Lunotriquetral and Triquetrohamate Arthrodesis: Operative Techniques and Protocols
Key Takeaway
Lunotriquetral arthrodesis is a definitive surgical intervention for chronic lunotriquetral instability and localized carpal arthritis. This procedure involves dorsal exposure, meticulous joint decortication, bone grafting, and rigid internal fixation, typically utilizing a triangular Kirschner wire configuration. Successful outcomes depend on precise reduction of volar intercalated segment instability (VISI) and strict adherence to a phased postoperative immobilization protocol to ensure solid osseous union and restore carpal kinematics.
INTRODUCTION TO LUNOTRIQUETRAL INSTABILITY AND ARTHRODESIS
Lunotriquetral (LT) arthrodesis is a highly specialized, definitive salvage procedure designed to address chronic lunotriquetral instability, localized degenerative arthritis, or symptomatic non-dissociative carpal instability that has proven refractory to conservative management or soft-tissue reconstruction. The lunotriquetral joint is a critical component of the proximal carpal row, and its integrity is paramount for normal radiocarpal and midcarpal kinematics.
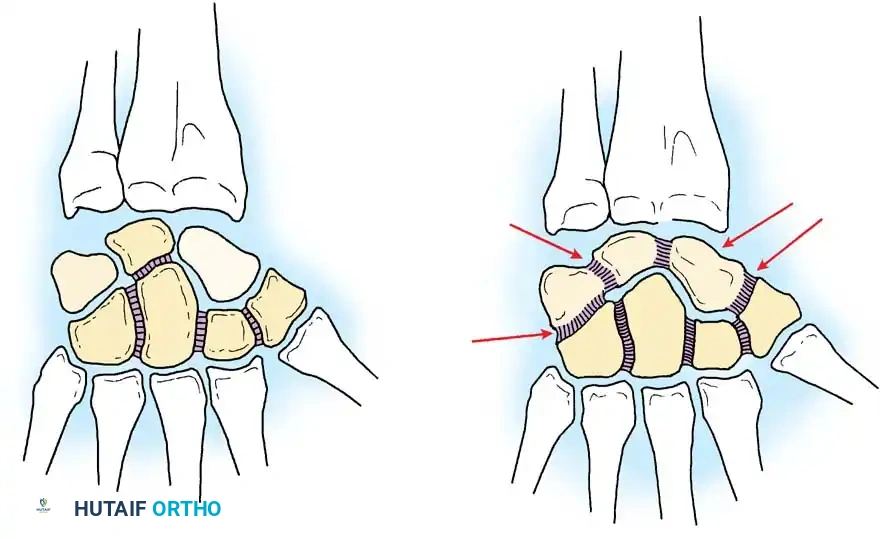
Disruption of the lunotriquetral interosseous ligament (LTIL), often combined with attenuation of the extrinsic volar radiocarpal ligaments, leads to a volar intercalated segment instability (VISI) pattern. In this biomechanical state, the lunate falls into abnormal flexion (following the scaphoid), while the triquetrum extends. When primary ligamentous repair or reconstruction is no longer viable due to tissue attenuation, fixed deformity, or the onset of chondral wear, limited intercarpal arthrodesis becomes the procedure of choice to restore a stable carpal block and alleviate ulnar-sided wrist pain.
Clinical Pearl: Lunotriquetral arthrodesis is notorious for a historically high rate of nonunion (reported between 15% and 50% in older literature). Meticulous joint decortication, the mandatory use of autologous cancellous bone graft, and rigid internal fixation are absolute prerequisites for achieving successful osseous consolidation.
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of carpal anatomy is essential for executing a successful LT arthrodesis. The proximal carpal row acts as an intercalated segment between the radius and the distal carpal row, possessing no direct tendinous insertions. Its motion is entirely dictated by articular contact forces and ligamentous tethers.
The Lunotriquetral Interosseous Ligament (LTIL)
The LTIL is a C-shaped structure divided into three distinct anatomical and biomechanical regions:
* Volar Region: The thickest and most biomechanically significant portion. It is the primary restraint to translation and rotational instability between the lunate and triquetrum.
* Membranous (Proximal) Region: Thin and avascular; primarily functions to contain synovial fluid within the radiocarpal joint. Tears here are often degenerative and may not cause gross instability.
* Dorsal Region: Thinner than the volar portion but acts as a secondary restraint to rotational forces.
Biomechanical Implications of Fusion
Fusing the lunate and triquetrum effectively creates a single osseous unit on the ulnar aspect of the proximal row. While this eliminates painful pathological motion, it alters global wrist kinematics. Patients typically experience a mild to moderate reduction in terminal wrist flexion and extension, as well as a slight decrease in radial and ulnar deviation. However, grip strength is generally improved due to the elimination of pain and the restoration of a stable fulcrum.
INDICATIONS AND CONTRAINDICATIONS
Indications
- Chronic, symptomatic lunotriquetral instability (dynamic or static VISI deformity).
- Failed prior soft-tissue reconstructions (e.g., LT ligament repair or tenodesis).
- Localized degenerative joint disease of the lunotriquetral articulation.
- Ulnar impaction syndrome with concomitant irreparable LT ligament tearing (often performed in conjunction with an ulnar shortening osteotomy).
Contraindications
- Absolute: Active local or systemic infection; advanced pancarpal arthritis; radiolunate arthritis.
- Relative: Tobacco use (significantly increases nonunion risk); non-compliant patients unable to adhere to strict postoperative casting protocols; isolated membranous LTIL tears without dynamic or static instability.
Surgical Warning: Always evaluate the radiolunate and radioscaphoid joints prior to committing to an LT arthrodesis. If radiolunate arthritis is present, a limited intercarpal fusion will fail to relieve pain, and a more extensive salvage procedure (e.g., radiocarpal arthrodesis or proximal row carpectomy) must be considered.
PREOPERATIVE PLANNING
Standard posteroanterior (PA), lateral, and specialized scaphoid/lunate views are mandatory. On the lateral radiograph, a VISI deformity is characterized by a radiolunate angle greater than 15 degrees of flexion and a scapholunate angle of less than 30 degrees.
Magnetic Resonance Imaging (MRI) or MR Arthrography can assist in evaluating the integrity of the interosseous ligaments and the vascularity of the carpal bones. However, diagnostic wrist arthroscopy remains the gold standard for evaluating the exact degree of LT instability (Geissler classification) and assessing the articular cartilage of the midcarpal and radiocarpal joints.
SURGICAL TECHNIQUE: LUNOTRIQUETRAL ARTHRODESIS
Patient Positioning and Preparation
- Place the patient in the supine position with the operative arm extended onto a radiolucent hand table.
- Apply a well-padded pneumatic tourniquet to the proximal arm.
- Administer regional anesthesia (supraclavicular or axillary brachial plexus block) or general anesthesia, according to patient and anesthesiologist preference.
- Exsanguinate the limb using an elastic wrap (Esmarch bandage) and inflate the tourniquet to 250 mm Hg (or 100 mm Hg above systolic blood pressure).
- Prepare and drape the limb in a standard sterile surgical fashion.
Surgical Approach and Exposure
- Incision: Make a 4 to 5 cm dorsal transverse incision centered over the radiocarpal joint, or a curved longitudinal incision centered over the lunotriquetral joint. The longitudinal incision allows for easier proximal extension if a distal radius bone graft is required.
- Superficial Dissection: Carefully dissect through the subcutaneous tissues. Identify and protect the dorsal sensory branches of the ulnar nerve (DSBUN) and the superficial radial nerve. Retract the dorsal venous network gently.
- Extensor Retinaculum: Incise the extensor retinaculum longitudinally over the third extensor compartment. Transpose the extensor pollicis longus (EPL) tendon radially. Elevate the retinaculum to expose the interval between the fourth (extensor digitorum communis) and fifth (extensor digiti minimi) extensor compartments.
- Capsulotomy: Enter the wrist capsule through a longitudinal incision or a ligament-sparing dorsal capsular flap (e.g., Mayo or Berger approach). Reflect the capsule to clearly identify the dorsal aspect of the scaphoid, lunate, and triquetrum.
Joint Preparation and Decortication
- Identify the lunotriquetral joint. In cases of chronic instability, the joint may be widened, and the dorsal LT ligament will be attenuated or absent.
- Use a combination of fine rongeurs, sharp osteotomes, and small curets (2.0 mm or 3.0 mm) to meticulously remove all articular cartilage and subchondral bone from the opposing articular surfaces of the lunate and triquetrum.
- Crucial Step: Decorticate down to healthy, bleeding cancellous bone on each side of the joint. The use of a high-speed burr should be minimized or accompanied by copious cold saline irrigation to prevent thermal necrosis of the delicate carpal bone, which can precipitate nonunion.
- Volar Preservation: Leave the most palmar portion of the lunotriquetral joint and the volar capsule intact. This preserves the critical volar radiocarpal ligaments (which provide essential blood supply) and acts as a volar hinge to prevent palmar extrusion of the bone graft.
Bone Grafting
- Harvest cancellous autograft. This can be obtained locally from the distal radius (e.g., Lister's tubercle) through the proximal extent of the incision, or from the iliac crest if a larger volume is required.
- Pack the decorticated lunotriquetral interval tightly with the cancellous bone graft.
Reduction and Internal Fixation
- Reduction: Reduce any instability pattern that may be present. Specifically, correct the VISI deformity by extending the flexed lunate and flexing the extended triquetrum. This can be facilitated by inserting a 0.062-inch Kirschner wire (K-wire) into each bone to act as "joysticks" for manipulation.
- Fixation: Once anatomic alignment is achieved, place four or five intercarpal K-wires (typically 0.045-inch or 0.062-inch) across the lunotriquetral joint.
- Configuration: Place the wires in a triangular or divergent configuration to maximize rotational stability and compress the arthrodesis site.
- Precautions: Place absolutely no wires across the radiocarpal joint, as this will tether the joint, damage the proximal articular surface, and lead to severe postoperative stiffness.
- Cut all K-wires beneath the skin to minimize the risk of pin tract infection and allow for prolonged casting.
Pitfall: Failure to adequately correct the VISI deformity prior to fixation will result in a malunion of the carpal block, leading to altered radiocarpal contact stresses, restricted motion, and accelerated secondary osteoarthritis.
Radiographic Confirmation and Closure
- Obtain intraoperative fluoroscopic radiographs (PA, lateral, and oblique views) to ascertain the satisfactory position of the carpal bones, complete correction of the VISI deformity, and the precise intraosseous placement of the internal fixation.
- Deflate the tourniquet and achieve meticulous hemostasis using bipolar electrocautery.
- Close the dorsal wrist capsule securely with interrupted absorbable sutures (e.g., 3-0 Vicryl) to prevent extensor tendon bowstringing and provide a barrier over the carpus.
- Repair the extensor retinaculum, leaving the EPL transposed subcutaneously if necessary to prevent friction over the closure.
- Close the skin with nonabsorbable sutures (e.g., 4-0 Nylon) or skin staples.
- Apply a sterile, nonadherent dressing followed by a well-molded, long-arm thumb spica cast with the wrist in neutral to slight extension and the forearm in neutral rotation.
TRIQUETROHAMATE ARTHRODESIS
Arthrodesis of the triquetrohamate joint is a related procedure indicated primarily for specific patterns of midcarpal instability (MCI) or localized degenerative joint disease affecting the ulnar column of the midcarpal joint.
Surgical Technique
- Approach: The triquetrohamate joint can be accessed through the exact same dorsal transverse or curved longitudinal incision used for the lunotriquetral arthrodesis described earlier.
- Exposure: Following the reflection of the extensor retinaculum and the dorsal capsulotomy, the dissection is carried slightly more distally to expose the articulation between the distal triquetrum and the proximal hamate.
- Preparation: Decortication of the articular surfaces is performed using curets and rongeurs, ensuring removal of all hyaline cartilage down to bleeding subchondral bone.
- Grafting and Fixation: Cancellous bone grafting (harvested from the distal radius) is packed into the defect. The joint is reduced and stabilized using multiple K-wires in a divergent pattern, ensuring no wires violate the surrounding functional articulations (e.g., the capitohamate or lunotriquetral joints, unless a combined fusion is planned).
- Postoperative Care: The immobilization protocol and postoperative care are identical to those used for lunotriquetral and other limited intercarpal arthrodeses.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The postoperative protocol for lunotriquetral (and triquetrohamate) arthrodesis requires strict adherence to prolonged immobilization to combat the high inherent risk of nonunion.
Phase I: 0 to 2 Weeks
- The patient remains in the initial postoperative long-arm thumb spica cast.
- Elevation and active digital range of motion (ROM) exercises for the fingers are encouraged immediately to prevent tendon adhesions and reduce edema.
- At 2 weeks, the cast and skin sutures are removed.
Phase II: 2 to 6 Weeks
- A new, well-molded long-arm thumb spica cast is applied.
- Rationale for Long-Arm Casting: The long-arm cast is critical during this phase to control forearm pronation and supination. Forearm rotation generates significant torque across the proximal carpal row; neutralizing this force protects the delicate K-wire fixation and the maturing bone graft.
- This cast is worn continuously for 4 weeks (until 6 weeks postoperatively).
Phase III: 6 Weeks to Radiographic Union
- At 6 weeks postoperatively, the long-arm cast is removed.
- Clinical evaluation and interval radiographs are obtained to assess early callus formation and hardware integrity.
- A short-arm thumb spica cast is applied. This allows for the initiation of elbow and forearm ROM while continuing to protect the carpus.
- This short-arm cast is worn until there is definitive radiographic evidence of solid bone union across the arthrodesis site. This typically requires an additional 4 to 6 weeks (totaling 10 to 12 weeks of cast immobilization).
Phase IV: Hardware Removal and Rehabilitation
- Once radiographic union is confirmed (usually around 10 to 12 weeks), the cast is discontinued.
- A removable, custom-molded plastic thumb spica splint or wrist orthosis is applied for protection during high-risk activities.
- Gentle, active and active-assisted wrist motion exercises are begun under the guidance of a certified hand therapist.
- Progressive strengthening exercises are initiated only after functional ROM is restored and the patient is pain-free.
- Hardware Removal: The buried Kirschner wires are typically removed in the operating room or minor procedure room under local anesthesia at approximately 3 months postoperatively, provided that solid osseous union is unequivocally confirmed on imaging.
COMPLICATIONS AND MANAGEMENT
- Nonunion: The most significant complication. If asymptomatic, it may be observed. If symptomatic, revision surgery with structural bone grafting (e.g., iliac crest) and rigid internal fixation (using headless compression screws or specialized intercarpal plates) is required.
- Hardware Migration or Breakage: K-wires can migrate dorsally, causing skin irritation or tendon rupture. Wires must be cut short and buried deep to the extensor retinaculum.
- Wrist Stiffness: Prolonged immobilization inevitably leads to capsular contracture. Aggressive postoperative hand therapy is mandatory once union is achieved.
-
Ulnar Impaction: Altered carpal height post-fusion may unmask or exacerbate ulnar positive variance. Concomitant or staged ulnar shortening osteotomy may be necessary if ulnar-sided pain persists despite a solid LT fusion.
You Might Also Like