagnosed with Spondyloepiphyseal Dysplasia congenita (SEDc). Which of the following best describes the underlying genetic defect and the typical associated clinical finding?
Explanation
SED congenita is caused by mutations in the COL2A1 gene, affecting Type II collagen production. Because Type II collagen is abundant in the vitreous humor of the eye, these patients frequently suffer from severe myopia and are at high risk for retinal detachment.
Question 46
A 9-year-old boy with normal intelligence and normal facial features presents with joint pain and a waddling gait. Lateral radiographs of his knees reveal a 'double-layer' patella. What is the most likely diagnosis?
Explanation
The 'double-layer' patella is a classic radiographic sign for Multiple Epiphyseal Dysplasia (MED). MED is most commonly caused by mutations in the Cartilage Oligomeric Matrix Protein (COMP) gene.
Question 47
Which of the following Mucopolysaccharidoses (MPS) is characterized by severe, progressive intellectual disability and profound central nervous system deterioration, but relatively mild somatic and orthopedic manifestations?
Explanation
Sanfilippo syndrome (MPS III) primarily affects the central nervous system, leading to severe behavioral issues and cognitive decline. Somatic features such as dwarfism, skeletal dysplasias, and joint stiffness are much milder compared to other MPS types.
Question 48
What is the recommended surgical management for a symptomatic chondromyxoid fibroma in the proximal tibia of a 25-year-old patient?
Explanation
Chondromyxoid fibroma is a benign but locally aggressive tumor. The standard of care is extended intralesional curettage utilizing a high-speed burr (with or without local adjuvants) followed by bone grafting or cementation.
Question 49
A patient with Hurler syndrome develops a severe thoracolumbar kyphosis (gibbus deformity). What is the primary radiographic abnormality of the vertebrae causing this deformity?
Explanation
In Hurler syndrome (MPS I), the vertebrae typically exhibit anteroinferior beaking, which leads to anterior wedging and progressive thoracolumbar kyphosis. In contrast, Morquio syndrome (MPS IV) classically features central anterior beaking.
Question 50
Which of the following enzyme deficiencies differentiates Morquio A syndrome from Morquio B syndrome?
Explanation
Morquio A (MPS IVA) is caused by a deficiency in galactose-6-sulfatase, while the much rarer Morquio B (MPS IVB) is caused by a deficiency in beta-galactosidase. Both result in the inability to degrade keratan sulfate, leading to similar skeletal manifestations.
Question 51
During the immunohistochemical evaluation of a suspected primary bone lymphoma biopsy, which of the following surface markers is most likely to be strongly positive?
Explanation
The vast majority of primary bone lymphomas are diffuse large B-cell lymphomas. Therefore, they will strongly express B-cell markers such as CD20, along with the leukocyte common antigen CD45.
Question 52
A 60-year-old male is undergoing staging for a newly diagnosed primary diffuse large B-cell lymphoma of the humerus. He presents to the emergency department with a displaced pathologic fracture through the lesion. What is the most appropriate management sequence?
Explanation
While uncomplicated primary bone lymphoma is treated medically, the presence of a displaced pathologic fracture necessitates prompt surgical stabilization. Post-operatively, the patient must proceed with the standard curative regimen of systemic chemotherapy and local radiation.
Question 53
Which of the following clinical or radiographic features best distinguishes Ribbing disease from Camurati-Engelmann disease (Progressive Diaphyseal Dysplasia)?
Explanation
Ribbing disease (multiple diaphyseal sclerosis) closely resembles Camurati-Engelmann disease radiographically but usually presents after puberty with unilateral or asymmetric diaphyseal sclerosis. Camurati-Engelmann disease presents in childhood with symmetric, bilateral involvement.
Question 54
When evaluating a patient with a known mucopolysaccharidosis, which clinical feature reliably helps distinguish Morquio syndrome (MPS IV) from Hurler syndrome (MPS I)?
Explanation
Patients with Morquio syndrome (MPS IV) typically have preserved, normal intelligence, despite profound skeletal dysplasias. In contrast, Hurler syndrome (MPS I) is characterized by progressive and severe cognitive decline.
Question 55
A 4-year-old boy presents with progressive joint stiffness, coarse facial features, and hepatosplenomegaly. His maternal uncle had a similar presentation and passed away in his twenties. There is no corneal clouding. Which of the following is the most likely deficient enzyme?
Explanation
Hunter syndrome (MPS II) is characterized by X-linked recessive inheritance, explaining the maternal uncle's history, and the absence of corneal clouding. It is caused by a deficiency of iduronate-2-sulfatase.
Question 56
A 6-year-old child with normal intelligence presents with short stature, severe genu valgum, and a barrel chest. Radiographs reveal platyspondyly with central anterior vertebral beaking.
Which of the following is the most critical screening evaluation prior to any surgical intervention?
Which of the following is the most critical screening evaluation prior to any surgical intervention?
Explanation
The clinical presentation and central vertebral beaking are classic for Morquio syndrome (MPS IV). These patients are at high risk for fatal atlantoaxial instability due to odontoid hypoplasia, necessitating cervical spine screening prior to anesthesia.
Question 57
A 12-year-old boy complains of bilateral leg pain and a waddling gait. Radiographs show symmetrical cortical thickening of the bilateral femoral and tibial diaphyses, sparing the epiphyses.
Mutation in which of the following genes is responsible for this condition?
Mutation in which of the following genes is responsible for this condition?
Explanation
The patient's presentation and images are characteristic of Camurati-Engelmann disease (Progressive Diaphyseal Dysplasia). It is inherited in an autosomal dominant pattern and is caused by a mutation in the TGFB1 gene.
Question 58
A 55-year-old man presents with dull, aching thigh pain for 3 months. Radiographs demonstrate a permeative, moth-eaten radiolucent lesion in the femoral diaphysis with minimal periosteal reaction.
Biopsy reveals sheets of uniform, small round blue cells. Immunohistochemistry is positive for CD20 and CD45. What is the standard initial treatment?
Biopsy reveals sheets of uniform, small round blue cells. Immunohistochemistry is positive for CD20 and CD45. What is the standard initial treatment?
Explanation
The diagnosis is primary bone lymphoma (diffuse large B-cell lymphoma), supported by the permeative lesion, age, and CD20/CD45 positivity. The primary treatment is multi-agent chemotherapy (e.g., R-CHOP) combined with localized radiation; surgery is reserved for impending or actual pathologic fractures.
Question 59
A 6-year-old child presents with severe disproportionate short-trunk dwarfism, knock-knees, and normal intelligence. Radiographs reveal platyspondyly and odontoid hypoplasia. Laboratory analysis confirms a diagnosis of Morquio syndrome (MPS IV). Which of the following is the deficient enzyme in Type A of this disorder?
Explanation
Morquio syndrome Type A is an autosomal recessive mucopolysaccharidosis caused by a deficiency in galactosamine-6-sulfatase. Unlike most other MPS types, intelligence is preserved, but severe skeletal deformities and atlantoaxial instability are hallmarks.
Question 60
A 60-year-old male presents with deep thigh pain.
Biopsy reveals sheets of uniform, small to medium-sized cells with prominent nucleoli. The cells are positive for CD45 and CD20. Which of the following immunohistochemical markers is also most likely to be positive, confirming the diagnosis?
Biopsy reveals sheets of uniform, small to medium-sized cells with prominent nucleoli. The cells are positive for CD45 and CD20. Which of the following immunohistochemical markers is also most likely to be positive, confirming the diagnosis?

Explanation
Primary bone lymphoma is most commonly a diffuse large B-cell lymphoma (DLBCL). These tumors typically express B-cell markers such as CD20, CD45 (LCA), and PAX5, distinguishing them from other small round blue cell tumors.
Question 61
A 35-year-old patient presents with chronic, asymmetric limb pain and joint stiffness. Radiographs show dense, irregular cortical hyperostosis extending along the diaphysis of the femur, resembling 'dripping candle wax'. Which gene mutation is most commonly associated with this condition?
Explanation
The described condition is melorheostosis, characterized radiographically by a 'dripping candle wax' appearance of the cortex. It is associated with a loss-of-function mutation in the LEMD3 gene.
Question 62
A 16-year-old male presents with knee pain. Radiographs reveal an eccentric, lytic lesion with a sclerotic margin in the proximal tibial metaphysis.
Which of the following is the hallmark histological feature of this lesion?
Which of the following is the hallmark histological feature of this lesion?
Explanation
Chondromyxoid fibroma exhibits a lobular pattern of stellate or spindle-shaped cells within a myxoid and chondroid background. The periphery of these lobules is highly cellular and typically contains osteoclast-like giant cells.
Question 63
A 1-year-old infant presents with corneal clouding, hepatosplenomegaly, mental retardation, and a noticeable gibbus deformity of the thoracolumbar spine. What is the deficient enzyme responsible for this clinical presentation?
Explanation
This presentation is classic for Hurler syndrome (MPS I), an autosomal recessive disorder. It is caused by a deficiency in alpha-L-iduronidase, leading to the accumulation of dermatan and heparan sulfate.
Question 64
A 12-year-old girl with a known TGFB1 mutation presents with severe bilateral leg pain, muscle weakness, and a waddling gait.
Radiographs confirm progressive diaphyseal dysplasia (Camurati-Engelmann disease). Which pharmacological treatment is considered first-line to improve her symptoms and walking tolerance?
Radiographs confirm progressive diaphyseal dysplasia (Camurati-Engelmann disease). Which pharmacological treatment is considered first-line to improve her symptoms and walking tolerance?

Explanation
Corticosteroids are the mainstay of medical treatment for symptomatic Camurati-Engelmann disease. They effectively relieve bone pain, improve muscle strength, and increase exercise tolerance.
Question 65
A 45-year-old male completes definitive radiation therapy for primary diffuse large B-cell lymphoma of the femoral diaphysis. Which of the following is the most significant orthopedic complication directly associated with treating appendicular primary bone lymphoma exclusively with local high-dose radiation?
Explanation
Radiation therapy alone for primary bone lymphoma in weight-bearing bones carries a high risk of subsequent pathologic fracture due to radiation-induced osteonecrosis and delayed bone remodeling. This has shifted modern paradigms toward combined chemoradiation or prophylactic stabilization.
Question 66
A 5-year-old child with a known deficiency of galactosamine-6-sulfatase requires general anesthesia for a hernia repair. Which pre-operative orthopedic evaluation is absolutely critical before intubation?
Explanation
Patients with Morquio syndrome (MPS IV) frequently have odontoid hypoplasia resulting in severe atlantoaxial instability. Flexion-extension cervical spine radiographs are mandatory before any procedure requiring intubation to prevent spinal cord injury.
Question 67
A 22-year-old female undergoes a core needle biopsy of an eccentric, lytic metaphyseal lesion in the distal femur. The pathology report confirms chondromyxoid fibroma. What is the most appropriate surgical treatment to minimize recurrence?
Explanation
Chondromyxoid fibroma is a benign but locally aggressive tumor with a high recurrence rate if treated with simple curettage. Extended intralesional curettage with high-speed burring and adjuvant treatment (e.g., phenol, cement) is the gold standard.
Question 68
A 7-year-old boy presents with profound intellectual disability, severe hyperactivity, and speech delay. Physical examination reveals mild coarse facial features but minimal skeletal abnormalities (mild dysostosis multiplex). He lacks corneal clouding. Which of the following mucopolysaccharidoses is the most likely diagnosis?
Explanation
Sanfilippo syndrome (MPS III) is characterized by severe central nervous system degeneration (profound mental retardation and hyperactivity) with relatively mild somatic and skeletal features compared to other MPS disorders.
Question 69
A 28-year-old male presents with a permeative lytic lesion of the humerus. A biopsy yields a small round blue cell tumor. The pathologist performs a reticulin stain to help differentiate between primary bone lymphoma and Ewing sarcoma. What is the classic reticulin staining pattern for primary bone lymphoma?
Explanation
In primary bone lymphoma, reticulin staining typically highlights a dense network of fibers surrounding individual tumor cells. In contrast, Ewing sarcoma shows reticulin fibers surrounding groups or nests of cells rather than individual cells.
Question 70
A 3-year-old child presents with a short trunk, prominent chest, and coxa vara. Ophthalmologic exam reveals high myopia. Radiographs show delayed ossification of the epiphyses and platyspondyly. The genetic defect underlying this condition primarily affects which of the following?
Explanation
The clinical picture describes spondyloepiphyseal dysplasia congenita (SEDC), which is caused by a mutation in the COL2A1 gene. This affects Type II collagen, a major structural component of both articular cartilage and the vitreous humor.
Question 71
A newborn is noted to have severe micromelia, bilateral clubfeet, hitchhiker thumbs, and swelling of the external ear auricles (cauliflower ears). Which of the following genes is mutated in this condition?
Explanation
Diastrophic dysplasia is an autosomal recessive disorder caused by a mutation in the SLC26A2 (DTDST) gene, which encodes a sulfate transporter. Hallmark features include hitchhiker thumbs, cauliflower ears, and severe clubfeet.
Question 72
A 10-year-old girl with normal intelligence presents with severe corneal clouding, heart valve abnormalities, and joint stiffness.
Radiographs demonstrate classic dysostosis multiplex. Laboratory testing reveals an accumulation of dermatan sulfate only. Which enzyme is deficient?
Radiographs demonstrate classic dysostosis multiplex. Laboratory testing reveals an accumulation of dermatan sulfate only. Which enzyme is deficient?
Explanation
Maroteaux-Lamy syndrome (MPS VI) is characterized by severe skeletal changes, corneal clouding, and preserved intelligence. It is caused by a deficiency in arylsulfatase B, leading solely to dermatan sulfate accumulation.
Question 73
Which of the following radiographic features is most reliable for distinguishing a chondromyxoid fibroma from a chondroblastoma in the long bones of a skeletally immature patient?
Explanation
Anatomic location is a key differentiator: chondroblastomas classically arise in the epiphysis or apophysis, whereas chondromyxoid fibromas are typically eccentrically located in the metaphysis.
Question 74
A 14-year-old boy presents for evaluation of frequent shoulder dislocations. Examination reveals he can touch his shoulders together in the midline. Dental examination shows delayed eruption of secondary teeth. The underlying mutation involves a transcription factor essential for which of the following cellular processes?
Explanation
The patient has cleidocranial dysplasia, caused by a mutation in RUNX2 (CBFA1). RUNX2 is a master transcription factor required for osteoblast differentiation and is crucial for intramembranous ossification (clavicles, cranium).
Question 75
A 9-year-old child presents with severe leg pain, waddling gait, and profound muscle weakness. Radiographs demonstrate bilateral symmetric cortical thickening of the long bone diaphyses with sparing of the epiphyses and metaphyses.
Which of the following medications is considered first-line for relieving symptoms and improving strength in this condition?
Which of the following medications is considered first-line for relieving symptoms and improving strength in this condition?
Explanation
This patient has Progressive Diaphyseal Dysplasia (Camurati-Engelmann disease), caused by a TGF-beta-1 mutation. Systemic corticosteroids are the first-line treatment as they successfully relieve bone pain and improve muscle strength.
Question 76
A 6-year-old boy presents with short trunk dwarfism, normal intelligence, and severe genu valgum. Spine radiographs demonstrate universal platyspondyly with central anterior vertebral beaking. He is diagnosed with Mucopolysaccharidosis Type IV (Morquio syndrome). Which specific enzyme is deficient in this patient?
Explanation
Morquio syndrome (MPS IV) is caused by a deficiency in Galactosamine-6-sulfatase (Type A) or Beta-galactosidase (Type B), leading to keratan sulfate accumulation. It uniquely features normal intelligence and central anterior vertebral beaking.
Question 77
A 60-year-old man presents with dull thigh pain. Plain radiographs show a subtle permeative osteolytic lesion in the femoral diaphysis with minimal periosteal reaction. MRI reveals extensive marrow replacement extending far beyond the radiographic abnormalities.
Histological evaluation of a core biopsy will most likely reveal cells that strongly express which of the following markers?
Histological evaluation of a core biopsy will most likely reveal cells that strongly express which of the following markers?
Explanation
The clinical and imaging findings are highly characteristic of primary bone lymphoma, often appearing as a 'ghost tumor' with extensive MRI marrow involvement. Primary bone lymphoma is typically a diffuse large B-cell lymphoma, which strongly expresses the B-cell marker CD20.
Question 78
A 22-year-old presents with chronic proximal tibial pain. Radiographs demonstrate a well-defined, eccentric, lucent metaphyseal lesion with a sclerotic rim.
Biopsy shows lobules of myxoid tissue separated by fibrous septa containing giant cells. What is the recommended treatment?
Biopsy shows lobules of myxoid tissue separated by fibrous septa containing giant cells. What is the recommended treatment?
Explanation
The diagnosis is a chondromyxoid fibroma (CMF), a rare benign cartilage tumor. The standard treatment is intralesional extended curettage (using a high-speed burr) followed by bone grafting or cementation to minimize the risk of local recurrence.
Question 79
A 2-year-old girl is evaluated for coarse facial features, corneal clouding, developmental delay, and severe kyphosis. Spine radiographs show anterior-inferior vertebral body beaking.
The accumulation of which glycosaminoglycans is primarily responsible for her clinical presentation?
The accumulation of which glycosaminoglycans is primarily responsible for her clinical presentation?
Explanation
The patient has Hurler syndrome (MPS I), caused by alpha-L-iduronidase deficiency. This leads to the toxic accumulation of heparan sulfate and dermatan sulfate, resulting in severe skeletal dysplasia, corneal clouding, and mental retardation.
Question 80
A 12-year-old boy presents with profound bilateral leg pain and fatigue. Radiographs show pronounced cortical thickening of the bilateral femoral diaphyses with sparing of the epiphyses and metaphyses.
What is the mode of inheritance for this disorder?
What is the mode of inheritance for this disorder?

Explanation
Progressive diaphyseal dysplasia (Camurati-Engelmann disease) is inherited in an autosomal dominant pattern. It is caused by mutations in the TGF-beta-1 gene, leading to excessive bone formation in the long bone diaphyses.
Question 81
A 45-year-old male is diagnosed with primary diffuse large B-cell lymphoma of the humerus based on an image-guided core needle biopsy. The cortical continuity is preserved, and the calculated Mirels score is 6. What is the most appropriate initial management?
Explanation
The primary treatment for primary bone lymphoma (diffuse large B-cell) is multi-agent chemotherapy (such as R-CHOP) with or without consolidative radiation. Surgery is strictly reserved for actual or impending fractures, which are unlikely with a Mirels score of 6.
Question 82
An 8-year-old boy with known Morquio syndrome (MPS IV) is scheduled for bilateral lower extremity corrective osteotomies to address severe genu valgum. Before general anesthesia is administered, which of the following is the most critical pre-operative orthopedic evaluation?
Explanation
Patients with Morquio syndrome (MPS IV) classically suffer from odontoid hypoplasia and ligamentous laxity, making them highly susceptible to atlantoaxial instability. Flexion-extension cervical radiographs (or MRI) are critical prior to intubation to prevent catastrophic spinal cord injury.
Question 83
A 7-year-old girl is evaluated for severe short stature, coarse facial features, corneal clouding, and joint contractures. Despite these severe somatic manifestations, her intelligence is completely normal. What is the deficient enzyme in this patient's condition?
Explanation
This presentation describes Maroteaux-Lamy syndrome (MPS VI), which is characterized by normal intelligence but severe somatic features including corneal clouding. It is caused by a deficiency in Arylsulfatase B.
Question 84
A 50-year-old woman complains of persistent knee pain. Plain radiographs show only subtle, ill-defined diaphyseal permeation. MRI reveals uniform low T1 signal replacing the entire distal femoral marrow cavity.
Which core needle biopsy finding would definitively confirm the most likely diagnosis?
Which core needle biopsy finding would definitively confirm the most likely diagnosis?

Explanation
The striking mismatch between minimal plain radiograph findings and extensive MRI marrow replacement is a hallmark of primary bone lymphoma ('ghost tumor'). Biopsy will yield small round blue cells strongly positive for leukocyte common antigen (CD45) and B-cell markers (CD20).
Question 85
Histological examination of a well-defined eccentric lytic proximal tibial lesion from a 19-year-old reveals lobules of myxoid tissue with stellate cells, separated by prominent fibrous septa containing multinucleated giant cells.
When distinguishing this lesion from conventional chondrosarcoma, which classic histological feature is characteristically ABSENT in this benign tumor?
When distinguishing this lesion from conventional chondrosarcoma, which classic histological feature is characteristically ABSENT in this benign tumor?
Explanation
Chondromyxoid fibroma (CMF) lacks abundant mature hyaline cartilage. Its hallmark is lobules of myxoid/chondroid tissue separated by vascularized fibrous septa with giant cells, which helps differentiate it from conventional chondrosarcoma.
Question 86
A 5-year-old boy with a known iduronate-2-sulfatase deficiency (Hunter syndrome) undergoes a comprehensive skeletal survey. Which of the following radiographic findings is most characteristic of the spinal deformities seen in this patient?
Explanation
Hunter syndrome (MPS II) is characterized radiographically by anterior-inferior vertebral body beaking, similar to Hurler syndrome (MPS I). Central anterior beaking is the hallmark of Morquio syndrome (MPS IV).
Question 87
A 24-year-old male presents with a dull ache in his proximal leg. Radiographs demonstrate an eccentric, sharply circumscribed lytic lesion in the proximal tibial metaphysis with a sclerotic margin.
Biopsy demonstrates a lobular arrangement of spindle or stellate cells in an abundant myxoid background, with osteoclast-like giant cells at the lobule periphery. What is the most appropriate definitive management for this lesion?
Biopsy demonstrates a lobular arrangement of spindle or stellate cells in an abundant myxoid background, with osteoclast-like giant cells at the lobule periphery. What is the most appropriate definitive management for this lesion?
Explanation
The clinical, radiographic, and histologic findings are diagnostic of a chondromyxoid fibroma. Due to a recurrence rate of up to 25% with simple curettage, the standard of care is extended intralesional curettage using a high-speed burr and local adjuvants (e.g., phenol, argon beam), followed by bone grafting or cementing.
Question 88
A 6-year-old girl presents with short-trunk dwarfism, severe genu valgum, and generalized joint hyperlaxity. She has normal intelligence but exhibits corneal clouding. Cervical spine radiographs reveal odontoid hypoplasia with significant atlantoaxial instability.
Which of the following glycosaminoglycans abnormally accumulates in this patient's specific syndrome?
Which of the following glycosaminoglycans abnormally accumulates in this patient's specific syndrome?
Explanation
The patient's presentation of short-trunk dwarfism, normal intelligence, joint hyperlaxity, and odontoid hypoplasia is classic for Morquio syndrome (Mucopolysaccharidosis Type IV). This condition is caused by a deficiency in galactosamine-6-sulfatase or beta-galactosidase, leading to the specific accumulation of keratan sulfate.
Question 89
A 22-year-old male presents with chronic knee pain. Imaging reveals an eccentric, lytic metaphyseal lesion in the proximal tibia with a sclerotic rim. Biopsy reveals lobules of stellate cells in a myxoid background with hypercellular peripheries containing multinucleated giant cells.
What is the most appropriate definitive management?
What is the most appropriate definitive management?
Explanation
The clinical, radiographic, and histologic descriptions are classic for chondromyxoid fibroma (CMF). The standard of care is extended intralesional curettage with local adjuvants (e.g., high-speed burring, phenol) to minimize recurrence risk.
Question 90
A 6-year-old child presents with severe genu valgum, prominent chest deformity, and normal intelligence. Radiographs demonstrate central anterior beaking of the vertebral bodies and platyspondyly. Which of the following is the most critical orthopedic screening required for this patient to prevent catastrophic neurological injury?
Explanation
This patient has Morquio syndrome (MPS IV), characterized by central vertebral beaking, normal intelligence, and severe skeletal dysplasia. Odontoid hypoplasia and atlantoaxial instability are hallmarks, necessitating careful cervical spine screening to prevent myelopathy.
Question 91
A 45-year-old woman presents with persistent, aching thigh pain not relieved by rest. Radiographs show a permeative, moth-eaten lytic lesion in the femoral diaphysis with minimal periosteal reaction.
Which of the following immunohistochemical markers is most likely to be definitively positive on biopsy?
Which of the following immunohistochemical markers is most likely to be definitively positive on biopsy?
Explanation
The presentation and imaging are typical of primary lymphoma of bone, which predominantly affects adults over 40. The majority are diffuse large B-cell lymphomas, which reliably stain positive for the B-cell markers CD20 and CD45.
Question 92
A 12-year-old boy presents with aching leg pain, severe fatigue, and a waddling gait. Radiographs demonstrate symmetrical cortical thickening of the bilateral femoral and tibial diaphyses, notably sparing the epiphyses.
Which of the following medical treatments has been shown to be most effective in alleviating pain and improving physical function in this condition?
Which of the following medical treatments has been shown to be most effective in alleviating pain and improving physical function in this condition?
Explanation
Progressive diaphyseal dysplasia (Camurati-Engelmann disease) is caused by a TGF-beta 1 mutation. Systemic corticosteroids are the mainstay of medical treatment, effectively reducing pain, decreasing fatigue, and improving gait.
Question 93
A 3-year-old girl is diagnosed with a mucopolysaccharidosis. Radiographs of her thoracolumbar spine demonstrate severe kyphosis (gibbus deformity). Which of the following radiographic features of the spine best distinguishes Hurler syndrome from Morquio syndrome?
Explanation
In Hurler syndrome (MPS I), the anterior vertebral beak is typically located at the anteroinferior aspect of the vertebral body. In contrast, Morquio syndrome (MPS IV) classically presents with a central anterior vertebral beak.
Question 94
A 9-year-old boy presents with bilateral knee and hip pain after activity. He is of normal height but has a waddling gait. Radiographs show delayed, irregular ossification of the capital femoral epiphyses and a classic "double-layer" appearance of the patella on lateral knee radiographs. A mutation in which of the following genes is most likely?
Explanation
The clinical presentation and classic "double-layer" patella strongly suggest Multiple Epiphyseal Dysplasia (MED). The most common mutation associated with MED is in the COMP (Cartilage Oligomeric Matrix Protein) gene, inherited in an autosomal dominant fashion.
Question 95
A 4-year-old child presents with short trunk dwarfism, severe coxa vara, and myopia. Radiographs reveal delayed ossification of the pubic bones, knee epiphyses, and calcaneus. Which collagen type is primarily affected by the underlying genetic mutation in this disorder?
Explanation
Spondyloepiphyseal dysplasia (SED) congenita is an autosomal dominant disorder caused by a mutation in the COL2A1 gene. This mutation specifically disrupts the formation of Type II collagen, which is critical for hyaline cartilage formation.
Question 96
An orthopedic oncologist is performing an incisional biopsy on a 60-year-old man with a destructive diaphyseal humeral lesion suspected to be a primary round blue cell tumor. To definitively diagnose and subclassify primary bone lymphoma, what special tissue handling is absolutely critical?
Explanation
When primary bone lymphoma is highly suspected, submitting fresh, un-decalcified tissue in RPMI medium or saline is crucial to allow for flow cytometry. This enables the evaluation of specific cell surface markers necessary to correctly subclassify the lymphoma.
Question 97
An infant is evaluated in the neonatal intensive care unit for severe short-limb dwarfism. Examination reveals bilateral severe rigid clubfeet, proximally placed "hitchhiker" thumbs, and cystic swelling of the bilateral pinnae. The underlying genetic defect involves an inability to properly transport which of the following?
Explanation
The infant's presentation of cauliflower ears, hitchhiker thumbs, and clubfeet is diagnostic for diastrophic dysplasia. This condition is caused by a mutation in the SLC26A2 (DTDST) gene, which encodes a sulfate transporter, leading to undersulfation of proteoglycans in cartilage.
Question 98
Which of the following descriptions best outlines the most common clinical presentation and radiographic location of a chondromyxoid fibroma?
Explanation
Chondromyxoid fibroma (CMF) is a rare benign bone tumor that typically presents in the second and third decades of life. The classic and most common radiographic location is an eccentric, lytic, well-circumscribed lesion in the metaphysis of the proximal tibia.
Question 99
A 4-year-old girl with achondroplasia presents to the clinic with progressive clumsiness, bilateral lower extremity hyperreflexia, and occasional apneic episodes during sleep. Radiographs confirm normal sagittal and coronal alignment of the thoracolumbar spine. What is the most likely cause of her progressive neurological symptoms?
Explanation
In young children with achondroplasia, abnormal endochondral ossification leads to poor development of the skull base, frequently causing foramen magnum stenosis. This can lead to cervicomedullary compression, presenting with hyperreflexia, sleep apnea, central hypotonia, and potentially sudden death if untreated.
Question 100
A 10-year-old boy presents to a multidisciplinary genetics and orthopedics clinic. He demonstrates profound, progressive intellectual disability, sleep disturbances, and hyperactive behavior. Orthopedic examination reveals only mild joint stiffness and minimal skeletal abnormalities (mild dysostosis multiplex) compared to other children with related metabolic disorders. This phenotype is most characteristic of which type of mucopolysaccharidosis?
Explanation
Sanfilippo syndrome (MPS III) is distinct because it is characterized by severe, progressive central nervous system degeneration and profound intellectual disability. In sharp contrast to other MPS types, the skeletal dysplasias and somatic features are relatively mild.
None
Previous ChapterMaster ABOS Orthopaedic Review: Bone Tumors, Skeletal Dyspl…
Next Chapter Musculoskeletal Tumors: Lipomas, Osteosarcoma, HME for ABOS…

Medically Verified Content by
Prof. Dr. Mohammed Hutaif Clinic
Consultant Orthopedic & Spine Surgeon