Ludloff Osteotomy Masterclass: Precision Correction for Hallux Valgus
Key Takeaway
This masterclass guides fellows through the modified Ludloff osteotomy for symptomatic hallux valgus. We'll meticulously cover comprehensive anatomy, precise preoperative planning, and detailed intraoperative execution, from lateral soft tissue release to fixation and capsular repair. Emphasis is placed on neurovascular protection, accurate osteotomy, and stable internal fixation. Postoperative rehabilitation and complication management are also thoroughly discussed, ensuring optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we are undertaking a masterclass in the surgical management of a common, yet biomechanically complex and frequently unforgiving deformity: symptomatic hallux valgus. Specifically, we will be dissecting the nuances of the modified Ludloff osteotomy. This is a highly powerful, diaphyseal technique designed for the precision correction of a first intermetatarsal angle (IMA) greater than 15 degrees, particularly in scenarios where conservative, nonoperative modalities have been exhausted. Originally described by Professor Karl Ludloff in 1918, the procedure initially fell out of favor due to the inherent instability of the unfixated osteotomy. However, it was brilliantly revitalized and modified by Dr. Mark Myerson and colleagues in the late 20th century with the addition of rigid internal fixation, transforming it into a workhorse procedure that offers robust correction, exceptional stability, and predictable osseous union.
The debate surrounding the exact cause-and-effect relationship between hallux valgus and metatarsus primus varus remains a subject of intense academic scrutiny. However, our primary objective in the surgical arena is the definitive, three-dimensional correction of the symptomatic deformity. Hallux valgus is not merely a cosmetic deviation or a simple two-dimensional angular deformity; it is a complex, triplanar derangement involving transverse plane deviation, sagittal plane elevation, and coronal plane pronation of the first ray. Correcting this requires more than just straightening a toe; it demands the restoration of the native biomechanical axis, the alleviation of pain, the normalization of forefoot weight-bearing mechanics, and the prevention of future catastrophic complications such as transfer metatarsalgia or progressive degenerative joint disease.
To master the Ludloff osteotomy, one must look beyond the simple geometry of the bone cut. The surgeon must possess an intimate understanding of the pathogenesis of the deformity, which is driven by an interplay of intrinsic and extrinsic factors. Extrinsic factors, most notably constricting footwear with a narrow toe box, play a significant role, as hallux valgus is almost exclusively documented in shoe-wearing populations. However, the presence of the deformity in patients who have never worn constricting footwear points to powerful intrinsic predispositions. These include a strong genetic penetrance, biomechanical abnormalities such as pes planovalgus (which imposes a longitudinal rotation on the first ray), and hypermobility of the first tarsometatarsal (TMT) joint. When the foot pronates, the first metatarsophalangeal (MTP) joint axis is forced into an oblique plane, drastically reducing the structural capacity of the medial column to resist the deforming forces of weight-bearing.
As we proceed through this masterclass, I implore you to pay meticulous attention to the details. We will delve deeply into the nuances of surgical anatomy, the critical steps of preoperative templating, the uncompromising execution of the osteotomy, and the rigid principles of internal fixation. The difference between an excellent outcome and a surgical failure in hallux valgus surgery frequently hinges on millimeters of translation and degrees of rotation. By mastering the modified Ludloff osteotomy, you equip yourself with a versatile and powerful tool capable of addressing some of the most challenging forefoot deformities encountered in orthopedic practice.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, an exhaustive, three-dimensional understanding of the anatomy and biomechanics of the first ray is absolutely paramount. This is not merely foundational textbook knowledge; it is the dynamic blueprint that dictates every single maneuver we execute in the operating room. The first ray is a complex, load-bearing structure that must simultaneously provide flexible shock absorption during heel strike and rigid propulsion during toe-off.
Osteology and Articular Configuration
The first metatarsophalangeal (MTP) joint is anatomically distinct from the lesser MTP joints, primarily due to the presence of the sesamoid mechanism. These two sesamoid bones—the medial (tibial) and lateral (fibular) sesamoids—are embedded within the tendinous slips of the flexor hallucis brevis (FHB). They articulate directly with two longitudinal, cartilage-covered grooves located on the plantar aspect of the first metatarsal head. These grooves are separated by a prominent central ridge of bone known as the crista. The sesamoids serve a critical biomechanical function: they increase the moment arm and mechanical advantage of the FHB, protect the flexor hallucis longus (FHL) tendon which glides between them, and bear a massive percentage of the body's weight during the propulsive phase of gait. Distally, the sesamoid apparatus is firmly anchored to the plantar base of the proximal phalanx via the thick, fibrous plantar plate.
The articular head of the first metatarsal is rounded, expansive, and covered in hyaline cartilage, articulating with the comparatively smaller, concave, elliptical base of the proximal phalanx. The inherent stability of this joint is not primarily bony, but rather relies heavily on the surrounding soft tissue envelope. Fan-shaped collateral and suspensory ligamentous bands originate from the medial and lateral epicondyles of the metatarsal head. These ligaments fan out to insert onto the base of the proximal phalanx, the medial and lateral margins of the sesamoids, and the robust plantar plate, creating a dynamic hammock that suspends the metatarsal head.
Soft Tissue Envelopes and Musculotendinous Intervals
The dynamic stability and movement of the great toe are governed by four critical groups of muscles and tendons, whose vectors are drastically altered in the presence of hallux valgus. The long and short extensor tendons (extensor hallucis longus and extensor hallucis brevis) run dorsally. In a severe valgus deformity, the EHL tendon subluxates laterally, transitioning from an extensor to a powerful deforming force that exacerbates the valgus drift (the "bowstringing" effect). Plantarly, the long and short flexor tendons (FHL and FHB) operate. The FHB, encasing the sesamoids, is crucial for plantarflexion power.
The intrinsic muscles are the primary drivers of the transverse plane deformity. The abductor hallucis originates from the medial calcaneal tubercle and inserts into the medial sesamoid and the medial base of the proximal phalanx. In hallux valgus, as the metatarsal head drifts medially, the abductor hallucis slides plantarly, losing its ability to abduct the toe and instead contributing to pronation of the hallux. Conversely, the adductor hallucis, composed of oblique and transverse heads, inserts into the lateral sesamoid and the lateral base of the proximal phalanx. Its contracture is the primary deforming force in hallux valgus, relentlessly pulling the proximal phalanx laterally and contributing to the lateral subluxation of the sesamoid apparatus. Releasing this contracted adductor tendon is a non-negotiable, critical component of our surgical reconstruction.
Neurovascular Architecture
The vascular supply to the first metatarsal head is precarious and represents a critical surgical consideration. Aggressive soft tissue stripping or thermal necrosis from the oscillating saw can easily compromise this supply, leading to devastating avascular necrosis (AVN) of the metatarsal head. The primary arterial inflow is derived from the first dorsal metatarsal artery, which courses dorsally within the first intermetatarsal space, sending multiple nutrient branches directly into the lateral and dorsal aspects of the metatarsal head. Additional supply arises from the first plantar metatarsal artery, feeding the plantar capsule and metatarsal head. Meticulous, extra-periosteal dissection and the avoidance of aggressive lateral capsular stripping are vital to preserving these delicate vascular networks.
Neurologically, the surgical approaches place several sensory branches at high risk. On the medial aspect, the dorsomedial cutaneous nerve of the hallux (a terminal branch of the superficial fibular nerve) is highly vulnerable during the medial incision and the subsequent capsulotomy. It typically courses subcutaneously directly over the medial eminence of the first MTP joint. Iatrogenic transection or entrapment in scar tissue can lead to debilitating, painful neuromas or chronic paresthesias. Laterally, the common digital nerve to the first web space (a branch of the medial plantar nerve) and the lateral plantar digital nerve to the hallux are at significant risk during the lateral soft tissue release, particularly when utilizing a dorsal first web space incision to dissect the adductor hallucis tendon.
Exhaustive Indications and Contraindications
The decision to proceed with a Ludloff osteotomy must be predicated on a rigorous evaluation of the patient's clinical presentation, radiographic parameters, and functional demands. The Ludloff is a powerful diaphyseal osteotomy, offering greater corrective potential than distal osteotomies (like the Chevron) but requiring meticulous technique to avoid destabilizing the first ray. It is specifically designed to address the intermetatarsal angle by translating and rotating the distal fragment relative to the proximal shaft.
The primary indication for the Ludloff osteotomy is a symptomatic, moderate-to-severe hallux valgus deformity characterized by an intermetatarsal angle (IMA) generally between 15 and 20 degrees, and a hallux valgus angle (HVA) exceeding 30 degrees. It is particularly useful in patients who have failed exhaustive conservative management, including shoe wear modification, orthotics, and anti-inflammatory therapies. Furthermore, the Ludloff is indicated when the first metatarsocuneiform (TMT) joint is clinically and radiographically stable. If gross hypermobility or degenerative arthrosis is present at the first TMT joint, a Lapidus procedure (first TMT arthrodesis) is the more biomechanically appropriate intervention.
Contraindications must be strictly respected to prevent catastrophic surgical failures. The most critical absolute contraindication is the presence of severe osteoarthritic changes within the first MTP joint (hallux rigidus). Attempting a joint-sparing osteotomy in the setting of advanced cartilage loss will inevitably lead to persistent pain and stiffness, necessitating a subsequent salvage arthrodesis. Additionally, a narrow first metatarsal diaphyseal shaft is a relative contraindication; the Ludloff relies on a long, oblique cut through the diaphysis, and a narrow shaft may not provide adequate surface area for bone-to-bone contact after rotation, predisposing the construct to nonunion or hardware failure.
| Category | Specific Clinical / Radiographic Criteria | Rationale / Surgical Implication |
|---|---|---|
| Primary Indications | IMA > 15 degrees, HVA > 30 degrees. | Diaphyseal osteotomy provides the necessary lever arm for large angular corrections. |
| Primary Indications | Symptomatic medial eminence pain failing conservative care. | Defines the necessity for surgical intervention over continued observation. |
| Primary Indications | Stable first TMT joint (no hypermobility). | Ensures the proximal foundation of the first ray can support the corrected distal segment. |
| Relative Contraindications | Narrow metatarsal diaphyseal width. | Insufficient bone stock for stable rotation and lag screw fixation; high risk of stress riser. |
| Relative Contraindications | Severe osteoporosis / osteopenia. | Poor screw purchase may lead to loss of fixation, dorsal elevation, and malunion. |
| Absolute Contraindications | Advanced osteoarthritis of the 1st MTP joint. | Joint-sparing procedures will fail; requires primary MTP arthrodesis. |
| Absolute Contraindications | Open physes (Skeletally immature patient). | Diaphyseal cuts risk growth plate injury or unpredictable continued growth. |
| Absolute Contraindications | Active local or systemic infection. | High risk of deep osseous infection and hardware colonization. |
Pre-Operative Planning, Templating, and Patient Positioning
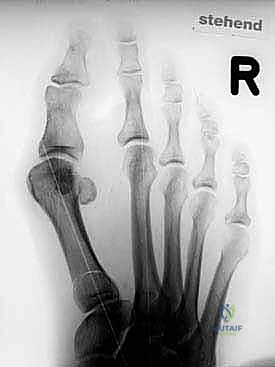
Preoperative planning for the Ludloff osteotomy is not a mere formality; it is the definitive blueprint for surgical success. The complexity of the triplanar correction demands that the surgeon enter the operating room with a precise, mathematically calculated plan. This begins with the acquisition of high-quality, standardized, weight-bearing radiographs of the foot, including anteroposterior (AP), lateral, and oblique projections. Non-weight-bearing films are entirely inadequate, as they fail to demonstrate the true dynamic splaying of the forefoot under physiologic load.
Radiographic Evaluation and Templating
On the weight-bearing AP radiograph, we meticulously measure the Hallux Valgus Angle (HVA), the Intermetatarsal Angle (IMA), and the Distal Metatarsal Articular Angle (DMAA). The DMAA is critical; if it is significantly elevated (indicating a congruent joint with lateral articular deviation), a Ludloff alone may result in a hallux that is straight relative to the metatarsal but subluxated at the joint. In such cases, an adjunctive distal Akin osteotomy of the proximal phalanx or a biplanar modification of the Ludloff may be required. We also assess the sesamoid station—typically graded from 1 to 7—to quantify the degree of lateral subluxation of the sesamoid apparatus relative to the crista.
Digital or acetate templating is mandatory. We draw the planned osteotomy line on the AP radiograph, originating dorsally and proximally (approximately 2-3 mm distal to the first TMT joint) and extending plantarly and distally to exit proximal to the sesamoid complex. By simulating the rotation of the plantar-distal fragment around the proximal axis, we can accurately predict the degree of correction, estimate the required length of the cannulated screws (typically 3.0 mm or 4.0 mm), and confirm that adequate cortical overlap will remain to ensure robust healing.
Operating Room Setup and Patient Positioning
The patient is positioned supine on the operating table. It is imperative that the patient is moved to the absolute distal edge of the bed. This positioning strategy allows the surgical team unimpeded, 360-degree access to the operative foot and facilitates seamless integration of the fluoroscopic C-arm. A small bump (often a rolled towel or a dedicated foam wedge) is placed underneath the ipsilateral greater trochanter. This internally rotates the lower extremity slightly, counteracting the natural external rotation of the relaxed leg and ensuring that the foot rests perfectly perpendicular to the floor. This neutral alignment is critical for obtaining true AP fluoroscopic images intraoperatively.
A pneumatic ankle tourniquet is highly recommended and routinely utilized. A bloodless surgical field is not merely a convenience; it is an absolute necessity for the meticulous identification of the delicate neurovascular structures, particularly the dorsomedial cutaneous nerve and the first web space arborizations. Following exsanguination with an Esmarch bandage, the tourniquet is inflated to standard pressures (typically 250 mmHg). The C-arm is positioned on the contralateral side of the table, draped sterilely, and brought in perpendicular to the foot. We confirm that we can easily obtain both AP and lateral projections without requiring the surgical assistant to awkwardly manipulate the limb.
Step-by-Step Surgical Approach and Fixation Technique
We are now scrubbed, draped, and ready to proceed. The execution of the Ludloff osteotomy requires patience, respect for the soft tissues, and absolute precision with the oscillating saw.
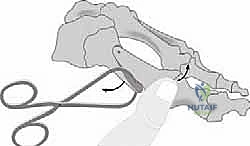
Lateral Soft Tissue Release
The procedure invariably begins with the lateral soft tissue release. This step is fundamental; attempting to correct the bony architecture without first neutralizing the primary deforming soft tissue forces (the contracted adductor hallucis and lateral capsule) will inevitably lead to under-correction or rapid recurrence.
Using a #15 blade, a 3-centimeter dorsal longitudinal incision is made over the first web space, meticulously centered over the interval between the first and second metatarsal heads.

Deep dissection is carried out bluntly using a combination of small tenotomy scissors and a blunt Freer elevator. The surgeon must remain acutely aware of the neurovascular bundle in the first web space. The common digital nerve branch and its plantar bifurcations are highly vulnerable here. The dissection must remain dorsal to the transverse metatarsal ligament and hug the lateral aspect of the first metatarsal head.

Once the interval is developed, a self-retaining Weitlaner or a small lamina spreader is gently inserted between the first and second metatarsal necks to distract the space, while a Langenbeck retractor is used to retract the dorsal soft tissues. This provides the necessary visualization of the lateral MTP joint capsule and the adductor hallucis insertion.

The lateral joint capsule is identified. Using a #15 blade, the lateral capsule is fenestrated, and the metatarsal-sesamoid suspensory ligament is carefully divided immediately superior to the lateral sesamoid. This release is critical for allowing the sesamoid apparatus to mobilize medially back beneath the metatarsal head.

Following the capsulotomy, the conjoined tendon of the adductor hallucis (comprising both the oblique and transverse heads) is identified at its insertion onto the lateral base of the proximal phalanx and the lateral sesamoid. This tendon is sharply detached from its insertion. A successful lateral release is confirmed clinically; the surgeon should be able to effortlessly correct the hallux into a neutral or slightly varus position without encountering soft tissue resistance.
Medial Approach and Exostectomy
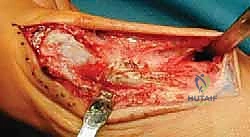
Attention is then directed to the medial aspect of the first ray. A longitudinal incision is made centered over the medial eminence, extending from the mid-diaphysis of the first metatarsal to the mid-diaphysis of the proximal phalanx.

Careful subcutaneous dissection is performed to identify and protect the dorsomedial cutaneous nerve of the hallux. The nerve is gently mobilized and retracted dorsally with the skin flap. A longitudinal or inverted-L capsulotomy is then performed to expose the medial eminence (the "bunion" deformity) and the metatarsal shaft.

Using a sagittal saw, the medial eminence is resected. The cut is made parallel to the medial border of the foot, taking care not to resect into the sagittal sulcus, which would compromise the articulation of the medial sesamoid and risk iatrogenic hallux varus.

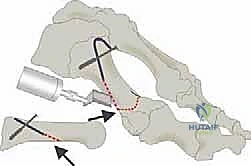
The Ludloff Osteotomy Execution
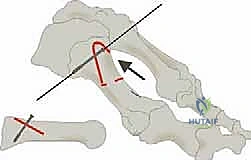
We now arrive at the critical phase: the osteotomy itself. The classic Ludloff cut is an oblique diaphyseal osteotomy. The orientation of this cut is paramount. It must originate dorsally and proximally, approximately 2 to 3 millimeters distal to the first TMT joint articulation. It then courses plantarly and distally, aiming to exit the plantar cortex just proximal to the sesamoid apparatus.


The angle of the saw blade in the sagittal plane is the most critical technical nuance of the procedure. The blade must be angled approximately 10 to 15 degrees plantarward relative to the longitudinal axis of the metatarsal shaft. If the cut is made perfectly parallel to the plantar weight-bearing surface, rotation of the distal fragment will inevitably result in dorsal elevation of the metatarsal head. This dorsal malunion is the primary cause of postoperative transfer metatarsalgia. By angling the cut plantarward, the rotation of the distal fragment inherently plantarflexes the metatarsal head, compensating for the shortening of the first ray and maintaining appropriate load-sharing across the forefoot.

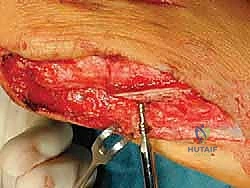
The cut is initiated with a sharp sagittal saw blade. Copious cold saline irrigation is used continuously to prevent thermal necrosis of the bone, which could jeopardize healing. The surgeon must maintain a steady hand, ensuring a single, perfectly planar cut to maximize bone-to-bone contact.

Deformity Correction and Internal Fixation
Once the osteotomy is complete, the distal fragment is highly mobile. The correction is achieved by rotating the plantar-distal fragment laterally (towards the second metatarsal) using the proximal dorsal cortex as a hinge point. This rotation simultaneously reduces the intermetatarsal angle and realigns the metatarsal head over the sesamoid apparatus.

While holding the correction manually, a stout 0.062-inch Kirschner wire is driven from dorsal-proximal to plantar-distal across the osteotomy site to achieve temporary provisional fixation. Fluoroscopy is immediately utilized to confirm the reduction of the IMA, the restoration of the sesamoid station, and the maintenance of a congruent MTP joint.


Rigid internal fixation is achieved using two cannulated lag screws (typically 3.0 mm or 4.0 mm, depending on the patient's bone stock). The first screw is placed perpendicular to the osteotomy cut to maximize interfragmentary compression. A guidewire is placed, depth is measured, and the near cortex is over-drilled to create a gliding hole, ensuring true lag technique.

The first screw is inserted and tightened, compressing the osteotomy.

A second screw is then placed, usually slightly proximal or distal to the first, to provide rotational stability and neutralize sheer forces across the diaphyseal cut.


Following rigid fixation, any overhanging medial bone ledge on the proximal fragment is carefully resected flush with the metatarsal shaft using the sagittal saw. This prevents a prominent medial ridge that could cause hardware irritation or shoe wear issues.

The medial capsule is then meticulously plicated and closed with strong absorbable sutures (e.g., 2-0 Vicryl) while holding the hallux in a neutral position. This medial reefing reinforces the correction. The skin is closed in a standard layered fashion, and a robust, compressive forefoot dressing is applied to maintain alignment and control postoperative edema.


Complications,
