ABOS Board Review: Orthopedic Pathology, Bone Tumors, Skeletal Dysplasias, Arthritis | Part 12

Key Takeaway
This ABOS Orthopedic Board Review provides comprehensive multiple-choice questions covering musculoskeletal pathology. Topics include bone tumors, skeletal dysplasias, arthritis, osteomyelitis, stress fractures, and rare bone disorders. It emphasizes clinical presentation, radiographic findings, and pathological insights crucial for board exam preparation.
ABOS Board Review: Orthopedic Pathology, Bone Tumors, Skeletal Dysplasias, Arthritis | Part 12
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 68-year-old male presents with generalized fatigue, worsening back pain, and a recent humeral shaft fracture after a minor fall. Radiographs demonstrate multiple punched-out lytic lesions.
Which of the following factors is primarily responsible for the suppression of osteoblastic activity in this patient's disease process?

Explanation
Question 2
A 9-year-old boy presents with severe leg pain, easy fatigability, and a waddling gait. Radiographs reveal symmetrical, bilateral cortical thickening of the diaphyseal regions of the femur and tibia, sparing the epiphyses.
What is the genetic mutation associated with this condition?
Explanation
Question 3
A 45-year-old female is 8 weeks status post closed reduction and cast immobilization for a distal radius fracture. She complains of severe, burning pain that is disproportionate to the injury, along with skin color changes and stiffness.
Radiographs show patchy osteopenia. Which intervention has been shown to reduce the incidence of this condition when administered daily following a distal radius fracture?
Explanation
Question 4
Which of the following describes the earliest biochemical change occurring in the articular cartilage during the pathogenesis of osteoarthritis?
Explanation
Question 5
A 25-year-old female with known rheumatoid arthritis presents with worsening neck pain and myelopathic symptoms. Radiographs of the cervical spine reveal an anterior atlanto-dens interval (ADI) of 11 mm. Which of the following radiographic measurements is the most reliable predictor of neurologic recovery after surgical decompression and stabilization?
Explanation
Question 6
A 35-year-old male undergoes curettage and cementation of a giant cell tumor of the distal femur. Six months later, he develops a massive recurrence that is deemed unresectable. Medical therapy with denosumab is initiated. What is the mechanism of action of this medication?
Explanation
Question 7
A 14-year-old boy presents with a painful, swollen thigh. Radiographs demonstrate a permeative, diaphyseal lytic lesion with an 'onion-skin' periosteal reaction. A biopsy confirms Ewing sarcoma. Which of the following chromosomal translocations is most characteristic of this tumor?
Explanation
Question 8
A 55-year-old male presents with severe acute monoarticular pain, erythema, and swelling in his first metatarsophalangeal joint. Joint aspiration reveals negatively birefringent, needle-shaped crystals under polarized light microscopy. Which of the following is the composition of these crystals?
Explanation
Question 9
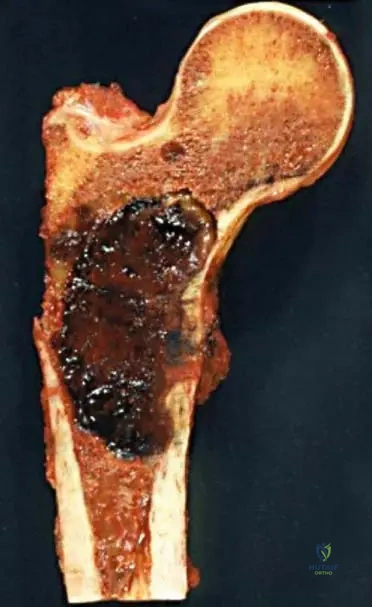
A 70-year-old male with long-standing Paget disease of bone complains of a sudden increase in pain and swelling in his right proximal femur over the last two months. Radiographs reveal a new, destructive lytic lesion with cortical breakthrough. What is the most likely diagnosis?
Explanation
Question 10
A 10-month-old infant is evaluated for short stature, frontal bossing, and a waddling gait. Radiographs reveal widening of the physes, cupping of the metaphyses, and bowing of the long bones. Laboratory studies show normal calcium, low phosphorus, and elevated alkaline phosphatase. Which of the following describes the underlying histologic defect?
Explanation
Question 11
A 30-year-old male with known ankylosing spondylitis presents to the emergency department with severe back pain after a low-speed motor vehicle collision. Neurological exam is intact. Radiographs are difficult to interpret due to extensive ossification. What is the most appropriate next step in management?
Explanation
Question 12
A 40-year-old female presents with a swelling in her knee joint. MRI reveals a large joint effusion with synovial hypertrophy demonstrating 'blooming artifact' on gradient-echo sequences. Biopsy confirms pigmented villonodular synovitis (PVNS/TGCT). What is the specific genetic aberration driving the overproliferation of cells in this condition?
Explanation
Question 13
Which of the following criteria is NOT part of the Mirels' scoring system for predicting the risk of a pathologic fracture in a long bone?
Explanation
Question 14
A 15-year-old male presents with bone pain and a palpable mass in his distal femur. Biopsy reveals malignant, spindle-shaped cells producing disorganized osteoid. Genetic testing of the tumor cells identifies a mutation in the TP53 gene. Which familial cancer syndrome is most commonly associated with this genetic profile?
Explanation
Question 15
A 35-year-old male presents with right hip pain. Radiographs reveal a benign-appearing, asymptomatic sessile osteochondroma of the proximal femur that has been stable for 15 years. The patient notes recent rapid growth and increasing pain. What MRI finding is most highly predictive of malignant transformation to a secondary chondrosarcoma?
Explanation
Question 16
A newborn is diagnosed with a skeletal dysplasia characterized by rhizomelic shortening of the limbs, a large head with frontal bossing, and a midface hypoplasia. The condition is inherited in an autosomal dominant pattern, though 80% are de novo mutations linked to advanced paternal age. What is the fundamental cellular defect?
Explanation
Question 17
A 6-year-old girl is evaluated for multiple recurrent long bone fractures with minimal trauma. Examination reveals blue sclerae and mild hearing loss. Radiographs show osteopenia and multiple healed fractures. Which of the following genes is most likely mutated in this patient?
Explanation
Question 18
A 12-year-old girl presents with precocious puberty, cafe-au-lait spots with irregular 'coast of Maine' borders, and a radiolucent 'ground glass' lesion in her proximal femur causing a shepherd's crook deformity. What is the underlying pathophysiology of her bone disease?
Explanation
Question 19
A 60-year-old female complains of right knee pain, stiffness, and swelling. Aspiration yields cloudy, low-viscosity fluid. Polarized light microscopy reveals rhomboid-shaped, positively birefringent crystals. This finding is most frequently associated with which of the following metabolic conditions?
Explanation
Question 20
A patient is evaluated for suspected Complex Regional Pain Syndrome (CRPS) Type I six months after an ankle fracture. According to the Budapest Criteria for the clinical diagnosis of CRPS, the patient must report at least one symptom in three of four categories. Which of the following is NOT one of the designated categories?
Explanation
Question 21
A 68-year-old male presents with generalized bone pain, lethargy, and recurrent respiratory infections. Radiographs demonstrate multiple punched-out lytic lesions in the skull and axial skeleton.
What is the most appropriate initial screening laboratory test to establish the underlying diagnosis?
Explanation
Question 22
A 9-year-old boy presents with severe, aching bilateral leg pain, a waddling gait, and progressive muscle weakness. Radiographs demonstrate marked, symmetrical cortical thickening of the diaphyseal regions of the femurs and tibias.
What is the genetic mutation responsible for this specific condition?
Explanation
Question 23
A 55-year-old female presents 8 weeks after closed reduction and casting of a distal radius fracture. She reports intense, burning pain, swelling, and vasomotor changes in her hand. Radiographs show patchy periarticular osteopenia.
Which of the following prophylactic measures has been prospectively shown to reduce the incidence of this condition when administered at the time of injury?
Explanation
Question 24
A 65-year-old man presents with intractable back pain. Radiographs reveal diffuse osteopenia and a vertebral compression fracture, while a skull radiograph shows punched-out lytic lesions.
What is the most definitive test to confirm the underlying diagnosis?
Explanation
Question 25
A 10-year-old child presents with bilateral leg pain and a waddling gait. Radiographs show symmetric, severe cortical thickening of the diaphyseal regions of the long bones.
What is the genetic mutation associated with this skeletal dysplasia?
Explanation
Question 26
A 45-year-old female is treated conservatively for a distal radius fracture. Eight weeks later, she develops severe burning pain out of proportion to the injury, along with skin changes and stiffness. Radiographs show patchy, periarticular osteopenia.
What is the best pharmacologic prophylaxis that could have been prescribed at the time of injury to reduce her risk of developing this condition?
Explanation
Question 27
A 62-year-old patient with known multiple myeloma presents with a symptomatic lytic lesion in the proximal femur. The lesion involves 60% of the cortex, and the Mirels score is calculated to be 10. What is the most appropriate next step in management?
Explanation
Question 28
Progressive Diaphyseal Dysplasia (Camurati-Engelmann disease) is a rare sclerosing bone dysplasia. Which of the following is the most common clinical presentation in childhood?
Explanation
Question 29
A 35-year-old male develops chronic, severe burning pain and allodynia in his forearm following a recognized median nerve injury from a glass laceration. What feature distinguishes his diagnosis of CRPS Type II from CRPS Type I?
Explanation
Question 30
A 30-year-old female presents with distal femur pain. Imaging reveals an eccentric, lytic, epiphyseal-metaphyseal lesion extending to the subchondral bone. Biopsy confirms Giant Cell Tumor (GCT). If medical therapy is considered, what is the mechanism of action of Denosumab?
Explanation
Question 31
A 4-year-old child with achondroplasia presents with progressively worsening lower extremity weakness, apnea, and hyperreflexia. What is the most likely anatomic cause of these symptoms?
Explanation
Question 32
In a patient with advanced rheumatoid arthritis evaluating the cervical spine, which radiographic parameter indicates the highest risk for progressive neurologic deficit and dictates the need for surgical stabilization?
Explanation
Question 33
A 16-year-old male is diagnosed with a conventional high-grade osteosarcoma of the distal femur. He undergoes 10 weeks of neoadjuvant chemotherapy followed by wide surgical resection. What is the most significant prognostic factor for long-term survival in this patient?
Explanation
Question 34
A 12-year-old boy presents with a permeative lytic lesion in the femoral diaphysis and an 'onion skin' periosteal reaction. Cytogenetics reveal a t(11;22) translocation. Which of the following fusion genes confirms the diagnosis?
Explanation
Question 35
A 55-year-old patient presents with localized bone pain and a single lytic lesion in the ilium without any other symptomatic sites.
What strict criteria must be met to diagnose a Solitary Bone Plasmacytoma rather than Multiple Myeloma?
Explanation
Question 36
A 6-year-old girl with blue sclerae, normal stature, and a history of three long bone fractures is diagnosed with Osteogenesis Imperfecta (OI) Type I. Which of the following best describes the underlying collagen defect?
Explanation
Question 37
A 55-year-old male presents with podagra. Joint fluid aspiration reveals negatively birefringent, needle-shaped crystals. For long-term chronic management, he is prescribed Allopurinol. What is its mechanism of action?
Explanation
Question 38
A 15-year-old boy presents with severe, dull aching pain in his proximal thigh that worsens at night and is dramatically relieved by ibuprofen. Imaging shows an 8mm intracortical radiolucent nidus with dense surrounding sclerosis. What is the standard of care for definitive, minimally invasive treatment?
Explanation
Question 39
A 40-year-old woman develops CRPS Type I of the hand and wrist.
She is completely intolerant of physical therapy due to extreme allodynia, and she has failed NSAIDs, gabapentin, and oral steroids. Which intervention is most appropriate next to facilitate active range of motion therapy?

Explanation
Question 40
A 25-year-old male with Multiple Hereditary Exostoses (MHE) presents with a rapidly enlarging and increasingly painful osteochondroma on his proximal tibia. Which of the following is the most critical complication to rule out?
Explanation
Question 41
During preoperative planning for a total hip arthroplasty in a patient with severe rheumatoid arthritis, the surgeon evaluates for acetabular protrusio. Which radiographic finding confirms this diagnosis on an AP pelvis radiograph?
Explanation
Question 42
A 70-year-old man presents with progressive hearing loss and increasing hat size. Radiographs demonstrate thickened cortices and coarsened trabeculae in the skull and pelvis. Paget's disease is diagnosed. The mixed phase of this disease is characterized by which of the following cellular activities?
Explanation
Question 43
The mnemonic 'CRAB' is used to recall the hallmark end-organ damage manifestations of Multiple Myeloma. Which of the following accurately represents the CRAB criteria?
Explanation
Question 44
A 65-year-old male presents with new-onset back pain, fatigue, and hypercalcemia. Radiographs show multiple punched-out lytic lesions in the axial skeleton, as seen in the provided image. Which laboratory finding is most specific for confirming the diagnosis of this pathology?
Explanation
Question 45
A 12-year-old boy presents with severe leg pain, waddling gait, and muscle weakness. Radiographs demonstrate bilateral cortical thickening of the femoral and tibial diaphyses. A mutation in which of the following genes is responsible for this condition?
Explanation
Question 46
A 45-year-old female presents 8 weeks after ORIF of a distal radius fracture with severe burning pain, swelling, and shiny skin. Radiographs show patchy osteopenia. Which prophylactic medication given post-operatively could have significantly reduced her risk of developing this condition?
Explanation
Question 47
In the pathophysiology of multiple myeloma bone disease, which cytokine pathway is primarily responsible for the uncoupled osteoclast activation leading to the characteristic lytic lesions?
Explanation
Question 48
According to the Budapest criteria for the clinical diagnosis of Complex Regional Pain Syndrome (CRPS), which of the following symptom categories is NOT part of the diagnostic requirement?
Explanation
Question 49
What is the first-line medical treatment for managing severe bone pain and improving clinical symptoms in patients with Camurati-Engelmann disease (progressive diaphyseal dysplasia)?
Explanation
Question 50
A 60-year-old male with multiple myeloma presents with severe thigh pain on weight-bearing. Radiographs show a 4 cm lytic lesion in the subtrochanteric region with 50% cortical destruction. What is the most appropriate management?
Explanation
Question 51
A 4-year-old boy with achondroplasia presents with progressively worsening lower extremity weakness, central sleep apnea, and hyperreflexia. Evaluation of which anatomical region is most critical in this scenario?
Explanation
Question 52
A 32-year-old female presents with a purely lytic, eccentric lesion in the distal femoral epiphysis. Biopsy reveals multinucleated giant cells in a background of mononuclear cells. The true neoplastic cells in this tumor express high levels of which marker?
Explanation
Question 53
A 55-year-old female with long-standing rheumatoid arthritis is scheduled for a total knee arthroplasty. Flexion-extension cervical spine radiographs reveal an anterior atlantoaxial subluxation (AAS) of 9 mm and a posterior atlantodental interval (PADI) of 12 mm. What is the most appropriate next step?
Explanation
Question 54
In the treatment of conventional high-grade osteosarcoma, which specific finding is the most important independent prognostic factor for long-term survival?
Explanation
Question 55
A 14-year-old boy presents with a permeative lytic lesion in the femoral diaphysis with an "onion skin" periosteal reaction. A biopsy shows small round blue cells. Molecular analysis is most likely to reveal which of the following translocations?
Explanation
Question 56
In the evaluation of medial compartment osteoarthritis of the knee, which dynamic gait parameter is most closely correlated with disease severity and progression?
Explanation
Question 57
A child is diagnosed with Osteogenesis Imperfecta Type I, which presents with mild bone fragility and blue sclerae. Which of the following best describes the underlying collagen defect in this specific type?
Explanation
Question 58
A 65-year-old male presents with acute severe pain and swelling in his knee. Joint aspiration reveals cloudy fluid. Polarized light microscopy shows weakly positively birefringent rhomboid-shaped crystals. This arthropathy is most strongly associated with which underlying condition?
Explanation
Question 59
A 55-year-old female sustains a distal radius fracture. To prevent the complication shown in the radiograph
, what pharmacological prophylaxis has historically been recommended during the conservative management of this injury?

Explanation
Question 60
A 65-year-old male presents with severe mechanical back pain. A skeletal survey demonstrates multiple punched-out lytic lesions in the skull and spine.
Which of the following molecules, secreted by the malignant cells in this condition, is primarily responsible for the uncoupling of bone remodeling by directly inhibiting osteoblast differentiation?
Explanation
Question 61
A 48-year-old female presents 12 weeks after a closed reduction of a distal radius fracture complaining of severe, burning hand pain. Examination reveals glossy, erythematous skin, profound stiffness, and hypersensitivity.
Which of the following criteria is the internationally accepted standard for diagnosing this condition?
Explanation
Question 62
A 10-year-old boy presents with progressive, deep-aching leg pain and a waddling gait. Radiographs reveal symmetrical, bilateral cortical thickening of the long bone diaphyses, sparing the metaphyses and epiphyses.
The pathogenesis of this disease is linked to a mutation in which of the following genes?
Explanation
Question 63
A 6-month-old infant is evaluated for short limbs and a prominent forehead. Genetic testing confirms an activating mutation in the FGFR3 gene. At the cellular level within the physis, this mutation primarily results in which of the following?
Explanation
Question 64
A 28-year-old female presents with knee pain. Radiographs show an eccentric, lytic epiphyseal lesion in the distal femur. Biopsy reveals multinucleated giant cells interspersed among mononuclear spindle cells. She is prescribed denosumab. What is the precise cellular target and mechanism of this medication in her condition?
Explanation
Question 65
An 11-year-old boy presents with a painful, swollen mid-thigh. Radiographs demonstrate a destructive diaphyseal lesion with an 'onion skin' periosteal reaction. Histology shows sheets of small, round, blue cells. Which chromosomal translocation is most classically associated with this malignancy?
Explanation
Question 66
A 16-year-old girl with distal femur osteosarcoma undergoes 10 weeks of neoadjuvant chemotherapy, followed by a wide surgical resection. Pathological analysis of the resected specimen is performed. Which of the following is the most important prognostic factor for her long-term survival?
Explanation
Question 67
A 60-year-old woman with long-standing rheumatoid arthritis presents with neck pain, bilateral hand clumsiness, and hyperreflexia. Lateral flexion-extension radiographs reveal anterior atlantoaxial subluxation. Which of the following radiographic parameters is the most reliable predictor of neurologic deficit and the potential for recovery after surgery?
Explanation
Question 68
A 62-year-old man presents with an impending pathologic fracture of the proximal femur secondary to a biopsy-proven metastatic renal cell carcinoma lesion. Prophylactic intramedullary nailing is planned. What is the most critical step in management immediately prior to surgical fixation?
Explanation
Question 69
A 22-year-old female undergoes corrective osteotomy for a 'shepherd's crook' deformity of the proximal femur. Pathology demonstrates a stroma of bland spindle cells with irregularly shaped trabeculae of woven bone lacking osteoblastic rimming. This condition is caused by a somatic activating mutation in which gene?
Explanation
Question 70
A 32-year-old man presents with recurrent, spontaneous hemarthroses of the knee. MRI demonstrates a nodular synovial mass with prominent 'blooming artifact' on gradient-echo sequences. The pathophysiology of this condition involves the overexpression of which of the following factors?
Explanation
Question 71
A 55-year-old man presents with acute, excruciating pain and swelling in his first metatarsophalangeal joint. Joint aspiration yields cloudy fluid. Under polarized light microscopy, which of the following findings confirms the diagnosis of gout?
Explanation
Question 72
A 12-year-old boy with a family history of bone bumps presents with multiple cartilage-capped bony outgrowths around his knees and wrists. He is diagnosed with Multiple Hereditary Exostoses. The genetic mutations responsible for this condition disrupt normal physeal growth by impairing which cellular process?
Explanation
Question 73
A newborn is noted to have a large anterior fontanelle, delayed closure of cranial sutures, and hypermobility of the shoulders, allowing them to be approximated in the anterior midline. Radiographs reveal hypoplastic clavicles. This condition is caused by a mutation in a gene essential for the differentiation of which cell type?
Explanation
Question 74
A 4-year-old child presents with short-limbed dwarfism, frontal bossing, and midface hypoplasia. Radiographs show narrowing of the interpedicular distances in the lumbar spine. Which genetic mutation and receptor anomaly are responsible for this condition?
Explanation
Question 75
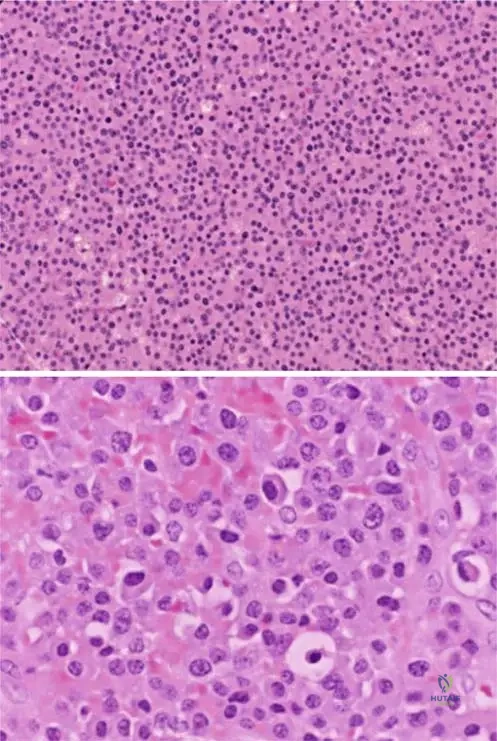
A 70-year-old man presents with severe back pain and anemia. Radiographs demonstrate multiple lytic skull lesions.
Serum electrophoresis shows an M-spike. Which of the following is the most likely finding on bone marrow biopsy?
Explanation
Question 76
A 55-year-old male undergoes arthrocentesis for a swollen, painful knee. Synovial fluid analysis reveals negatively birefringent, needle-shaped crystals under polarized light microscopy. What is the composition of these crystals?
Explanation
Question 77
A 32-year-old female presents with knee pain. Radiographs show an eccentric, purely lytic lesion in the distal femur epiphysis extending to the subchondral bone. A biopsy reveals multinucleated giant cells. Which of the following targeted therapies is most appropriate for unresectable disease?
Explanation
Question 78
A 6-year-old boy has sustained multiple low-energy fractures. Examination shows blue sclerae and mild hearing loss. The primary underlying defect in this condition involves which of the following?
Explanation
Question 79
A 14-year-old boy has a permeative, destructive lesion in the distal femur with a "sunburst" periosteal reaction. Biopsy confirms high-grade intramedullary osteosarcoma. What is the single most important prognostic factor for his long-term survival?
Explanation
Question 80
A 50-year-old female presents 3 months after a conservatively treated distal radius fracture with a stiff, swollen, erythematous hand, and severe allodynia. Radiographs show periarticular osteopenia.
What is the primary autonomic nervous system dysfunction mediating her symptoms?
Explanation
Question 81
A 60-year-old woman with long-standing rheumatoid arthritis presents with new-onset myelopathy. Flexion-extension cervical radiographs reveal an atlantodental interval (ADI) of 10 mm. Which ligament's failure is primarily responsible for this radiographic finding?
Explanation
Question 82
A 12-year-old boy presents with thigh pain and fever. Radiographs show a diaphyseal lytic lesion of the femur with an "onion-skin" periosteal reaction. Biopsy shows small blue round cells. Which chromosomal translocation is most characteristically associated with this tumor?
Explanation
Question 83
A 10-year-old girl exhibits hypermobility of her shoulders allowing them to meet in the midline. She also has delayed eruption of permanent teeth. What is the most likely genetic mutation responsible for her condition?
Explanation
Question 84
A 65-year-old man presents with chronic hip pain. Radiographs show a large destructive lesion in the ilium with "rings and arcs" calcification. Biopsy confirms a grade II conventional chondrosarcoma. What is the most appropriate primary treatment?
Explanation
Question 85
A 65-year-old man presents with increasing head size and dull, aching pain in his right thigh. Radiographs of the femur demonstrate a thickened cortex with a "blade of grass" lucency at the leading edge. What is the primary cellular defect in this condition?
Explanation
Question 86
In the pathophysiology of primary osteoarthritis, progressive articular cartilage degradation is primarily driven by upregulation of which of the following enzymes by chondrocytes?
Explanation
Question 87
A 45-year-old woman undergoes an MRI for knee pain, which reveals a 4 cm cartilage tumor in the distal femur. Which of the following features is the most reliable indicator of a grade I chondrosarcoma rather than a benign enchondroma?
Explanation
Question 88
A 16-year-old boy presents with a 6-month history of right thigh pain that is worse at night and completely relieved by ibuprofen. Radiographs show a 1 cm radiolucent nidus surrounded by dense sclerotic bone. The profound pain relief from NSAIDs is due to inhibition of which substance produced by the nidus?
Explanation
Question 89
A 15-year-old male presents with enlarging bumps around his knees and ankles. Radiographs demonstrate multiple sessile and pedunculated osteochondromas. He carries a mutation in the EXT1 gene. What is the approximate lifetime risk of malignant transformation to chondrosarcoma in this condition?
Explanation
Question 90
A newborn presents with short-limbed dwarfism, "hitchhiker" thumbs, clubfeet, and "cauliflower" ears. Radiographs reveal severely shortened first metacarpals. What is the underlying genetic defect in this dysplasia?
Explanation
Question 91
A 68-year-old male presents with fatigue, diffuse bone pain, and hypercalcemia. A representative radiograph is shown.
Serum protein electrophoresis confirms a monoclonal gammopathy. When evaluating the extent of this patient's skeletal disease, which of the following imaging modalities is most likely to yield false-negative results due to the underlying pathophysiology of the bone lesions?
Explanation
None
