Ilioinguinal Approach: Master the Deep Inguinal Ring for Success

Key Takeaway
This topic focuses on Ilioinguinal Approach: Master the Deep Inguinal Ring for Success, The ilioinguinal approach offers extensive exposure of the inner pelvis, including the anterior and medial surfaces of the acetabulum, ideal for anterior column fractures. This technique involves careful dissection and mobilization of neurovascular structures, alongside the spermatic cord (which traverses the deep inguinal ring) or round ligament. It provides clear visualization from the sacroiliac joint to the pubic symphysis for complex pelvic trauma.
Introduction and Epidemiology
The ilioinguinal approach, pioneered by Emile Letournel and Robert Judet in the 1960s, remains a foundational surgical exposure for the management of complex acetabular and pelvic ring fractures. This extensile anterior approach provides unparalleled visualization of the internal aspect of the hemipelvis, spanning from the sacroiliac joint to the pubic symphysis. It is specifically designed to expose the anterior column, the anterior wall, and the medial aspect of the acetabulum (the quadrilateral surface) without violating the hip joint capsule or the abductor musculature.



Acetabular fractures exhibit a bimodal epidemiological distribution. High-energy trauma, such as motor vehicle collisions and falls from height, typically affects younger patients, resulting in complex, multi-fragmentary fracture patterns. Conversely, low-energy falls in the geriatric population increasingly result in anterior column and anterior wall fractures due to osteoporotic bone. The ilioinguinal approach is highly relevant in both demographics, allowing for anatomic reduction and stable internal fixation, which are critical for preserving native hip joint congruency and preventing post-traumatic osteoarthritis.


Mastery of this approach requires a profound understanding of intrapelvic and inguinal anatomy. The dissection is complex, involving the mobilization of critical neurovascular structures and the meticulous reconstruction of the inguinal canal to prevent postoperative herniation. As orthopedic surgeons operate in an anatomic domain typically reserved for general and vascular surgeons, rigorous cadaveric training and interdisciplinary collaboration are strongly advised for those in the early stages of their learning curve.
Surgical Anatomy and Biomechanics
The ilioinguinal approach is defined by its navigation through the complex neurovascular and musculofascial anatomy of the lower abdominal wall and false pelvis. A comprehensive understanding of these structures is mandatory for safe execution.
Osteology and Biomechanics
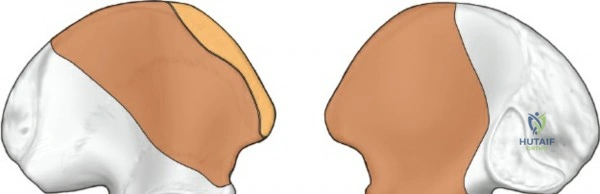
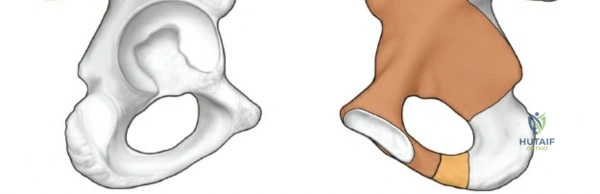
The anterior column of the acetabulum extends from the anterior iliac wing down to the pubic symphysis. It encompasses the anterior half of the iliac wing, the anterior wall of the acetabulum, and the superior pubic ramus. Biomechanically, the anterior column is subjected to significant compressive forces during weight-bearing. The quadrilateral plate, representing the medial wall of the acetabulum, is frequently medially displaced in both-column fractures. The ilioinguinal approach allows direct access to the pelvic brim (iliopectineal line), which serves as the primary corridor for plate fixation to buttress the anterior column and reduce the quadrilateral plate.
Musculofascial Anatomy and the Inguinal Canal
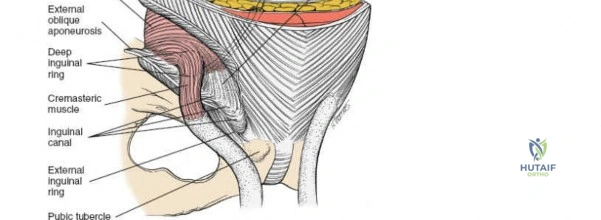
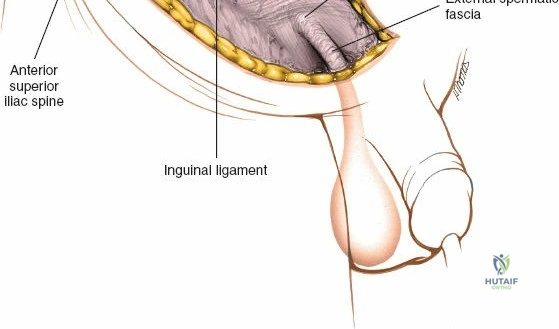
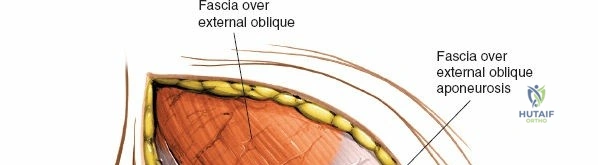
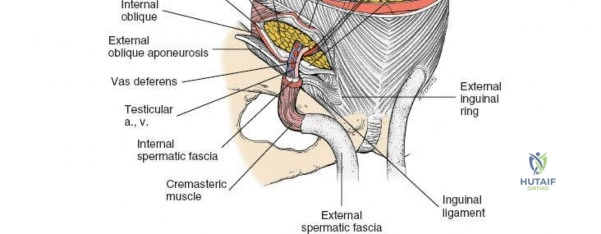
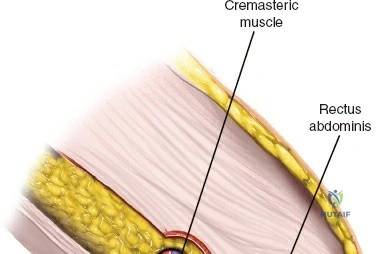
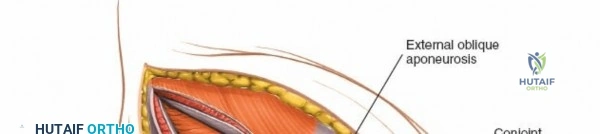
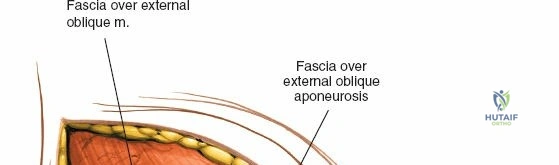
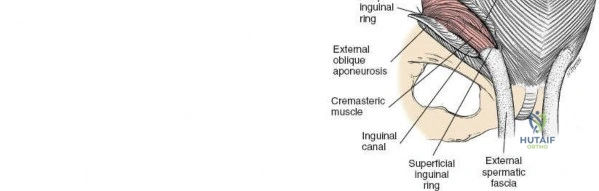
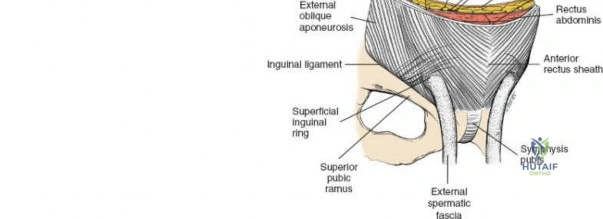
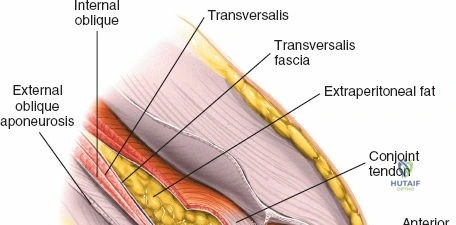
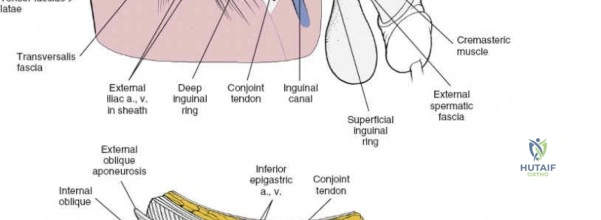
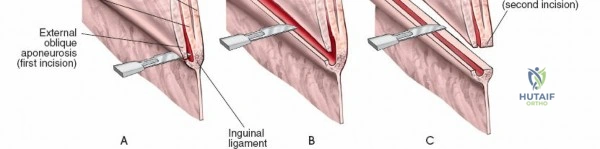
The abdominal wall consists of the external oblique, internal oblique, and transversus abdominis muscles. The aponeurosis of the external oblique forms the anterior wall of the inguinal canal. The inferior margin of this aponeurosis forms the inguinal ligament (Poupart's ligament), stretching from the anterior superior iliac spine (ASIS) to the pubic tubercle.
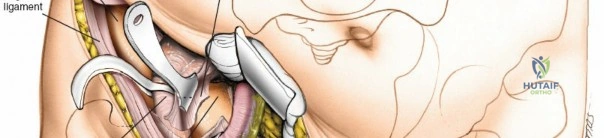
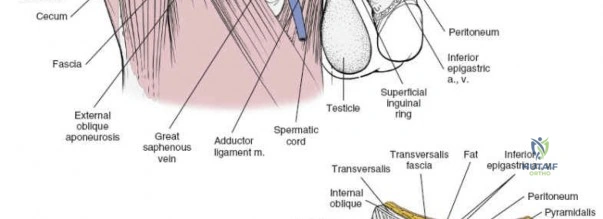
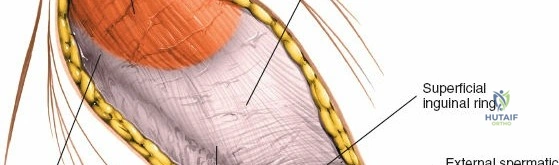
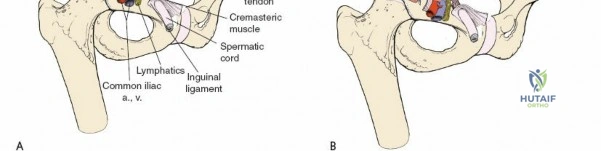
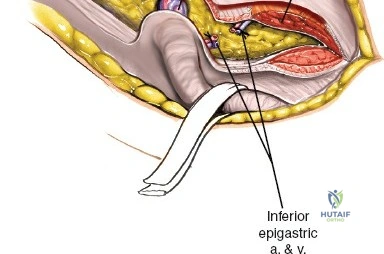
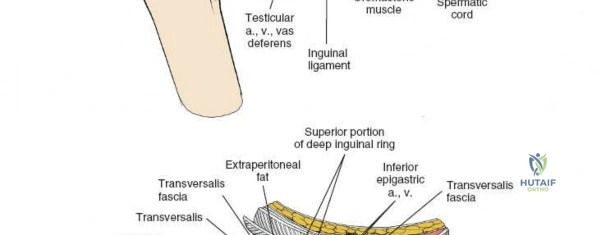
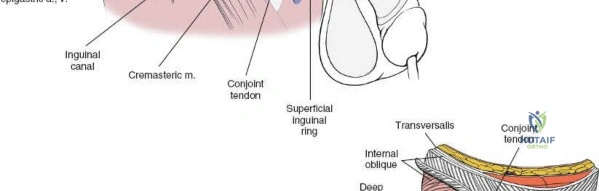
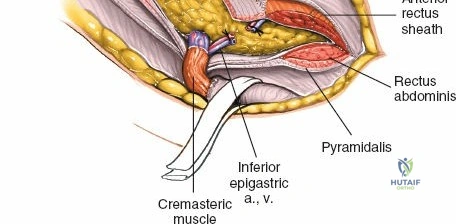
The deep inguinal ring is an opening in the transversalis fascia, located midway between the ASIS and the pubic symphysis, just lateral to the inferior epigastric vessels. The superficial inguinal ring is a triangular defect in the external oblique aponeurosis, superolateral to the pubic tubercle. The contents of the inguinal canal—the spermatic cord in males and the round ligament in females—must be meticulously identified, vessel-looped, and protected.

Neurovascular Anatomy
Several critical neurovascular structures dictate the surgical windows of the ilioinguinal approach:
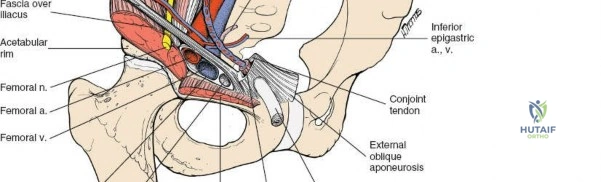
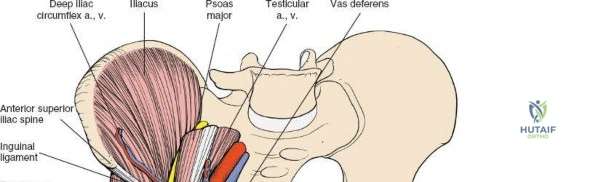
1. Lateral Femoral Cutaneous Nerve (LFCN): Typically exits the pelvis medial to the ASIS, passing under or through the inguinal ligament. It exhibits significant anatomic variance and is highly susceptible to iatrogenic injury during the lateral dissection.
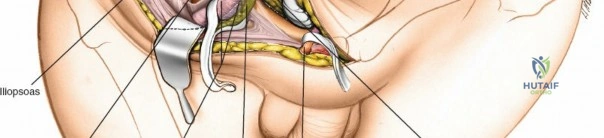
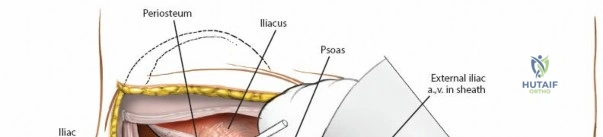
2. Femoral Nerve: Lies deep to the iliacus fascia, within the groove between the psoas major and iliacus muscles. It is protected within the first and second surgical windows by maintaining the integrity of the iliopsoas fascia until intentional release.
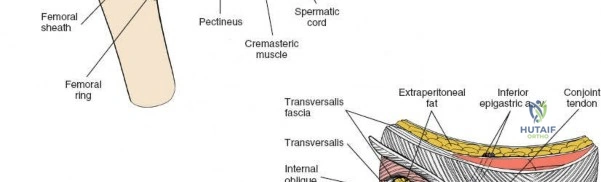
3. External Iliac Vessels: The external iliac artery and vein exit the pelvis under the inguinal ligament to become the femoral vessels. They are encased in a vascular sheath and define the boundary between the second and third surgical windows.
4. Corona Mortis: A critical vascular anastomosis between the obturator and external iliac (or inferior epigastric) systems, located on the posterior aspect of the superior pubic ramus. It is present in up to 80% of hemipelves and must be identified and ligated during the medial dissection to prevent catastrophic hemorrhage.

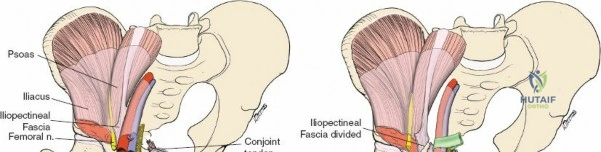
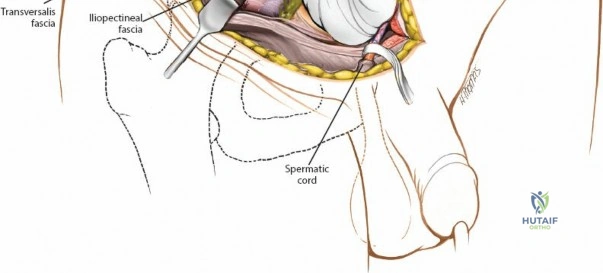
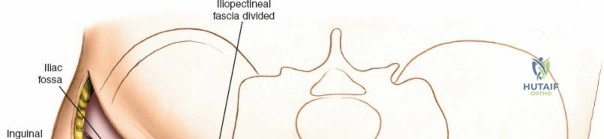
The Iliopectineal Fascia
The iliopectineal fascia is a thick fibrous septum that separates the muscular lacuna (containing the iliopsoas and femoral nerve) laterally from the vascular lacuna (containing the external iliac vessels) medially. Division of this fascia down to the pelvic brim is the absolute crux of the ilioinguinal approach, allowing communication between the surgical windows and providing access to the true pelvis.

Indications and Contraindications
The selection of the ilioinguinal approach relies heavily on the Letournel classification of acetabular fractures. It is the gold standard for fractures with predominant anterior displacement, but it provides no access to the posterior column or posterior wall.
Operative vs Non Operative Management
| Parameter | Operative Indications (Ilioinguinal Approach) | Contraindications / Non-Operative |
|---|---|---|
| Fracture Pattern | Anterior column, Anterior wall, Anterior column + posterior hemitransverse, Associated both-column (if anterior displacement dictates reduction). | Pure posterior wall, pure posterior column, T-type fractures with severe posterior displacement. |
| Displacement | > 2 mm displacement within the weight-bearing dome. | < 2 mm displacement, secondary congruence in both-column fractures. |
| Joint Stability | Hip joint instability, marginal impaction, intra-articular incarcerated fragments. | Stable hip joint, concentric reduction on all radiographic views. |
| Patient Factors | Medically optimized for major pelvic surgery, capable of adhering to postoperative weight-bearing restrictions. | Severe medical comorbidities, active abdominal/pelvic infection, presence of a colostomy/ileostomy in the surgical field. |
| Timing | Acute fractures (< 3 weeks). | Delayed presentations (> 3 weeks) often require extensile approaches (e.g., iliofemoral) due to callus formation. |

Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is critical for minimizing intraoperative complications and achieving an anatomic reduction. Standard radiographic evaluation includes an anteroposterior (AP) view of the pelvis and Judet views (iliac oblique and obturator oblique). High-resolution computed tomography (CT) with 2D multiplanar reformats and 3D surface rendering is mandatory to delineate fracture lines, assess marginal impaction, and identify intra-articular debris.


Patient Positioning
- Table: Place the patient supine on a fully radiolucent operating table, such as a Jackson table with a flat top, to allow for unimpeded intraoperative fluoroscopy in AP, iliac oblique, and obturator oblique planes.
- Positioning: The ipsilateral greater trochanter should be positioned at the edge of the table. This allows the gluteal mass to fall posteriorly, facilitating fracture reduction.
- Preparation: A urinary catheter must be inserted prior to positioning. Decompressing the bladder is critical to prevent iatrogenic injury and to maximize the intrapelvic working space.
- Draping: The abdomen is prepped from the costal margin to the mid-thigh bilaterally. The ipsilateral lower extremity must be draped free to allow for intraoperative manipulation (flexion and adduction relax the iliopsoas and neurovascular bundles).
- Bump: A sterile bump is often placed under the ipsilateral knee to maintain hip flexion, thereby relaxing the iliopsoas muscle and the femoral nerve, which decreases tension during retraction.

Detailed Surgical Approach and Technique
The ilioinguinal approach does not utilize a true internervous plane; rather, it is an anatomical dissection that lifts muscular, nervous, and vascular structures off the inner table of the pelvis.
Incision and Superficial Dissection
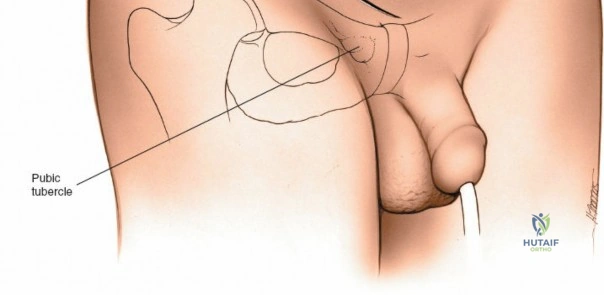
Palpate the ASIS and the pubic tubercle. The incision begins approximately 5 cm proximal and posterior to the ASIS, following the crest anteriorly. At the ASIS, the incision curves medially, running parallel to and approximately 1 to 2 cm proximal to the inguinal crease, ending 2 cm past the midline just superior to the pubic symphysis.


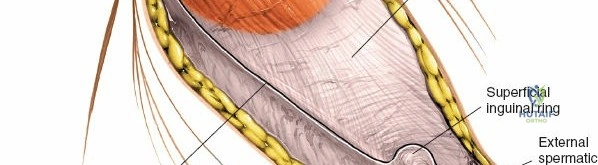
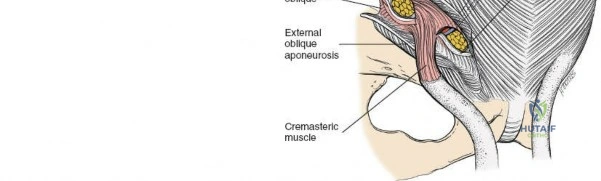
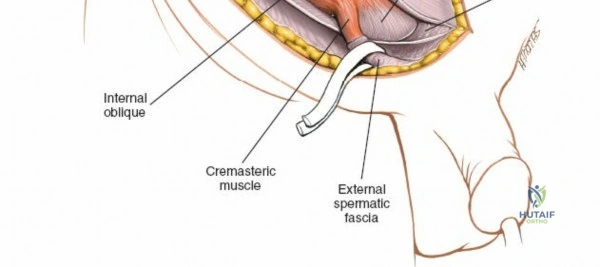
Dissect through the subcutaneous tissues (Camper's and Scarpa's fascia) to expose the external oblique aponeurosis. Identify the superficial inguinal ring medially. Incise the external oblique aponeurosis in line with its fibers, starting from the superficial ring and extending laterally to the ASIS. Carefully protect the ilioinguinal nerve, which typically runs just deep to the aponeurosis.
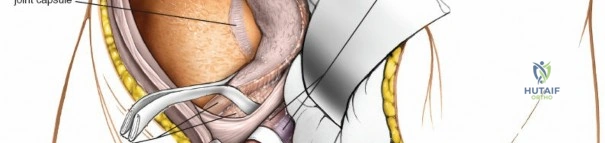
Once the aponeurosis is open, identify the spermatic cord (or round ligament). Mobilize it circumferentially and place it in a Penrose drain.
Deep Dissection: Developing the Three Windows
The essence of the ilioinguinal approach is the development of three distinct surgical windows, separated by critical neurovascular structures.
The First Window (Lateral Window)
This window is developed lateral to the iliopsoas muscle.
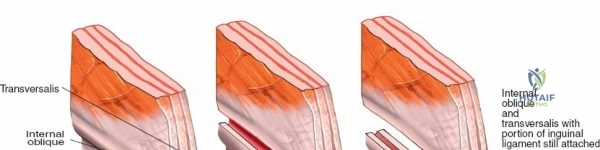
1. Incise the abdominal musculature (external oblique, internal oblique, and transversus abdominis) off the anterior iliac crest.
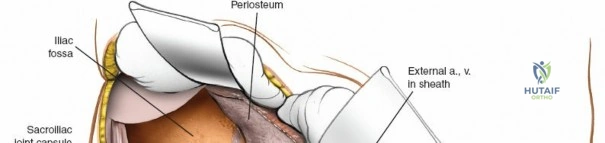
2. Perform a subperiosteal elevation of the iliacus muscle from the internal iliac fossa.
3. Pack the fossa with laparotomy sponges to maintain hemostasis.
4. This window provides exposure of the entire internal iliac fossa down to the sacroiliac joint and the superior aspect of the pelvic brim.

The Second Window (Middle Window)
This window is located between the iliopsoas muscle/femoral nerve laterally and the external iliac vessels medially.
1. Detach the internal oblique and transversus abdominis muscles from the lateral half of the inguinal ligament. Leave a 2 mm cuff of tissue on the ligament to facilitate robust closure and prevent herniation.
2. Identify the iliopectineal fascia, which separates the iliopsoas from the external iliac vessels.
3. Critical Step: Divide the iliopectineal fascia sharply down to the pectineal eminence. This release allows the external iliac vessels to be mobilized medially and the iliopsoas to be mobilized laterally, opening access to the true pelvis.
4. This window provides access to the pelvic brim, the quadrilateral plate, and the anterior wall of the acetabulum.


The Third Window (Medial Window)
This window is located medial to the external iliac vessels and lateral to the rectus abdominis muscle.
1. Carefully mobilize the external iliac artery and vein laterally using a vascular loop.
2. Dissect along the superior pubic ramus towards the pubic symphysis.
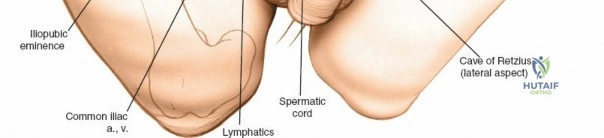
3. Critical Step: Identify and ligate the corona mortis. This anastomotic vessel crosses the superior pubic ramus approximately 3 to 5 cm lateral to the symphysis. Failure to control this vessel can result in retraction into the true pelvis and catastrophic hemorrhage.
4. This window exposes the superior pubic ramus, the Space of Retzius, and the pubic symphysis.


Fracture Reduction and Fixation
Reduction is achieved utilizing a combination of specific pelvic reduction forceps (e.g., Matta clamps, Jungbluth clamps), Schanz pins placed in the iliac wing as joysticks, and specialized ball-spike pushers. The quadrilateral plate can be reduced using a collinear reduction clamp or by applying a buttress plate through the middle window.
Fixation typically consists of 3.5 mm pelvic reconstruction plates contoured to the pelvic brim. These plates span from the intact ilium posteriorly, across the iliopectineal line, to the pubic symphysis anteriorly. Lag screws can be directed down the anterior column or antegrade into the posterior column depending on the fracture morphology.

Closure and Inguinal Canal Reconstruction
Meticulous layered closure is imperative to prevent postoperative abdominal wall herniation.
1. Clean the wound and ensure absolute hemostasis. Remove all laparotomy sponges.
2. Repair the conjoint tendon and the transversalis fascia to the inguinal ligament using heavy, non-absorbable, interrupted sutures.
3. Reattach the internal oblique and transversus abdominis to the iliac crest.
4. Ensure the deep inguinal ring is snug but not constricting the spermatic cord.
5. Close the external oblique aponeurosis over the cord, recreating the superficial inguinal ring.
6. Close the subcutaneous tissues and skin.


Complications and Management
Due to the extensive dissection and proximity to major neurovascular structures, the ilioinguinal approach carries specific risks. Awareness and preemptive management are key to minimizing morbidity.

Common Complications Table
| Complication | Incidence | Etiology / Mechanism | Prevention and Salvage Strategies |
|---|---|---|---|
| LFCN Neuropraxia | 25% - 30% | Traction or direct transection during lateral window exposure. | Careful dissection medial to ASIS. Inform patient preoperatively of numbness over anterolateral thigh. Usually self-limiting if not transected. |
| Femoral Nerve Palsy | 2% - 5% | Excessive retraction in the first/second window, hematoma. | Maintain hip flexion intraoperatively. Limit continuous retraction time. Release iliopectineal fascia fully to reduce tension. |
| Vascular Injury (Corona Mortis) | < 2% (if managed) | Avulsion during medial dissection or fracture displacement. | Identify and ligate routinely before medial exploration. If avulsed, pack immediately and extend exposure for direct repair or embolization. |
| Inguinal Hernia | 1% - 3% | Inadequate repair of the transversalis fascia/conjoint tendon to inguinal ligament. | Meticulous, layered closure with heavy non-absorbable suture. General surgery consultation if tissue quality is poor. |
| DVT / Pulmonary Embolism | 5% - 10% | Pelvic venous stasis, endothelial injury, hypercoagulable state. | Mechanical prophylaxis intraoperatively. Chemical prophylaxis (LMWH) initiated postoperatively once hemostasis is secure. |
| Infection | 2% - 4% | Extensive soft tissue stripping, prolonged operative time. | Preoperative antibiotics, meticulous hemostasis, minimization of dead space, judicious use of closed suction drains. |

Post Operative Rehabilitation Protocols
Postoperative rehabilitation must be tailored to the stability of the fixation and the specific fracture pattern. However, general principles apply to all patients undergoing acetabular reconstruction via the ilioinguinal approach.
- Weight-Bearing: Patients are typically restricted to toe-touch weight-bearing (TTWB) or flat-foot weight-bearing (to eliminate equinus contracture) for 8 to 12 weeks postoperatively. Full weight-bearing is delayed until radiographic evidence of fracture consolidation is present.
- Range of Motion: Early passive and active-assisted range of motion (ROM) of the hip, knee, and ankle is encouraged immediately postoperatively to nourish the articular cartilage and prevent capsular contracture.
Clinical & Radiographic Imaging