ABOS Board Review: Pediatric Orthopedics, Bone Tumors & Skeletal Dysplasias | Part 6
20 Jun 2026
43 min read
25 Views

Key Takeaway
This ABOS board review covers essential pediatric orthopedic pathology, including septic arthritis, osteomyelitis in infants, benign bone tumor (osteoblastoma) characteristics, and a comprehensive overview of skeletal dysplasias. Learn about their clinical presentation, radiographic features, and management strategies for spinal and hip complications. Part 6 focuses on critical diagnostic and treatment principles.
ABOS Board Review: Pediatric Orthopedics, Bone Tumors & Skeletal Dysplasias | Part 6
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 15-year-old boy presents with chronic, dull back pain that is not completely relieved by NSAIDs. Imaging reveals a 3 cm expansile, partially sclerotic lesion in the posterior elements of L3.
Based on the clinical and radiographic findings, which of the following is true regarding this pathology?
Based on the clinical and radiographic findings, which of the following is true regarding this pathology?
Explanation
The clinical and radiographic presentation is classic for an osteoblastoma, which typically affects the posterior elements of the spine and is >2 cm. Unlike osteoid osteomas, the pain is less predictably relieved by NSAIDs, and histology shows loose fibrovascular connective tissue with irregular osteoid.
Question 2
A 17-year-old girl undergoes biopsy of a solitary bone lesion. The photomicrograph is shown below.
The presence of loose fibrovascular connective tissue intermixed with irregular osteoid and normal-appearing mitotic figures most strongly supports which diagnosis?
The presence of loose fibrovascular connective tissue intermixed with irregular osteoid and normal-appearing mitotic figures most strongly supports which diagnosis?
Explanation
The histology describes osteoblastoma, characterized by interlacing trabeculae of osteoid in a loose, highly vascular fibrous stroma. While mitotic figures may be present, the lack of atypical mitoses and absence of permeative destruction helps differentiate it from osteosarcoma.
Question 3
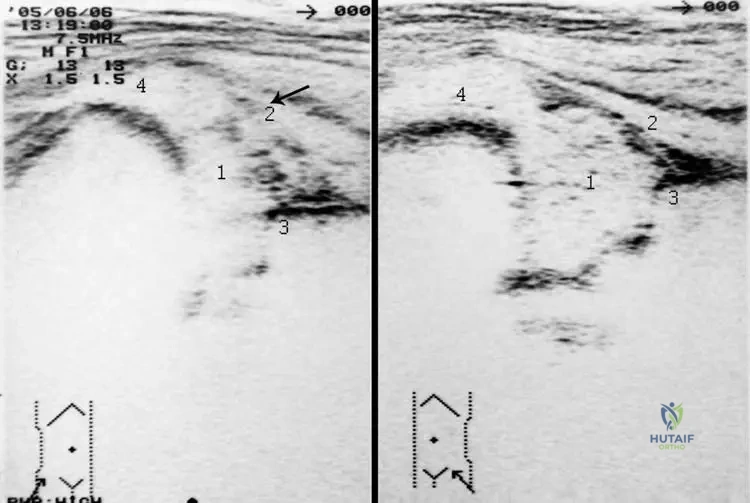
A 2-week-old neonate presents with pseudoparalysis of the right lower extremity and crying upon diaper changes. Ultrasound confirms a significant hip effusion.
What is the most appropriate next step in management?
What is the most appropriate next step in management?
Explanation
Neonatal septic arthritis ('coxitis') is a surgical emergency that can rapidly destroy the cartilaginous femoral head. Immediate joint aspiration and urgent open arthrotomy with irrigation is required to prevent permanent joint destruction.
Question 4
A 6-month-old infant with achondroplasia is noted to have brisk deep tendon reflexes and sleep apnea. What is the most common cause of mortality in this patient population during infancy?
Explanation
The most common cause of sudden death in infants with achondroplasia is cervicomedullary compression due to foramen magnum stenosis. Central sleep apnea and brisk reflexes are critical warning signs warranting urgent neurosurgical evaluation.
Question 5
Which of the following is the primary mechanism of action for the class of medications most commonly used to reduce fracture risk in pediatric patients with Osteogenesis Imperfecta?
Explanation
Bisphosphonates are the standard pharmacological treatment for Osteogenesis Imperfecta. They function by inhibiting osteoclast-mediated bone resorption, which increases bone density and decreases fracture incidence.
Question 6
A 16-year-old male presents with a 6-month history of chronic, dull back pain that is not completely relieved by NSAIDs. Radiographs reveal an expansile, lytic lesion in the posterior elements of L3.
What is the most likely diagnosis?
What is the most likely diagnosis?
Explanation
Osteoblastomas frequently involve the posterior elements of the spine and are classically larger than 2 cm. Unlike osteoid osteomas, the pain is typically less responsive to NSAIDs and less likely to be strictly nocturnal.
Question 7
A biopsy is taken from a 3 cm expansile lesion in the posterior elements of the cervical spine. Histological analysis reveals loose fibrovascular connective tissue intermixed with irregular osteoid and plump osteoblasts.
Which of the following is a primary characteristic distinguishing this condition from osteoid osteoma?
Which of the following is a primary characteristic distinguishing this condition from osteoid osteoma?
Explanation
Osteoblastoma and osteoid osteoma share identical histology, featuring irregular osteoid lined by plump osteoblasts in a vascular stroma. They are distinguished primarily by size (osteoblastoma > 2 cm) and clinical symptoms.
Question 8
A 5-month-old infant presents with frontal bossing, rhizomelic shortening of the limbs, and midface hypoplasia. Which of the following describes the genetic etiology of this condition?
Explanation
Achondroplasia is the most common skeletal dysplasia, caused by a gain-of-function mutation in the FGFR3 gene. This mutation constitutively inhibits chondrocyte proliferation in the proliferative zone of the physis.
Question 9
A 12-year-old boy presents with a painful mass on his distal femur. Radiographs show a permeative, diaphyseal lesion with an 'onion-skin' periosteal reaction. Which chromosomal translocation is most classically associated with this tumor?
Explanation
Ewing sarcoma typically presents as a permeative diaphyseal lesion with onion-skinning. It is strongly associated with the t(11;22) translocation, resulting in the EWS-FLI1 fusion protein.
Question 10
A 3-week-old neonate presents with fever, irritability, and a pseudoparalysis of the right lower extremity. Ultrasound reveals a hip joint effusion.
What is the most appropriate next step in management?
What is the most appropriate next step in management?
Explanation
Neonatal septic arthritis of the hip is a surgical emergency. Delay in decompression can lead to rapid destruction of the unossified femoral head (Tom Smith arthritis).
Question 11
A 7-year-old girl is evaluated for recurrent long bone fractures after minimal trauma. She has blue sclerae and mild hearing loss. This condition is primarily caused by a defect in which of the following?
Explanation
Osteogenesis imperfecta is characterized by brittle bones, blue sclerae, and hearing loss. It is caused by mutations in the COL1A1 or COL1A2 genes, which encode Type I collagen.
Question 12
A 9-year-old boy sustains a minor fall and presents with arm pain. Radiographs reveal a centrally located, lytic metaphyseal lesion in the proximal humerus with a 'fallen leaf' sign. Aspiration yields clear, yellow fluid. What is the most likely diagnosis?
Explanation
Unicameral (simple) bone cysts are fluid-filled, centrally located metaphyseal lesions commonly found in the proximal humerus or femur. A 'fallen leaf' sign represents a fractured piece of cortex settling at the bottom of the cystic cavity.
Question 13
A newborn presents with severe bilateral clubfeet, 'hitchhiker' thumbs, and cystic swelling of the external ears (cauliflower ears). Which of the following genes is mutated in this condition?
Explanation
Diastrophic dysplasia is an autosomal recessive disorder caused by a mutation in the SLC26A2 sulfate transporter gene. Classic features include hitchhiker thumbs, cauliflower ears, and severe clubfeet.
Question 14
Which of the following clinical features most accurately differentiates an osteoblastoma from an osteoid osteoma?
Explanation
Unlike osteoid osteomas, osteoblastomas produce dull, aching pain that is less strictly nocturnal and less predictably relieved by NSAIDs. Osteoblastomas are also defined by a size greater than 2 cm.
Question 15
A 14-year-old male presents with knee pain. Radiographs show a well-circumscribed, eccentrically placed, lytic lesion in the distal femoral epiphysis with a thin sclerotic rim. Histological examination shows mononuclear cells and areas of 'chicken-wire' calcification. What is the diagnosis?
Explanation
Chondroblastoma is a rare benign cartilage tumor that characteristically arises in the epiphysis of long bones in skeletally immature patients. 'Chicken-wire' calcification is the pathognomonic histologic feature.
Question 16
An 8-year-old boy presents with a waddling gait and bilateral knee and hip pain. Radiographs reveal delayed ossification and irregularity of multiple epiphyses. Spine radiographs are completely normal. Mutation in which gene is most likely responsible?
Explanation
Multiple Epiphyseal Dysplasia (MED) involves irregular, delayed epiphyseal ossification but spares the spine, differentiating it from spondyloepiphyseal dysplasia. The most common mutation is in the COMP gene (Cartilage Oligomeric Matrix Protein).
Question 17
A 15-year-old girl presents with a rapidly growing mass on her distal femur. Biopsy reveals malignant spindle cells producing delicate, lace-like osteoid matrix. What is the most common subtype of this tumor?
Explanation
Osteosarcoma is characterized by malignant cells producing an osteoid matrix. The conventional intramedullary subtype is the most common form, typically arising in the metaphyses of long bones in adolescents.
Question 18
A 6-year-old boy presents with a solitary, 'punched-out' lytic skull lesion. Biopsy reveals cells with grooved nuclei (coffee-bean appearance) and eosinophils. Immunohistochemistry will likely be positive for which of the following markers?
Explanation
Langerhans Cell Histiocytosis (LCH), previously known as Eosinophilic Granuloma in its localized form, features Langerhans cells with coffee-bean nuclei and Birbeck granules on EM. They characteristically stain positive for CD1a and S-100.
Question 19
A child born with normal length and facial features develops severe short stature and a waddling gait by age 3. Radiographs demonstrate small, irregular epiphyses and platyspondyly with anterior tongue-like projections of the vertebral bodies. Which of the following is the most likely diagnosis?
Explanation
Pseudoachondroplasia patients are normal at birth but develop significant dwarfism in early childhood. Unlike classic achondroplasia, they have normal facies but significant epiphyseal and spinal involvement (COMP mutation).
Question 20
A 12-year-old boy with Multiple Hereditary Exostoses (MHE) is monitored for malignant transformation. Which anatomical location of an osteochondroma carries the highest risk of malignant transformation into a secondary chondrosarcoma?
Explanation
While osteochondromas are most common around the knee, lesions located in the pelvis, shoulder girdle, and proximal femur carry the highest risk for malignant transformation into secondary chondrosarcomas.
Question 21
An incidental finding on a knee radiograph of a 14-year-old male shows an eccentrically located, multilobulated lucent lesion with a sclerotic rim in the distal femoral metaphysis. Histology from a similar lesion typically shows spindle cells in a storiform pattern with foamy histiocytes. What is the most appropriate management?
Explanation
Non-ossifying fibromas (NOF) are common, benign, self-limiting lesions in children and adolescents. They are asymptomatic, discovered incidentally, and heal spontaneously by sclerosis, requiring only observation.
Question 22
A newborn presents with delayed closure of the cranial sutures, wormian bones, and absent clavicles. What gene mutation is associated with this syndrome?
Explanation
Cleidocranial dysplasia is an autosomal dominant condition characterized by absent or hypoplastic clavicles and delayed cranial suture closure. It is caused by a mutation in the RUNX2 (CBFA1) transcription factor, essential for osteoblast differentiation.
Question 23
An 11-year-old boy presents with fever, focal distal femur pain, and elevated inflammatory markers. Radiographs show a permeative diaphyseal lesion. Biopsy shows sheets of small round blue cells. Immunohistochemistry is strongly positive for CD99. Which of the following is the most important component of the initial treatment algorithm for this condition?
Explanation
The clinical presentation, small round blue cells, and CD99 positivity indicate Ewing sarcoma. The standard of care involves neoadjuvant systemic chemotherapy to address micrometastatic disease, followed by local control (surgery or radiation).
Question 24
A 4-year-old child presents with a severe limb length discrepancy. Radiographs show complete destruction and absence of the capital femoral epiphysis and femoral neck on the right side.
This is the classic sequela of which untreated infantile condition?
This is the classic sequela of which untreated infantile condition?
Explanation
Tom Smith arthritis refers to the complete destruction of the infant hip joint due to delayed or untreated neonatal septic arthritis. The cartilaginous anlage is rapidly destroyed by proteolytic enzymes.
Question 25
A 19-year-old undergoes curettage of a 3.5 cm expansile lesion in the posterior elements of T12. Grossly, the tissue is a hemorrhagic, gritty, purplish-red friable mass.
What is the recommended standard surgical treatment for this benign but locally aggressive lesion?
What is the recommended standard surgical treatment for this benign but locally aggressive lesion?
Explanation
Osteoblastomas are locally aggressive benign tumors. The standard treatment is extended intralesional curettage, high-speed burring of the cavity, and bone grafting, which provides a low recurrence rate.
Question 26
A 16-year-old male presents with persistent mid-back pain not completely relieved by NSAIDs and a new-onset painful structural scoliosis. Radiographs of the spine are evaluated.
What is the most appropriate definitive management for the most likely diagnosis?
What is the most appropriate definitive management for the most likely diagnosis?
Explanation
Osteoblastoma typically presents in the posterior elements of the spine and can cause painful scoliosis. Unlike osteoid osteoma, it is >2cm, less responsive to NSAIDs, and usually treated with intralesional curettage or marginal excision.
Question 27
A 19-year-old female undergoes biopsy of an expansile lytic lesion in the posterior elements of L3.
The histology demonstrates irregular osteoid trabeculae in a vascular connective tissue stroma with prominent osteoblasts. What is the most likely diagnosis?
The histology demonstrates irregular osteoid trabeculae in a vascular connective tissue stroma with prominent osteoblasts. What is the most likely diagnosis?
Explanation
The histology shows benign, irregular osteoid intermixed with loose fibrovascular connective tissue and prominent osteoblastic rimming, characteristic of osteoblastoma. It differs from osteosarcoma by lacking severe cytologic atypia and atypical mitoses.
Question 28
A child with short stature, frontal bossing, and rhizomelic limb shortening is evaluated. Radiographs show narrowing of the interpedicular distances in the lumbar spine. Which of the following describes the underlying molecular defect?
Explanation
Achondroplasia is caused by an autosomal dominant gain-of-function mutation in the FGFR3 gene. This leads to profound inhibition of chondrocyte proliferation in the proliferative zone of the physis, resulting in rhizomelic dwarfism and spinal stenosis.
Question 29
A newborn presents with short-limbed dwarfism, bilateral rigid clubfeet, "hitchhiker" thumbs, and cystic swelling of the pinnae. What is the primary pathophysiologic defect in this condition?
Explanation
Diastrophic dysplasia is caused by an autosomal recessive mutation in the SLC26A2 gene, resulting in a defect in the diastrophic dysplasia sulfate transporter (DTDST). This leads to profoundly impaired sulfation of cartilage proteoglycans.
Question 30
A 14-year-old boy presents with right knee pain. Radiographs reveal a well-circumscribed, eccentrically located lytic lesion with a thin sclerotic rim within the proximal tibial epiphysis. Histology shows mononuclear cells with grooved nuclei and "chicken-wire" calcifications. Which immunohistochemical marker is characteristically positive in this tumor?
Explanation
Chondroblastomas are benign, epiphyseal cartilage-producing tumors that classically exhibit "chicken-wire" calcification and coffee-bean shaped nuclei. They are characteristically positive for S-100 and DOG1 on immunohistochemical staining.
Question 31
A 10-year-old girl presents with a permeative lytic lesion in the femoral diaphysis with an "onion-skin" periosteal reaction. A biopsy confirms Ewing sarcoma. Which of the following cytogenetic abnormalities is most commonly associated with this tumor?
Explanation
Ewing sarcoma is classically associated with the t(11;22)(q24;q12) translocation. This chromosomal abnormality fuses the EWS gene on chromosome 22 with the FLI1 gene on chromosome 11, creating an oncogenic transcription factor.
Question 32
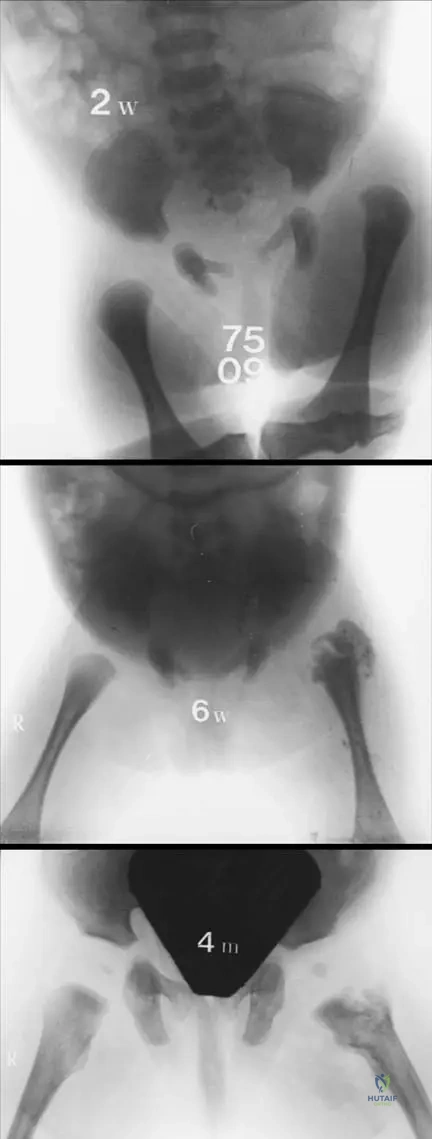
A 3-year-old child presents with a painless waddling gait.
AP pelvis radiograph demonstrates a decreased femoral neck-shaft angle, a vertically oriented physis, and a distinct triangular bone fragment in the inferior femoral neck. What radiographic measurement is the primary determinant for surgical intervention in this condition?
AP pelvis radiograph demonstrates a decreased femoral neck-shaft angle, a vertically oriented physis, and a distinct triangular bone fragment in the inferior femoral neck. What radiographic measurement is the primary determinant for surgical intervention in this condition?
Explanation
In infantile coxa vara, a Hilgenreiner's epiphyseal angle (HEA) greater than 60 degrees is a strong indication for surgical correction via a valgus-producing osteotomy. Angles less than 45 degrees typically resolve spontaneously.
Question 33
A 15-year-old boy has a biopsy-proven high-grade intramedullary osteosarcoma of the distal femur without distant metastasis. What is the standard treatment protocol for this patient?
Explanation
The standard of care for high-grade conventional osteosarcoma includes neoadjuvant chemotherapy, followed by wide surgical resection (favoring limb salvage if feasible), and concluding with adjuvant chemotherapy. This multidisciplinary approach maximizes long-term survival.
Question 34
A 6-year-old child with normal intelligence, corneal clouding, and severe platyspondyly presents with progressive cervical myelopathy. Radiographs reveal severe odontoid hypoplasia and atlantoaxial instability. What is the accumulated metabolite in this syndrome?
Explanation
Morquio syndrome (MPS Type IV) is an autosomal recessive disorder caused by a defect in galactose-6-sulfatase, leading to keratan sulfate accumulation. Patients typically have normal intelligence but severe skeletal dysplasia, notably odontoid hypoplasia causing profound atlantoaxial instability.
Question 35
A 7-year-old girl is evaluated for delayed dental eruption and abnormal shoulder mobility, allowing her to touch her shoulders together anteriorly. Radiographs show absent clavicles and delayed closure of cranial sutures. What is the mutated gene responsible for this condition?
Explanation
Cleidocranial dysplasia is an autosomal dominant condition caused by mutations in the RUNX2 (formerly CBFA1) gene, which is essential for osteoblast differentiation. It is characterized by absent or hypoplastic clavicles, delayed suture closure, and multiple dental anomalies.
Question 36
A 4-year-old child with recurrent fractures, blue sclerae, and dentinogenesis imperfecta is treated with intravenous pamidronate. What is the primary mechanism of action of this medication in treating this condition?
Explanation
Bisphosphonates like pamidronate are used in Osteogenesis Imperfecta to increase bone mineral density by inhibiting osteoclast-mediated bone resorption. They are internalized by osteoclasts, leading to disruption of the cytoskeleton and apoptosis.
Question 37
A 16-year-old boy presents with a painful rigid scoliosis that is poorly relieved by NSAIDs. Radiographs and CT show a 3.5 cm expansile, radiolucent lesion in the posterior elements of L3. Histology reveals woven bone trabeculae rimmed by prominent osteoblasts without nuclear atypia. What is the most appropriate definitive management?
Explanation
Osteoblastoma is a benign bone-forming tumor characteristically larger than 2 cm, frequently presenting in the posterior elements of the spine. Unlike osteoid osteoma, it is less responsive to NSAIDs and is best managed with meticulous intralesional curettage and bone grafting.
Question 38
A biopsy from a symptomatic lytic bone lesion in the distal femur of a 14-year-old reveals the provided histology, showing loose fibrovascular connective tissue intermixed with irregular osteoid. Which of the following features most reliably differentiates this lesion clinically from an osteoid osteoma?
Explanation
Both osteoblastoma and osteoid osteoma share identical, benign histologic features of woven bone and vascular stroma. They are primarily distinguished by size, with osteoblastomas arbitrarily defined as being greater than 2 centimeters in diameter.
Question 39
A 3-week-old neonate presents with pseudoparalysis of the right leg and crying with diaper changes. There is no fever, but CRP is significantly elevated. Ultrasound reveals a hip effusion. If this neonatal septic arthritis (coxitis) is diagnosed late and untreated, what is the most severe classical long-term orthopedic complication?
Explanation
Neonatal septic arthritis of the hip often lacks classic systemic signs like high fever. Delayed diagnosis and treatment lead to rapid cartilaginous destruction and complete resorption of the proximal femur, a devastating sequela known as Tom Smith arthritis.
Question 40
A 6-year-old boy is evaluated for short stature, a waddling gait, and a barrel chest. Radiographs demonstrate delayed ossification of the capital femoral epiphyses, coxa vara, and platyspondyly. Ophthalmic examination reveals high myopia. A mutation in which of the following genes is most likely responsible?
Explanation
Spondyloepiphyseal dysplasia congenita (SEDC) affects the spine and epiphyses, and is associated with coxa vara, high myopia, and retinal detachment. It is caused by an autosomal dominant mutation in the COL2A1 gene affecting Type II collagen.
Question 41
The image demonstrates the gross curettage specimen of a primary bone tumor excised from the posterior elements of a 17-year-old's cervical spine. The tumor typically presents with dull pain that is not completely relieved by NSAIDs. Which of the following best describes the classical radiographic finding of this condition?
Explanation
Osteoblastomas typically appear radiographically as expansile, predominantly lytic lesions larger than 2 cm with a thin rim of reactive bone. They are most commonly located in the posterior elements of the spine.
Question 42
A 4-year-old girl with frontal bossing, midface hypoplasia, and rhizomelic shortening of the upper and lower extremities is being evaluated in the clinic. Her parents are of normal stature. Which of the following describes the pathophysiologic mechanism of the genetic mutation in this patient?
Explanation
Achondroplasia is caused by a gain-of-function mutation in the FGFR3 gene. This overactivity continuously inhibits normal chondrocyte proliferation in the proliferative zone of the physis, leading to restricted endochondral ossification.
Question 43
A 17-year-old male presents with chronic dull, aching back pain that is not completely relieved by NSAIDs. Imaging shows a 2.5 cm expansile lytic lesion in the posterior elements of L3.
What is the most likely diagnosis?
What is the most likely diagnosis?
Explanation
Osteoblastoma typically presents as an expansile lesion greater than 2 cm in the posterior elements of the spine. Unlike osteoid osteoma, the pain is less classically nocturnal and less completely responsive to NSAIDs.
Question 44
A biopsy is taken from a painful expansile lesion in the C2 lamina. Histology demonstrates the following features.
Which histologic finding is most characteristic of this condition?
Which histologic finding is most characteristic of this condition?
Explanation
Osteoblastomas typically feature loose fibrovascular connective tissue intermixed with irregular osteoid. Mitotic figures may be present, differentiating it somewhat from entirely quiescent lesions, but lacks malignant anaplasia.
Question 45
A 2-week-old neonate presents with asymmetric skin folds, pseudoparalysis of the right leg, and pain with passive hip motion.
Ultrasound confirms a large joint effusion consistent with septic arthritis. Which pathogen is most uniquely common in this specific age group compared to older children?
Ultrasound confirms a large joint effusion consistent with septic arthritis. Which pathogen is most uniquely common in this specific age group compared to older children?
Explanation
Group B Streptococcus (S. agalactiae) is a major cause of neonatal septic arthritis (coxitis), acquired during vaginal delivery. While S. aureus is also common, Group B Strep is uniquely prevalent in the neonatal period.
Question 46
A 4-year-old child with rhizomelic short stature, frontal bossing, and trident hands is diagnosed with achondroplasia. Which of the following best describes the underlying genetic defect?
Explanation
Achondroplasia is caused by an autosomal dominant gain-of-function mutation in the FGFR3 gene. This overactivity continuously inhibits chondrocyte proliferation in the proliferative zone of the physis.
Question 47
Which of the following radiographic findings is most characteristic of an aggressive osteoblastoma rather than conventional osteosarcoma?
Explanation
Aggressive osteoblastoma often presents as a large, expansile lesion with a thin peripheral shell of reactive bone. Conventional osteosarcoma classically shows more destructive features like Codman's triangle or a sunburst reaction.
Question 48
An infant is placed in a Pavlik harness for developmental dysplasia of the hip. At the 2-week follow-up, the parents report the infant is no longer actively kicking the right leg. Physical examination reveals absent active knee extension on the affected side. What is the most likely cause?
Explanation
Femoral nerve palsy in a Pavlik harness is typically caused by excessive hip flexion resulting from overtightened anterior straps. Management involves loosening the anterior straps or discontinuing the harness temporarily.
Question 49
A 5-year-old boy presents with disproportionate short stature, normal facies, and joint laxity. Radiographs demonstrate delayed epiphyseal ossification and platyspondyly with anterior tongue-like projections. What is the most likely diagnosis?
Explanation
Pseudoachondroplasia presents with short-limb dwarfism, severe joint laxity, and normal facial features (unlike achondroplasia). It is caused by a mutation in the COMP gene.
Question 50
A 12-year-old obese boy presents with a left slipped capital femoral epiphysis (SCFE). Which of the following is an absolute indication for prophylactic in situ pinning of the contralateral, asymptomatic hip?
Explanation
Prophylactic pinning of the contralateral hip in SCFE is strongly recommended in patients with endocrine disorders (e.g., hypothyroidism, renal osteodystrophy) due to the very high risk of bilateral involvement.
Question 51
During the Ponseti method for treating idiopathic clubfoot, the very first step in casting manipulation addresses which component of the deformity?
Explanation
The first step in the Ponseti method is to correct the cavus deformity. This is achieved by elevating the first ray and supinating the forefoot to align it with the hindfoot.
Question 52
A 10-year-old girl presents with a rapidly enlarging mass over her proximal humerus. Radiographs show an eccentric, expansile, purely lytic lesion. MRI demonstrates multiple fluid-fluid levels. What is the most appropriate definitive surgical management after biopsy confirms an active aneurysmal bone cyst (ABC)?
Explanation
The standard surgical treatment for an active aneurysmal bone cyst is extended intralesional curettage utilizing an adjuvant (e.g., high-speed burr, phenol, cryotherapy) followed by bone grafting or cementation.
Question 53
In Legg-Calvé-Perthes disease, the Herring Lateral Pillar classification is most reliably applied at what stage of the disease to predict the ultimate deformity?
Explanation
The Herring Lateral Pillar classification assesses the structural height of the lateral pillar of the femoral head. It is most accurately determined during the early to mid fragmentation stage before reossification begins.
Question 54
A 6-year-old child is evaluated for a severe limp and limb length discrepancy. History is significant for a prolonged neonatal intensive care unit stay for sepsis. Radiographs demonstrate complete absence of the femoral head and neck, as seen in the provided late-stage example. What is this specific sequela of neonatal septic arthritis called?

Explanation
Tom Smith arthritis refers to the complete resorption or destruction of the femoral head and neck following severe infantile septic arthritis. This results in a chronically dislocated, unstable hip with a profound limb length discrepancy.
Question 55
A 16-year-old male presents with dull, aching pain in his cervical spine. Radiographs and MRI demonstrate an expansile 3.5 cm lesion in the posterior elements of C4.
During curettage, the lesion appears hypervascular and granular. Which of the following best describes the distinguishing features of this lesion compared to an osteoid osteoma?
During curettage, the lesion appears hypervascular and granular. Which of the following best describes the distinguishing features of this lesion compared to an osteoid osteoma?
Explanation
Osteoblastomas are typically larger than 2 cm, show progressive pain not reliably relieved by NSAIDs/salicylates, and predominantly affect the posterior elements of the spine. Osteoid osteomas are smaller (<2 cm) and respond well to NSAIDs.
Question 56
A 3-week-old infant presents with fever, irritability, and pseudoparalysis of the right leg. Ultrasound confirms a large hip effusion.
If surgical drainage is delayed, what is the most severe and irreversible complication according to the Choi classification?
If surgical drainage is delayed, what is the most severe and irreversible complication according to the Choi classification?
Explanation
Delayed treatment of neonatal septic arthritis (coxitis) can rapidly lead to avascular necrosis and complete destruction of the cartilaginous femoral head and neck. This corresponds to the most severe types in the Choi classification, resulting in permanent instability.
Question 57
A 4-year-old child with disproportionate short stature, frontal bossing, and rhizomelic shortening of the limbs is diagnosed with achondroplasia. Which of the following accurately describes the molecular pathogenesis of this condition?
Explanation
Achondroplasia is caused by an activating (gain-of-function) mutation in the FGFR3 gene. This constitutively active receptor inhibits normal chondrocyte proliferation at the growth plate, leading to rhizomelic dwarfism.
Question 58
A 7-year-old boy with blue sclerae, dentinogenesis imperfecta, and multiple prior fractures is started on intravenous pamidronate. What is the primary mechanism of action of this medication in the treatment of Osteogenesis Imperfecta?
Explanation
Pamidronate is a nitrogen-containing bisphosphonate that inhibits farnesyl pyrophosphate synthase in the mevalonate pathway. This promotes osteoclast apoptosis and decreases bone resorption, increasing overall bone density in Osteogenesis Imperfecta.
Question 59
A biopsy from a diaphyseal femur lesion in an 11-year-old boy reveals sheets of uniform, small, round, blue cells. Molecular testing is positive for a t(11;22)(q24;q12) translocation. Which of the following fusion proteins is most likely driving this malignancy?
Explanation
The t(11;22)(q24;q12) translocation is the hallmark of Ewing Sarcoma. It results in the EWSR1-FLI1 fusion protein, which acts as an aberrant transcription factor promoting tumorigenesis.
Question 60
A 12-year-old boy with Multiple Hereditary Exostoses (MHE) is evaluated for a rapidly growing, painful lesion on his proximal humerus. Mutations in EXT1 and EXT2 genes are implicated in MHE. These genes normally encode enzymes responsible for the synthesis of which molecule?
Explanation
EXT1 and EXT2 genes encode glycosyltransferases essential for the polymerization of heparan sulfate. Defects in this pathway disrupt normal physeal signaling, leading to osteochondroma formation.
Question 61
A patient presents with absent clavicles, delayed closure of cranial sutures, and supernumerary teeth. Which transcription factor is primarily mutated in this syndrome?
Explanation
Cleidocranial dysplasia is caused by an autosomal dominant mutation in the RUNX2 (CBFA1) gene. This transcription factor is critical for osteoblast differentiation and both intramembranous and endochondral ossification.
Question 62
Which of the following clinical and genetic findings uniquely characterize Diastrophic Dysplasia compared to other short-limb dysplasias?
Explanation
Diastrophic dysplasia is an autosomal recessive disorder caused by a defect in the SLC26A2 sulfate transporter. It is classically associated with cauliflower ears, hitchhiker thumbs, severe clubfeet, and cleft palate.
Question 63
A 9-year-old girl sustains a pathologic fracture through a proximal humerus lesion. Radiographs demonstrate a centrally located, lytic metaphyseal lesion with a "fallen leaf" sign. Which of the following best describes the natural history of this lesion if left untreated?
Explanation
Unicameral bone cysts (UBCs) are benign, fluid-filled lesions typically found in the metaphysis of growing children. They migrate diaphyseally away from the physis over time and usually resolve spontaneously upon skeletal maturity.
Question 64
Aneurysmal bone cysts (ABCs) can occur as primary lesions or secondary to other bone tumors. Primary ABCs have been shown to be true neoplasms driven by a specific genetic rearrangement. Which gene is typically upregulated due to translocation in primary ABCs?
Explanation
Primary aneurysmal bone cysts are neoplastic and characterized by translocations involving the USP6 gene on chromosome 17 (e.g., t(16;17)). This leads to increased matrix metalloproteinase activity and cystic bone destruction.
Question 65
A 10-year-old boy undergoes knee radiographs following minor trauma, revealing an incidental, eccentric, cortically based, multiloculated lucent lesion in the distal femoral metaphysis. He is completely asymptomatic. What is the most appropriate management?
Explanation
The radiographic description is classic for a Non-Ossifying Fibroma (NOF). Because the patient is asymptomatic and the lesion is an incidental finding, the standard of care is observation. NOFs typically ossify and resolve by skeletal maturity.
Question 66
A 5-year-old child presents with waddling gait and disproportionate short stature. Unlike patients with achondroplasia, this child has normal craniofacial features. Radiographs show delayed epiphyseal ossification and irregular, fragmented metaphyses. A mutation in which gene is most likely responsible?
Explanation
Pseudoachondroplasia presents with severe disproportionate short stature but is distinguished from achondroplasia by completely normal craniofacial features. It is caused by mutations in the Cartilage Oligomeric Matrix Protein (COMP) gene.
Question 67
A 6-year-old boy with Morquio Syndrome (Mucopolysaccharidosis Type IV) is scheduled for elective bilateral osteotomies for severe genu valgum. Preoperatively, which of the following evaluations is absolutely critical to prevent catastrophic neurologic injury during intubation?
Explanation
Patients with Morquio Syndrome frequently have odontoid hypoplasia leading to severe atlantoaxial instability. Flexion-extension cervical spine radiographs are mandatory before any procedure requiring anesthesia or neck manipulation to prevent spinal cord injury.
Question 68
A 14-year-old girl presents with precocious puberty, café-au-lait macules with irregular 'coast of Maine' borders, and multiple lytic bone lesions with a ground-glass appearance. Histologic examination of the bone lesions would most likely reveal:
Explanation
The clinical presentation is classic for McCune-Albright syndrome, which features polyostotic fibrous dysplasia. Histologically, fibrous dysplasia exhibits irregular trabeculae of woven bone (Chinese character pattern) in a fibrous stroma, characteristically lacking osteoblastic rimming.
Question 69
A 15-year-old boy complains of chronic knee pain. Radiographs demonstrate a well-circumscribed, eccentrically located, lytic lesion exclusively within the proximal tibial epiphysis. Biopsy reveals mononuclear cells with longitudinal nuclear grooves and areas of "chicken-wire" calcification. What is the diagnosis?
Explanation
Chondroblastoma is a rare, benign cartilaginous tumor that characteristically arises in the epiphysis or apophysis of growing children. The histologic hallmarks are chondroblasts with grooved nuclei (coffee-bean shape) and pericellular 'chicken-wire' calcifications.
Question 70
Spondyloepiphyseal Dysplasia Congenita (SEDC) is a disproportionate short-trunk dwarfism. Patients frequently present with severe coxa vara. Which genetic mutation is primarily responsible for SEDC?
Explanation
Spondyloepiphyseal Dysplasia Congenita (SEDC) is caused by autosomal dominant mutations in the COL2A1 gene, which encodes type II collagen. This leads to defective endochondral ossification, prominent spinal involvement (platyspondyly), and coxa vara.
Question 71
A 4-year-old boy presents with a painful, solitary lytic lesion of the skull. A biopsy demonstrates sheets of cells with indented nuclei intermixed with eosinophils. Immunohistochemistry is positive for CD1a and S-100. Electron microscopy of these cells would most likely show:
Explanation
The clinical and histologic findings describe Langerhans Cell Histiocytosis (Eosinophilic Granuloma). The diagnostic ultrastructural feature on electron microscopy is the presence of Birbeck granules, which resemble tennis rackets.
Question 72
A 13-year-old girl is diagnosed with high-grade intramedullary osteosarcoma of the distal femur. Which of the following is considered the most significant adverse prognostic factor at the time of initial diagnosis?
Explanation
While an elevated alkaline phosphatase is a poor prognostic factor, the presence of macroscopic skip metastases within the same bone indicates advanced disease and is associated with a significantly worse prognosis and higher risk of systemic spread.
Question 73
During curettage of a suspected benign spinal lesion in a 20-year-old female, the surgeon notes the gross appearance shown in the provided atlas image.
The tissue is red, granular, and heavily bleeding. Histologic analysis is ordered. Which feature is crucial to differentiate this lesion (osteoblastoma) from a well-differentiated osteosarcoma?
The tissue is red, granular, and heavily bleeding. Histologic analysis is ordered. Which feature is crucial to differentiate this lesion (osteoblastoma) from a well-differentiated osteosarcoma?
Explanation
Osteoblastomas are benign and distinctively well-circumscribed (pushing margins), despite their hypercellularity and occasional atypia. The hallmark differentiating them from osteosarcoma is the absence of permeative invasion trapping host lamellar bone trabeculae.
Question 74
A 2-year-old boy presents with anterolateral bowing of the left tibia. Radiographs reveal sclerosis and a narrowing of the medullary canal at the apex of the bow. Which of the following systemic conditions is most strongly associated with this finding?
Explanation
Anterolateral bowing of the tibia is the hallmark precursor to congenital pseudarthrosis of the tibia (CPT). It is highly associated with Neurofibromatosis Type 1 (NF-1), occurring in up to 50% of CPT patients.
Question 75
A 16-year-old male presents with localized cervical spine pain. Radiographs reveal a 3.5 cm expansile, radiolucent lesion in the posterior elements of C4.
Which of the following characteristics most reliably differentiates this lesion from an osteoid osteoma?
Which of the following characteristics most reliably differentiates this lesion from an osteoid osteoma?
Explanation
Osteoblastoma and osteoid osteoma are histologically identical, primarily consisting of woven bone trabeculae and fibrovascular stroma. The main clinical and diagnostic differentiating factor is size, with osteoblastomas defined as being larger than 2 cm in diameter.
Question 76
A 2-year-old boy presents with disproportionate short stature, rhizomelic shortening, and frontal bossing. Radiographs show narrowing of the interpedicular distances in the lumbar spine. Which of the following gene mutations is the primary cause of this condition?
Explanation
Achondroplasia is the most common form of short-limbed dwarfism, caused by an autosomal dominant gain-of-function mutation in the FGFR3 gene. This mutation inhibits chondrocyte proliferation in the proliferative zone of the physis, leading to defective endochondral ossification.
Question 77
A 19-year-old female undergoes curettage for an expansile, painful lesion in the posterior elements of T12. The gross pathological specimen is shown.
Histological analysis shows rich vascularity and prominent osteoblasts surrounding irregular osteoid. What is the most common potential complication if this lesion is treated with standard intralesional curettage alone?
Histological analysis shows rich vascularity and prominent osteoblasts surrounding irregular osteoid. What is the most common potential complication if this lesion is treated with standard intralesional curettage alone?
Explanation
Osteoblastoma is a benign but locally aggressive tumor. When treated with intralesional curettage alone, local recurrence rates can be high (up to 20%), often necessitating extended curettage with a high-speed burr or en bloc resection.
Question 78
A 4-week-old infant was diagnosed with neonatal septic arthritis of the hip. Treatment was delayed for several days prior to surgical drainage. A follow-up radiograph one year later shows complete absence of the proximal femoral epiphysis and neck.
This severe structural loss is primarily the result of which of the following pathophysiologic mechanisms?
This severe structural loss is primarily the result of which of the following pathophysiologic mechanisms?
Explanation
In neonatal septic arthritis, bacterial toxins and white blood cell-derived proteolytic enzymes rapidly destroy the unossified hyaline cartilage of the femoral head. Combined with capsular distension compromising intra-articular vasculature, this leads to complete resorption of the proximal femoral epiphysis.
Question 79
A 6-year-old child presents with a femoral shaft fracture after a minor mechanical fall. Physical examination reveals blue sclerae and mild hearing loss. Radiographs show generalized osteopenia and thin cortices. Which of the following represents the underlying molecular defect in this patient's condition?
Explanation
Osteogenesis imperfecta is typically caused by autosomal dominant mutations in the COL1A1 or COL1A2 genes, leading to defective type I collagen synthesis or structure. This results in brittle bones, multiple fractures, blue sclerae, and early-onset hearing loss.
Question 80
A 22-year-old man presents with chronic, non-mechanical lower back pain. Imaging shows an expansile 3 cm lytic lesion of the L4 pedicle. A biopsy is performed, and the photomicrograph is shown below.
Which of the following features is most characteristic of this lesion's microscopic appearance?
Which of the following features is most characteristic of this lesion's microscopic appearance?
Explanation
The defining histology of an osteoblastoma involves loose fibrovascular connective tissue intermixed with irregular, interconnected woven bone trabeculae rimmed by prominent, benign osteoblasts. It lacks the severe cellular atypia and destructive permeation seen in osteosarcoma.
Question 81
A 12-year-old boy presents with multiple painless, bony prominences around his knees, ankles, and shoulders. Radiographs reveal multiple osteochondromas pointing away from the joint lines. He is diagnosed with Multiple Hereditary Exostoses (MHE). Which of the following genes is most likely mutated, and what is the estimated risk of malignant transformation in his lifetime?
Explanation
Multiple Hereditary Exostoses is inherited in an autosomal dominant pattern and is most often caused by mutations in the EXT1 or EXT2 tumor suppressor genes. The lifetime risk of an osteochondroma undergoing malignant transformation to a secondary chondrosarcoma is approximately 1% to 5%.
Question 82
A 16-year-old boy presents with painful scoliosis. Radiographs demonstrate an expansile lesion in the posterior elements of the lumbar spine.
What is the characteristic scoliotic curve pattern associated with this type of lesion?
What is the characteristic scoliotic curve pattern associated with this type of lesion?
Explanation
Painful lesions like osteoblastoma and osteoid osteoma in the posterior elements cause unilateral paravertebral muscle spasm. This spasm creates a concavity on the side of the lesion, causing the apex of the scoliotic curve to be directed away from the lesion.
Question 83
An 18-year-old male undergoes curettage of a 3.5 cm posterior spinal lesion. The gross specimen demonstrates hemorrhagic, gritty red tissue.
Based on the gross appearance and size of the lesion, what is the most likely diagnosis?
Based on the gross appearance and size of the lesion, what is the most likely diagnosis?
Explanation
Osteoblastoma is histologically identical to osteoid osteoma but is distinguished by a size greater than 2 cm. Grossly, it appears as a vascular, gritty, and reddish mass due to abundant osteoid and prominent vascularity.
Question 84
A 3-week-old infant is brought to the emergency department for pseudoparalysis of the right leg. Ultrasound confirms a large hip effusion.
Diagnostic aspiration yields frankly purulent fluid. In addition to Staphylococcus aureus, which pathogen is uniquely highly prevalent in this specific age group?
Diagnostic aspiration yields frankly purulent fluid. In addition to Staphylococcus aureus, which pathogen is uniquely highly prevalent in this specific age group?
Explanation
While Staphylococcus aureus is the most common cause of septic arthritis across all pediatric age groups, Group B Streptococcus (S. agalactiae) is the second most common pathogen uniquely seen in neonates. Kingella kingae is more frequently seen in older infants and toddlers (6 months to 4 years).
Question 85
In the surgical treatment of neonatal septic arthritis of the hip, an anterior approach (Smith-Petersen) is often preferred for open arthrotomy and drainage. Which internervous plane is utilized in this surgical approach?
Explanation
The anterior (Smith-Petersen) approach to the hip utilizes the internervous plane between the sartorius (femoral nerve) and the tensor fasciae latae (superior gluteal nerve). This approach provides direct access to the hip joint capsule while avoiding the critical medial circumflex femoral artery.
Question 86
A 4-year-old boy presents with rhizomelic short stature, frontal bossing, midface hypoplasia, and trident hands. Which genetic mutation is responsible for his condition?
Explanation
Achondroplasia is the most common form of short-limb dwarfism and is caused by an autosomal dominant gain-of-function mutation in the FGFR3 gene. This mutation abnormally inhibits chondrocyte proliferation in the proliferative zone of the physis.
Question 87
A 5-year-old child presents with a history of recurrent long bone fractures after minimal trauma, blue sclerae, and dentinogenesis imperfecta. What is the underlying biochemical defect in this disorder?
Explanation
Osteogenesis imperfecta is caused by a quantitative or qualitative defect in Type I collagen, which is the primary collagen type in bone, sclera, and dentin. It typically results from mutations in the COL1A1 or COL1A2 genes.
Question 88
A 14-year-old male presents with chronic knee pain. Radiographs reveal a 2 cm well-circumscribed, lytic lesion in the distal femoral epiphysis with a sclerotic margin. Biopsy shows polyhedral mononuclear cells and "chicken wire" calcifications. What is the diagnosis?
Explanation
Chondroblastoma is a rare benign bone tumor that classically occurs in the epiphysis or apophysis of growing children. Histologically, it is characterized by mononuclear chondroblasts, osteoclast-like giant cells, and distinctive "chicken wire" pericellular calcifications.
None
Previous ChapterMaster ABOS Orthopedic Board Review: Pediatric Infections, …
Next Chapter Master ABOS Orthopedic Pathology & Skeletal Dysplasia Revie…

Medically Verified Content by
Prof. Dr. Mohammed Hutaif Clinic
Consultant Orthopedic & Spine Surgeon