Master ABOS Orthopedic Board Review: Bone Tumors & Skeletal Dysplasias | Part 10
Key Takeaway
This ABOS review covers key orthopedic bone tumors like enchondroma, giant cell tumor, fibrous dysplasia, and lymphoma, alongside skeletal dysplasias such as achondroplasia, Osteogenesis Imperfecta, Paget's disease, Ollier's disease, and osteopetrosis. It details their clinical presentation, radiographic features, and management for comprehensive board exam preparation.
Master ABOS Orthopedic Board Review: Bone Tumors & Skeletal Dysplasias | Part 10
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
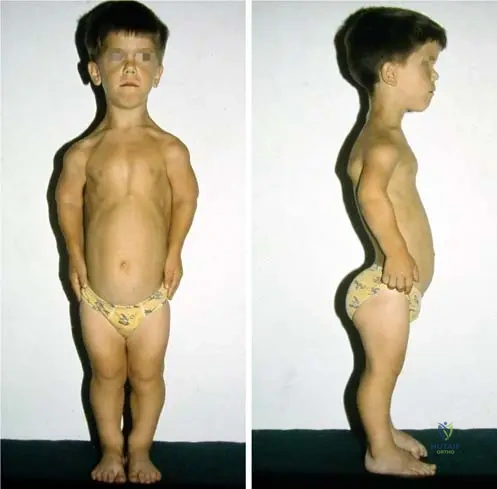
Achondroplasia is the most common form of short-limbed dwarfism. The underlying genetic defect is a gain-of-function mutation in the FGFR3 gene. Which zone of the physis is primarily affected by this mutation?
Explanation
Question 2
A 45-year-old male presents with persistent thigh pain. Radiographs show a permeative, destructive diaphyseal lesion with minimal periosteal reaction. Biopsy reveals sheets of uniform round blue cells. Immunohistochemistry is strongly positive for CD20 and CD45. What is the most appropriate initial management?
Explanation
Question 3
A 30-year-old female presents with multiple cartilaginous lesions in the phalanges and multiple soft tissue hemangiomas. Which of the following gene mutations is most strongly associated with this syndrome?
Explanation
Question 4
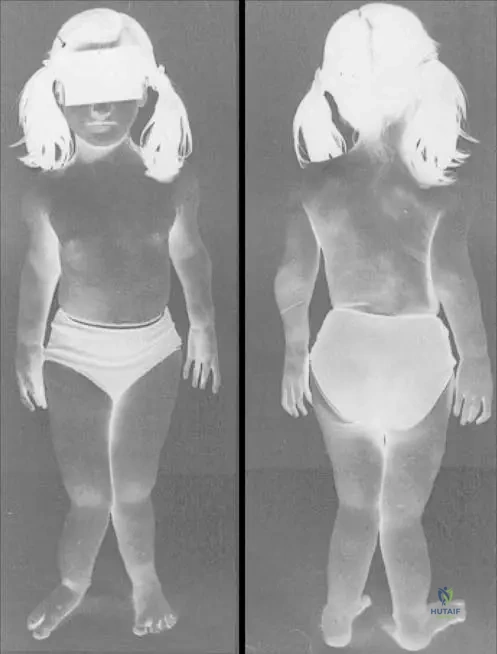
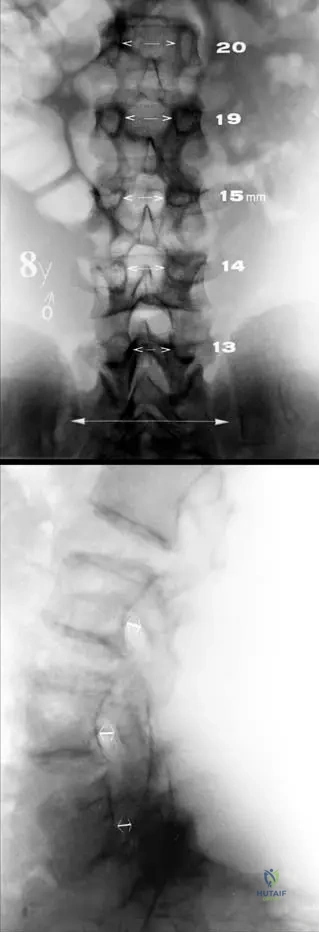
A newborn is diagnosed with a skeletal dysplasia characterized by rhizomelic shortening, frontal bossing, and midface hypoplasia. Radiographs show narrowing of the interpedicular distances in the lumbar spine. What is the inheritance pattern and associated gene mutation?
Explanation
Question 5
A 32-year-old female presents with a purely lytic, eccentric lesion in the distal femur extending to the subchondral bone. Biopsy confirms giant cell tumor of bone. Neoadjuvant therapy with denosumab is considered. What is the mechanism of action of this drug?
Explanation
Question 6
A 45-year-old male with achondroplasia presents with progressive neurogenic claudication. The most common cause of lumbar spinal stenosis in this patient population is:
Explanation
Question 7
A 50-year-old male with Ollier disease presents with new-onset, progressive pain in his proximal humerus over the last 3 months. Radiographs demonstrate a pre-existing cartilaginous lesion now showing endosteal scalloping > 2/3 of cortical thickness and a new soft tissue mass. What is the most likely diagnosis?
Explanation
Question 8
An infant presents with short limbs and frontal bossing. Radiographs show narrowing of interpedicular distances from L1 to L5.
What is the primary cellular mechanism affected by the genetic mutation in this condition?
Explanation
Question 9
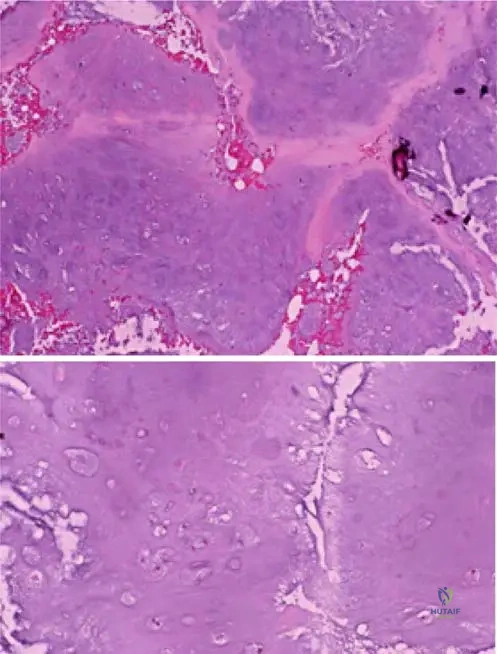
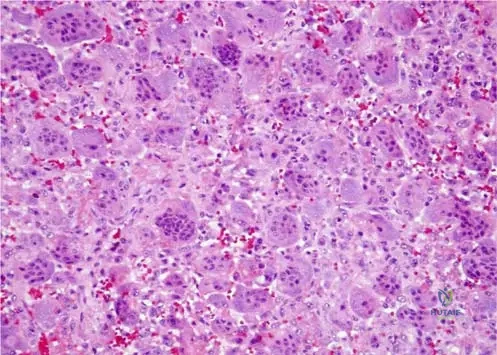
A 32-year-old male presents with knee pain. Radiographs reveal an eccentric, lytic epiphyseal lesion in the distal femur. Biopsy reveals multinucleated giant cells and mononuclear stromal cells.
Which cell population harbors the neoplastic mutation, and what marker do they overexpress?
Explanation
Question 10
A 65-year-old male presents with thigh pain. Radiographs show a permeative lytic lesion in the femoral diaphysis. MRI demonstrates a massive soft tissue mass, yet the cortical bone appears structurally intact on CT. Biopsy confirms primary bone lymphoma.
What is the most appropriate initial management for this lesion assuming no impending fracture?
Explanation
Question 11
Which of the following skeletal dysplasias is characterized by a mutation in the RUNX2 (CBFA1) gene, delayed closure of cranial sutures, and supernumerary teeth?
Explanation
Question 12
A 45-year-old female is diagnosed with multiple enchondromas predominantly affecting her right arm and leg, as well as multiple soft-tissue hemangiomas.
Which of the following statements is true regarding her condition?
Explanation
Question 13
A 4-year-old boy presents with short trunk dwarfism, prominent joints, myopia, and coxa vara. Cervical spine radiographs demonstrate odontoid hypoplasia. What is the genetic basis of this disorder?
Explanation
Question 14
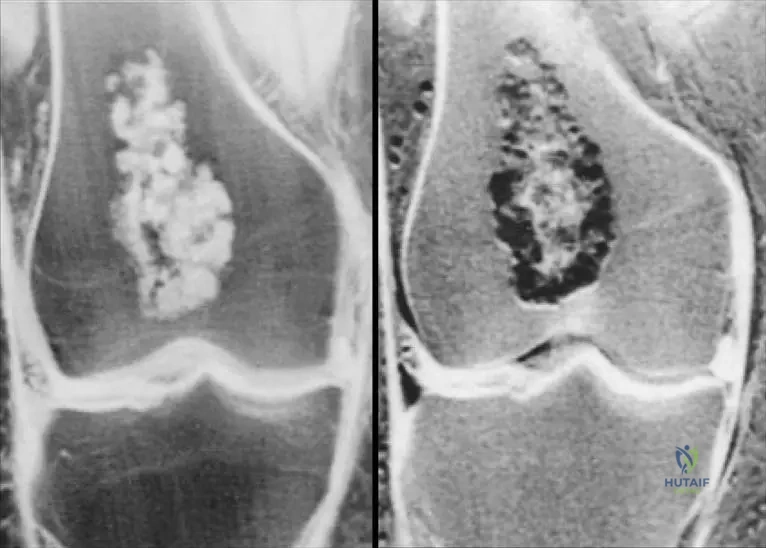
An asymptomatic 30-year-old woman undergoes hand radiography following minor trauma, revealing a well-circumscribed, 1 cm central lytic lesion with stippled calcifications in the proximal phalanx.
There is no cortical breakthrough. What is the most appropriate management?
Explanation
Question 15
A patient with achondroplasia
requires spinal surgery for severe neurogenic claudication. What anatomical feature of the lumbar spine primarily contributes to this stenosis?
Explanation
Question 16
A newborn is diagnosed with achondroplasia. Which of the following accurately describes the molecular pathophysiology of this skeletal dysplasia?
Explanation
Question 17
A 32-year-old woman presents with knee pain. Radiographs show an eccentric, lytic epiphyseal-metaphyseal lesion of the distal femur. Biopsy confirms a Giant Cell Tumor. If she is treated with denosumab preoperatively, which histological change is most expected?
Explanation
Question 18
A 65-year-old man presents with thigh pain. Radiographs reveal a permeative, moth-eaten diaphyseal lesion in the femur with minimal periosteal reaction. Biopsy shows small, round blue cells that stain positive for CD45 and CD20. What is the most appropriate primary treatment for an uncomplicated presentation of this disease?
Explanation
Question 19
A 28-year-old man sustains a minor trauma to his right ring finger and develops acute pain. Radiographs demonstrate a centrally located lytic lesion in the proximal phalanx with a pathologic fracture. What is the most appropriate management after the fracture heals?
Explanation
Question 20
A 15-year-old girl presents with multiple asymmetric cartilaginous lesions in the appendicular skeleton and bluish, compressible subcutaneous nodules on her extremities. Which of the following is true regarding her condition?
Explanation
Question 21
Parents of a 6-month-old infant with achondroplasia report that the child has episodes of sleep apnea, snoring, and difficulty feeding. Neurological exam reveals hyperreflexia in the lower extremities. What is the most critical next step in management?
Explanation
Question 22
In a Giant Cell Tumor of bone, which specific cell population harbors the pathognomonic H3F3A mutation and is considered the true neoplastic component?
Explanation
Question 23
A skeletal survey of a child with achondroplasia will typically demonstrate which of the following pathognomonic pelvic radiographic findings?
Explanation
Question 24
A 4-year-old child with disproportionate short stature is diagnosed with achondroplasia. What is the underlying genetic mutation and its typical inheritance pattern?
Explanation
Question 25
A 3-year-old child with achondroplasia presents with delayed motor milestones, hypotonia, and signs of central sleep apnea.
Which of the following is the most appropriate initial diagnostic imaging modality?
Explanation
Question 26
A 32-year-old female presents with progressive knee pain. Radiographs demonstrate an eccentric, lytic, epiphyseal-metaphyseal lesion of the distal femur extending to the subchondral bone.
Biopsy confirms a Giant Cell Tumor of bone. Which cell type is considered the primary neoplastic cell in this lesion?
Explanation
Question 27
In the management of a massive, unresectable recurrent giant cell tumor of the sacrum, which of the following targeted medical therapies is the most appropriate primary treatment?
Explanation
Question 28
A 65-year-old male presents with severe, unremitting thigh pain. Radiographs demonstrate a permeative, moth-eaten diaphyseal lesion in the femur with minimal periosteal reaction.
Biopsy reveals sheets of small round blue cells that stain positive for CD20. What is the most likely diagnosis?
Explanation
Question 29
A 45-year-old asymptomatic male is found to have an incidental well-defined medullary lesion in the proximal humerus with stippled "arcs and rings" calcifications.
Which MRI finding most strongly suggests transformation to a low-grade chondrosarcoma rather than a benign enchondroma?
Explanation
Question 30
A 12-year-old boy presents with multiple unilateral enchondromas causing limb-length discrepancy and angular deformity.
Physical examination reveals no cutaneous or soft tissue hemangiomas. What is the diagnosis, and what is the estimated lifetime risk of malignant transformation?
Explanation
Question 31
An adult male with achondroplasia presents with bilateral leg heaviness, weakness, and progressive neurogenic claudication.
What is the primary anatomical etiology of his spinal stenosis?
Explanation
Question 32
A 28-year-old patient undergoes extended intralesional curettage for a Campanacci Grade II giant cell tumor of the proximal tibia.
Which of the following surgical adjuncts is most commonly utilized to decrease the rate of local recurrence?
Explanation
Question 33
A 50-year-old female is diagnosed with primary diffuse large B-cell lymphoma of the right humerus. There is no impending or actual pathologic fracture.
What is the mainstay of treatment for this condition?
Explanation
Question 34
Which of the following structural defects is primarily responsible for the clinical manifestations seen in patients with Osteogenesis Imperfecta?
Explanation
Question 35
A 5-year-old child presents with disproportionate short stature, normal facies, and marked joint laxity. Radiographs demonstrate delayed epiphyseal ossification and irregular metaphyses. Genetic testing reveals a mutation in the COMP (Cartilage Oligomeric Matrix Protein) gene. What is the most likely diagnosis?
Explanation
Question 36
A 35-year-old male with a history of a distal radius giant cell tumor presents 2 years post-resection. Routine chest imaging reveals multiple small pulmonary nodules. Biopsy of a nodule confirms benign GCT histology. What is this phenomenon called, and what is its typical clinical behavior?
Explanation
Question 37
A 32-year-old female presents with an incidental finding on a hand radiograph taken after mild trauma. The image shows a well-defined lucency with stippled calcification in the proximal phalanx, with no cortical breakthrough or soft tissue mass. What is the most appropriate next step in management?
Explanation
Question 38
A 28-year-old female presents with knee pain. Radiographs show an eccentric, lytic epiphyseal lesion extending to the subchondral bone. Biopsy confirms a tumor characterized by mononuclear stromal cells and multinucleated giant cells. Which of the following best describes the mechanism of the targeted medical therapy for this condition?

Explanation
Question 39
Parents bring their 6-month-old infant with short-limbed dwarfism for evaluation. The child has hypotonia and hyperreflexia. An MRI of the cervicomedullary junction is ordered. What is the primary cause of the underlying pathology at this anatomical site in this condition?

Explanation
Question 40
A 55-year-old male presents with deep knee pain. Radiographs reveal a permeative diaphyseal lesion in the distal femur. Biopsy confirms primary non-Hodgkin lymphoma of bone. Which of the following is true regarding this condition?
Explanation
Question 41
A 14-year-old boy has multiple painless bony protuberances around his knees and shoulders. Genetic testing reveals a mutation in the EXT1 gene. This mutation primarily affects which of the following cellular processes?
Explanation
Question 42
A 4-year-old girl with a history of multiple low-energy fractures, blue sclerae, and dentinogenesis imperfecta is started on pamidronate. What is the primary mechanism of action of this medication in treating her condition?
Explanation
Question 43
A 35-year-old male undergoes curettage and cementing for a giant cell tumor (GCT) of the proximal tibia. Two years later, a chest CT reveals multiple small, asymptomatic pulmonary nodules. Biopsy of a nodule confirms metastatic GCT. What is the most appropriate next step in management?
Explanation
Question 44
A 40-year-old male with achondroplasia presents with progressive neurogenic claudication. He is diagnosed with severe lumbar spinal stenosis. Which of the following anatomical anomalies is the primary contributor to his stenosis?
Explanation
Question 45
A 25-year-old male presents with multiple asymmetric enchondromas predominantly involving the right side of his body, without any associated soft tissue vascular lesions. What is his estimated lifetime risk of malignant transformation to chondrosarcoma?
Explanation
Question 46
A newborn is evaluated for skeletal dysplasia. Physical examination reveals short limbs, clubfeet, 'hitchhiker' thumbs, and cystic swelling of the external ears (cauliflower ears). Which of the following gene mutations is most likely responsible for this phenotype?
Explanation
Question 47
A 12-year-old boy presents with a painful, swollen thigh and low-grade fever. Radiographs show a permeative diaphyseal lesion with an 'onion skin' periosteal reaction. Which of the following cytogenetic abnormalities is most characteristic of this tumor?
Explanation
Question 48
A 16-year-old boy presents with nocturnal back pain relieved by NSAIDs. Imaging reveals a 7mm intracortical nidus in the lamina of L4, located 4 mm from the traversing L4 nerve root. Which of the following is the most appropriate definitive management?
Explanation
Question 49
An adult patient with a known solitary enchondroma of the proximal humerus presents with new-onset, progressive pain at rest. Imaging reveals endosteal scalloping greater than two-thirds of the cortical thickness and cortical breakthrough. What is the most likely diagnosis?
Explanation
Question 50
A 15-year-old boy presents with the ability to appose his shoulders at the midline. He has delayed eruption of permanent teeth and an unusually wide face. Radiographs show absent clavicles. This condition is primarily due to a defect in which of the following?
Explanation
Question 51
A 6-year-old boy presents with recurrent fractures, anemia, and hepatosplenomegaly. Radiographs reveal a 'bone-within-a-bone' appearance and generalized osteosclerosis. What is the most definitive curative treatment for the underlying systemic disease?
Explanation
Question 52
A 32-year-old female presents with knee pain. Radiographs show an eccentric, lytic epiphyseal lesion in the distal femur.
Biopsy confirms multinucleated giant cells interspersed among mononuclear cells. Which genetic mutation is highly specific and diagnostic for this neoplasm?
Explanation
Question 53
A 4-year-old boy with a known skeletal dysplasia presents for a routine evaluation.
Given his condition (achondroplasia), radiographs of the lumbar spine are most likely to demonstrate which of the following characteristic findings?
Explanation
Question 54
A 45-year-old asymptomatic male has an incidental finding on a knee radiograph obtained after minor trauma.
The lesion is centrally located in the metaphysis, demonstrating stippled calcification without cortical destruction or periosteal reaction. What is the most appropriate next step in management?
Explanation
Question 55
Primary bone lymphoma is a rare malignancy that most commonly affects the metaphysis or diaphysis of long bones.
Which of the following is the most significant prognostic factor for long-term survival in primary bone lymphoma?

Explanation
Question 56
A 6-year-old child presents with a history of frequent long bone fractures, blue sclerae, and early-onset hearing loss. A genetic defect in which of the following processes is primarily responsible for this clinical presentation?
Explanation
Question 57
A 12-year-old boy presents with localized pain, fever, and weight loss. Radiographs reveal a permeative lesion in the femoral diaphysis with an "onion-skin" periosteal reaction. Cytogenetic testing reveals a t(11;22) translocation. Which fusion protein is most commonly produced by this genetic alteration?
Explanation
Question 58
A 16-year-old male complains of chronic hip pain. Radiographs reveal a 2 cm well-circumscribed, lytic lesion in the greater trochanter apophysis with fine matrix calcifications. Histology shows polygonal mononuclear cells with clefted nuclei and "chicken-wire" calcification. What is the standard treatment?
Explanation
Question 59
A 25-year-old female presents with a progressive "shepherd's crook" deformity of her right proximal femur. She also reports a history of precocious puberty and has large, irregular café-au-lait macules. This condition is caused by a mutation in the GNAS gene, leading to overactivity of which cellular messenger?
Explanation
Question 60
An infant presents with failure to thrive, hepatosplenomegaly, and severe anemia. Radiographs show diffusely dense bones with a "bone-within-bone" appearance in the metaphyses. A mutation impairing which of the following cellular mechanisms is most likely responsible?
Explanation
Question 61
A 14-year-old male with multiple painless, bony bumps around his knees and shoulders is diagnosed with Multiple Hereditary Exostoses (MHE). He asks about his risk of malignant transformation. The highest risk is malignant transformation into which of the following?
Explanation
Question 62
Denosumab is increasingly used in the neoadjuvant management of unresectable or complex giant cell tumors of bone.
What is the specific target of this monoclonal antibody?
Explanation
Question 63
A newborn is noted to have severe short-limbed dwarfism, a "hitchhiker" thumb deformity, clubfeet, and cystic swelling of the external ear (cauliflower ear). Which of the following genes is mutated in this autosomal recessive skeletal dysplasia?
Explanation
Question 64
A 5-year-old girl with normal intelligence, short-trunk dwarfism, and corneal clouding is diagnosed with Morquio syndrome (Mucopolysaccharidosis Type IV). Which orthopedic complication must be urgently screened for due to a high risk of catastrophic neurologic injury?
Explanation
Question 65
A 15-year-old patient is evaluated for delayed dental eruption, open cranial sutures, and abnormal shoulder mobility, allowing them to approximate their shoulders anteriorly. This autosomal dominant condition is caused by a mutation in the RUNX2 (CBFA1) gene. This gene normally controls the differentiation of which cell type?
Explanation
Question 66
A 19-year-old male presents with severe nocturnal pain in the proximal tibia that is completely relieved by oral ibuprofen. Imaging shows a 1.2 cm radiolucent nidus surrounded by thick cortical sclerosis. Which specific cell type is primarily responsible for the excessive prostaglandin E2 (PGE2) production in this lesion?
Explanation
Question 67
A 6-year-old child presents with short-limbed dwarfism, a waddling gait, and prominent joint laxity. Unlike achondroplasia, the child has a completely normal facial appearance. Radiographs show delayed epiphyseal ossification and irregular metaphyses. A mutation in which of the following genes is responsible?
Explanation
Question 68
A 15-year-old female presents with a rapidly enlarging, painful mass in her distal radius. Radiographs show an eccentric, expansile lytic lesion with a thin "eggshell" cortex. MRI reveals multiple fluid-fluid levels. Which genetic rearrangement is highly characteristic of the primary form of this lesion?
Explanation
Question 69
A 65-year-old male presents with increasing hat size, asymmetric hearing loss, and bowing of his right tibia. Laboratory testing reveals markedly elevated alkaline phosphatase with normal serum calcium and phosphorus. Which phase of this specific disease process is characterized by intense, unregulated osteoclastic resorption?
Explanation
Question 70
A 9-year-old boy sustains a pathologic fracture of the proximal humerus after a minor fall. Radiographs show a centrally located, cystic lesion in the metaphysis extending to the physis, featuring a "fallen leaf" sign. Which of the following statements is true regarding the classification of this lesion?
Explanation
Question 71
A 16-year-old male is undergoing treatment for conventional high-grade osteosarcoma of the distal femur. After completing neoadjuvant chemotherapy, wide surgical resection is performed. Which of the following histologic findings in the resected specimen is the most important predictor of long-term survival?
Explanation
Question 72
A 28-year-old female presents with severe knee pain. Radiographs reveal an eccentric, lytic epiphyseal-metaphyseal lesion in the proximal tibia.
Biopsy is consistent with a giant cell tumor of bone. Which of the following describes the primary neoplastic cell population in this lesion?
Explanation
Question 73
A 14-month-old male with achondroplasia presents with central sleep apnea, hyperreflexia, and hypotonia.
What is the most critical next step in his evaluation?
Explanation
Question 74
A 45-year-old asymptomatic male undergoes a shoulder radiograph following mild trauma, revealing a well-defined intramedullary lesion with punctate calcifications in the proximal humerus.
There is no endosteal scalloping or cortical breakthrough. What is the most appropriate management?
Explanation
Question 75
A 60-year-old male presents with a painful, destructive lesion in his distal femur.
Biopsy confirms Primary Bone Lymphoma (Diffuse Large B-Cell type). Which of the following clinical factors portends the most favorable prognosis in this patient?

Explanation
Question 76
A 12-year-old male presents with a mixed lytic and sclerotic metaphyseal lesion of the distal femur with a 'sunburst' periosteal reaction. He has a history of poikiloderma, sparse hair, and bilateral cataracts. Which gene mutation is most likely responsible for his underlying syndrome?
Explanation
Question 77
A 14-year-old male presents with severe mid-thigh pain, swelling, and low-grade fever. Radiographs show a permeative diaphyseal lesion with an 'onion-skin' periosteal reaction. Molecular testing of the biopsy specimen is most likely to reveal which of the following translocations?
Explanation
Question 78
A 16-year-old male complains of chronic right knee pain. Radiographs show a 2 cm eccentric, purely lytic lesion in the proximal tibial epiphysis with a thin sclerotic rim. Histological examination shows mononuclear cells with grooved nuclei and areas of pericellular 'chicken-wire' calcification. What is the most likely diagnosis?
Explanation
Question 79
A 7-year-old girl is evaluated for delayed eruption of secondary teeth. Examination reveals a persistently open anterior fontanelle, hypermobility of the shoulders allowing them to meet in the midline, and short stature. The gene responsible for this condition is critical for the differentiation of which cell type?
Explanation
Question 80
A 32-year-old female presents with progressive knee pain. Radiographs reveal an eccentric, lytic epiphyseal lesion extending to the subchondral bone in the distal femur.
Biopsy confirms a giant cell tumor. She is treated preoperatively with a monoclonal antibody to facilitate joint salvage. What is the primary mechanism of action of this medication?
Explanation
Question 81
An 8-month-old infant with achondroplasia presents with delayed motor milestones, hypotonia, and witnessed episodes of central sleep apnea.
What is the most appropriate next step in evaluation?
Explanation
Question 82
A 45-year-old male sustains a minor twisting injury to his hand. Radiographs show a well-circumscribed, lucent lesion with central stippled calcifications in the proximal phalanx of the ring finger.
There is no cortical breakthrough. Which of the following mutations is most frequently associated with the development of multiple such lesions in a mostly unilateral or asymmetric distribution?
Explanation
Question 83
A 60-year-old male presents with worsening thigh pain over several months. Radiographs demonstrate a permeative, poorly marginated radiolucent lesion in the femoral diaphysis.
MRI reveals extensive soft tissue and marrow involvement that appears vastly out of proportion to the subtle cortical destruction. What is the most likely diagnosis?
Explanation
Question 84
A 45-year-old female undergoes an MRI of her shoulder for suspected rotator cuff pathology. An incidental lesion is found in the proximal humerus, corresponding to punctate calcifications seen on plain radiographs. MRI shows a lobulated high T2 signal lesion with no endosteal scalloping or cortical breakthrough.
What is the most appropriate management for this bone lesion?
Explanation
Question 85
A 25-year-old female presents with progressive knee pain. Radiographs reveal an eccentric, expansile, lytic lesion in the distal femoral epiphysis extending to the subchondral bone plate. Biopsy confirms a giant cell tumor of bone.
If pharmacological therapy with denosumab is considered, this drug specifically targets which of the following mechanisms in this pathology?
Explanation
Question 86
A 4-year-old boy with achondroplasia presents with lower extremity hyperreflexia, clumsiness, and central sleep apnea.
What is the most likely anatomic cause of these symptoms?
Explanation
Question 87
A 50-year-old male presents with deep thigh pain. Radiographs demonstrate a poorly defined, permeative lytic lesion in the femoral diaphysis with minimal cortical destruction. MRI reveals extensive marrow replacement and a large surrounding soft tissue mass.
Which of the following statements best describes primary lymphoma of bone compared to other primary bone malignancies?
Explanation
Question 88
A 10-year-old boy is referred for delayed eruption of his permanent teeth, prominent frontal bossing, and excessive shoulder mobility. Radiographs demonstrate hypoplastic clavicles and delayed ossification of the pubic symphysis. A mutation in which of the following transcription factors is responsible for this condition?
Explanation
Question 89
An 18-year-old male presents with rapid onset of pain and swelling over his distal thigh following minor trauma. Radiographs reveal a purely lytic, expansile metaphyseal lesion with cortical destruction. Biopsy shows blood-filled cystic spaces separated by septa containing highly pleomorphic spindle cells and fine, lace-like osteoid. What is the most likely diagnosis?
Explanation
Question 90
A 12-year-old boy presents with multiple hard, painless masses around his knees and ankles. Radiographs demonstrate multiple bone excrescences pointing away from the joints, with continuity of the medullary cavity into the lesions. What is the underlying pathogenesis of this condition?
Explanation
Question 91
A 7-year-old boy complains of localized mid-back pain for several weeks. A lateral radiograph of the thoracic spine reveals a "vertebra plana" at T8 with preserved disc spaces. Laboratory studies are normal. Electron microscopy of a biopsy specimen from this lesion would most likely reveal which of the following structures?
Explanation
Question 92
An infant born at 38 weeks gestation is noted to have profound osteopenia, severe limb deformities with multiple acute and healing fractures, and deep blue sclerae. The infant succumbs to respiratory failure secondary to a small, frail thorax shortly after birth. According to the Sillence classification, which type of osteogenesis imperfecta does this patient have?
Explanation
Question 93
A 15-year-old male presents with chronic knee pain. Radiographs display a well-circumscribed, eccentrically located lytic lesion with a thin sclerotic margin in the proximal tibial epiphysis. Biopsy shows polygonal mononuclear cells with longitudinally clefted nuclei and areas of "chicken-wire" intercellular calcification. Following extended curettage and bone grafting, what is the most common complication of this lesion?
Explanation
Question 94
A 9-year-old girl is evaluated for a limp and a leg-length discrepancy. Physical exam notes large café-au-lait macules with irregular, "coast of Maine" borders. She also has a history of early-onset menses. Radiographs show a polyostotic intramedullary lesion with a hazy, "ground-glass" appearance. This clinical syndrome is associated with a mutation affecting which of the following?
Explanation
Question 95
A 65-year-old man presents with severe back pain. Radiographs show multiple dense, osteoblastic lesions throughout the lumbar spine and pelvis. Laboratory evaluation reveals a significantly elevated serum prostate-specific antigen (PSA). The osteoblastic nature of these skeletal metastases is primarily driven by tumor secretion of which factor?
Explanation
Question 96
A newborn is evaluated in the NICU for marked shortening of all limbs, proximally placed "hitchhiker" thumbs, severe clubfeet, and distinct cystic swelling of the pinnae (cauliflower ears). Radiographs show short, thick long bones and a normal skull. The underlying genetic mutation in this condition primarily impairs which cellular process?
Explanation
Question 97
A 30-year-old female presents with a slow-growing, mildly painful mass in her anterior shin. Plain radiographs reveal an eccentric, multi-loculated, "soap-bubble" osteolytic lesion in the anterior tibial diaphysis. Histology shows nests of epithelial cells within a fibrous stroma. Which of the following conditions is most frequently considered a precursor or is commonly found coexisting with this specific tumor?
Explanation
Question 98
A 25-year-old male with a known history of Ollier disease presents with new, rapidly worsening pain and a palpable mass in his proximal humerus. Radiographs show a previously stable enchondroma that now exhibits cortical destruction and a soft tissue mass containing rings-and-arcs calcifications.
What is the most likely diagnosis of this new aggressive lesion?
Explanation
Question 99
A 12-month-old infant with achondroplasia presents for a routine check-up. The parents note a prominent outward curve in the child's lower back when sitting upright. Radiographs confirm a moderate thoracolumbar kyphosis.
What is the most appropriate initial management for this spinal finding?
Explanation
None
