Acetabular and Pelvic Fractures: A Comprehensive Surgical Guide

Key Takeaway
Acetabular fractures represent one of the most formidable challenges in orthopaedic trauma. Successful management demands a profound understanding of pelvic osteology, precise radiographic interpretation, and mastery of complex surgical approaches. This guide details the evidence-based protocols for initial resuscitation, anatomical reduction, and rigid internal fixation. By adhering to the principles established by Letournel and Judet, surgeons can optimize articular congruity, minimize neurovascular complications, and significantly improve long-term patient outcomes in high-energy pelvic trauma.
Comprehensive Introduction and Patho-Epidemiology
The operative treatment of acetabular fractures remains one of the most complex, unforgiving, and technically demanding disciplines within the realm of orthopaedic trauma surgery. Historically, these severe articular disruptions were managed nonoperatively with prolonged periods of skeletal traction. This archaic approach frequently yielded abysmal functional outcomes, characterized by early, severe post-traumatic arthrosis, joint contractures, and profound disability. The modern era of acetabular reconstruction was unequivocally pioneered by the visionary work of Emile Letournel and Robert Judet in the mid-20th century. Their rigorous establishment of the two-column anatomical concept, standardized radiographic evaluation through specific oblique projections, and the development of extensile and targeted surgical approaches fundamentally revolutionized the standard of patient care.
However, mastering these intricate techniques involves a notoriously steep and well-documented learning curve. As demonstrated in landmark longitudinal studies by Matta and Merritt, the chronological grouping of a surgeon’s first 100 operatively treated acetabular fractures reveals a direct, undeniable correlation between cumulative surgical experience and the incidence of achieving anatomical reductions. The spatial reasoning required to manipulate complex, multi-planar pelvic geometry through limited surgical windows demands both innate aptitude and rigorous, specialized fellowship training. Similarly, Kebaish, Roy, and Rennie highlighted that experienced pelvic trauma surgeons achieve significantly higher rates of anatomical reduction compared to their less experienced counterparts. Because the quality of articular reduction is the single most critical prognostic factor for long-term native hip survivorship, these procedures should ideally be centralized and performed in Level I trauma centers by surgeons with dedicated pelvic and acetabular training.
Epidemiologically, acetabular fractures present with a distinct bimodal distribution. The first peak occurs in young, predominantly male patients subjected to high-energy blunt trauma mechanisms, such as high-speed motor vehicle collisions, motorcycle accidents, or falls from significant heights. These high-energy vectors often result in massive comminution, marginal impaction of the articular cartilage, and concomitant life-threatening injuries. The second, increasingly prevalent peak involves the geriatric population. With the global demographic shift toward an aging population, low-energy falls from a standing height in patients with underlying osteopenia or frank osteoporosis are resulting in complex fracture patterns. These osteoporotic fractures frequently involve the anterior column and quadrilateral plate, presenting unique biomechanical challenges for stable internal fixation and often necessitating acute total hip arthroplasty (THA) in conjunction with internal fixation.

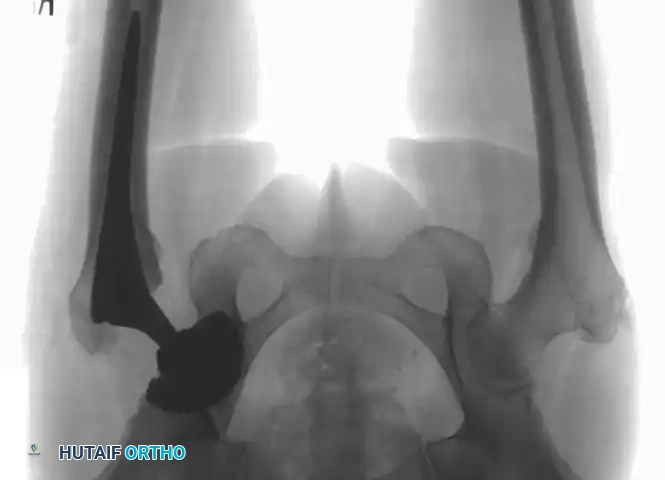
Initial patient management must strictly adhere to Advanced Trauma Life Support (ATLS) protocols. Because these fractures are predominantly the result of high-energy trauma, patients frequently present in extremis with concomitant hemorrhagic shock, traumatic brain injuries, thoracic trauma (e.g., pneumothorax, pulmonary contusion), and visceral abdominal injuries. Orthopaedic intervention, particularly definitive fixation, is secondary to hemodynamic stabilization and the acute management of massive pelvic hemorrhage. Once the patient is resuscitated, early application of skeletal traction via a distal femoral pin is advocated. Distraction of the femoral head away from the abrasive edges of the fractured acetabular cartilage minimizes ongoing chondral damage. Furthermore, the rapid identification and urgent reduction of irreducible fracture-dislocations—where the femoral head is incarcerated within the true pelvis or blocked by a rotated posterior wall fragment—is a critical orthopaedic emergency to mitigate the exponentially rising risk of femoral head osteonecrosis and irreversible sciatic nerve ischemia.

Detailed Surgical Anatomy and Biomechanics
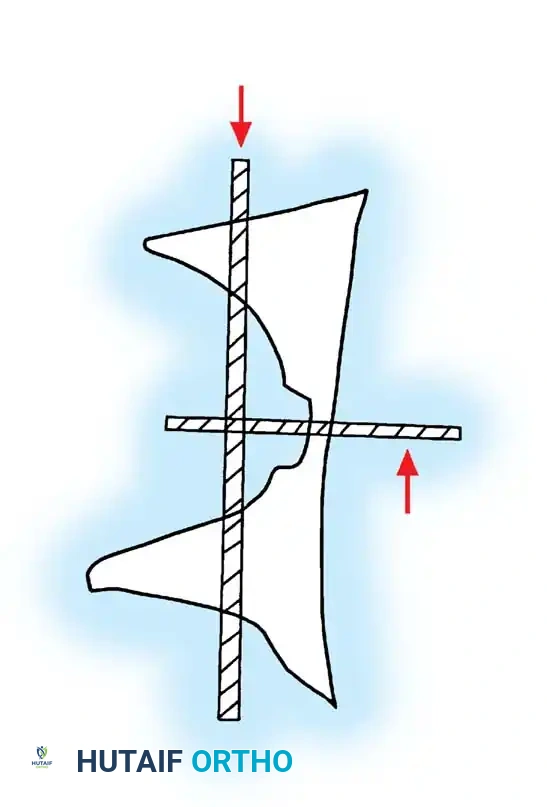
The Letournel Two-Column Concept
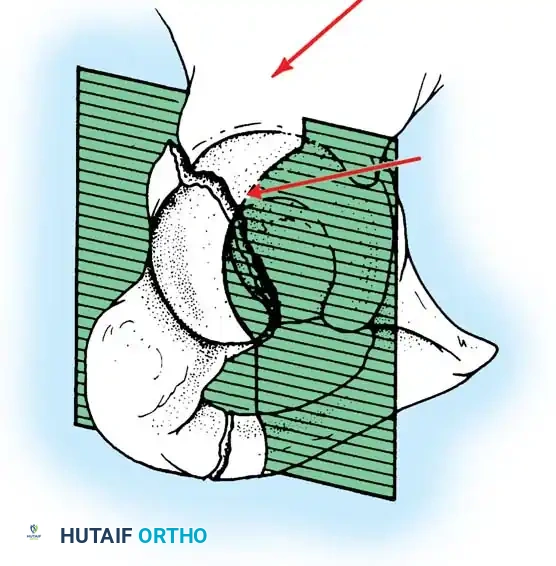
A profound, intuitive, three-dimensional understanding of pelvic osteology is absolutely non-negotiable for the acetabular surgeon. Letournel brilliantly conceptualized the acetabulum as an incomplete hemispherical socket supported by two distinct, structural pillars of bone, resembling an inverted "Y" when viewed from the lateral perspective. This architectural framework dictates both fracture classification and the subsequent selection of surgical approaches. The anterior column extends from the anterior iliac crest down to the pubic symphysis. It is a complex, multi-planar structure comprising the anterior iliac wing, the anterior superior iliac spine (ASIS), the anterior inferior iliac spine (AIIS), the anterior half of the acetabular articular surface, and the superior and inferior pubic rami.
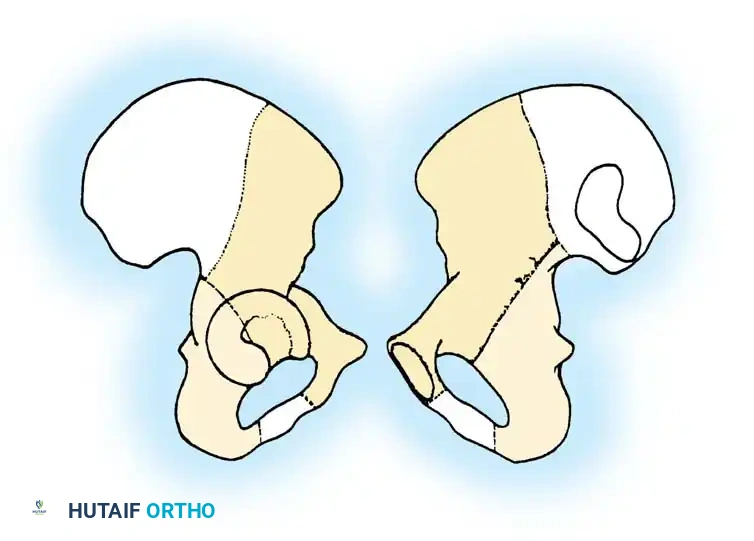
Conversely, the posterior column is a significantly shorter, thicker, and denser pillar of bone. It begins at the dense cortical bone of the greater sciatic notch and extends inferiorly to terminate at the ischial tuberosity. The posterior column encompasses the posterior half of the acetabulum, the ischial spine, and the ischium itself. The intersection of these two columns forms the thickest portion of the innominate bone, located just superior to the acetabulum, known as the sciatic buttress. Understanding the distinct trajectories and cortical densities of these columns is critical for safe and effective screw placement, particularly when utilizing intraosseous column screws that must traverse the narrow medullary corridors without breaching the hip joint or the pelvic basin.
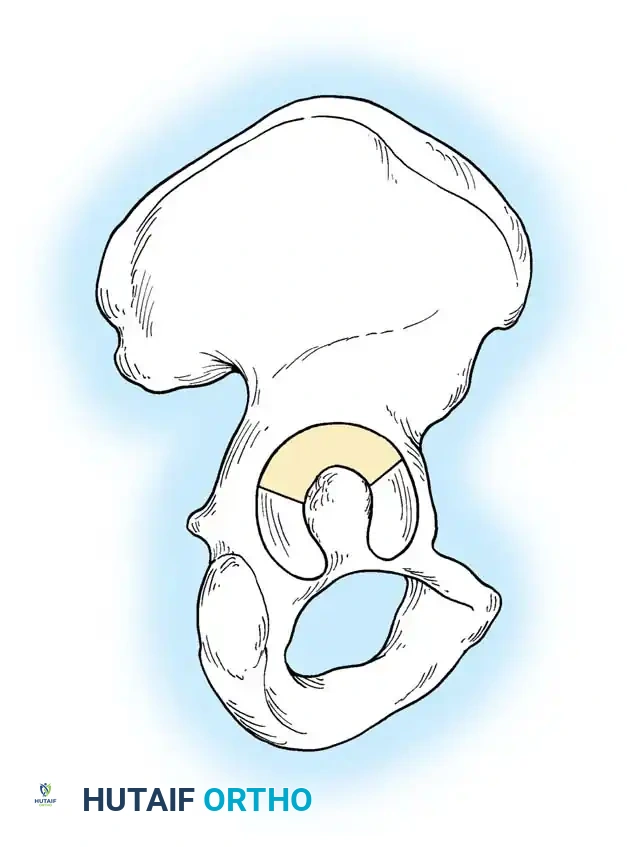
The Weight-Bearing Dome and Quadrilateral Surface
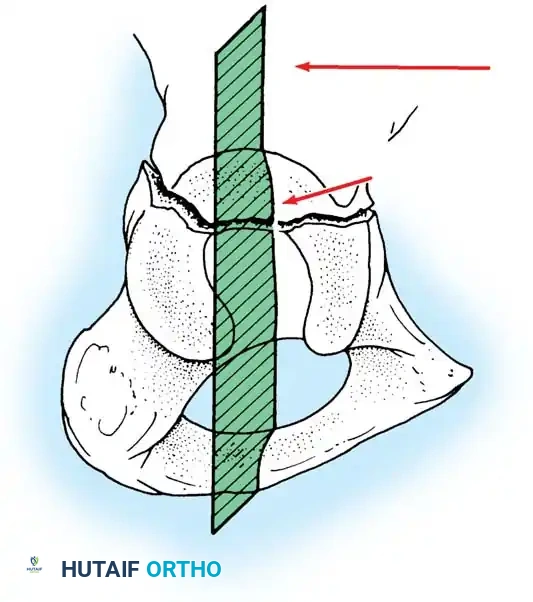
The superior aspect of the acetabulum, commonly referred to as the "dome" or "roof," constitutes the primary weight-bearing articular surface. Anatomical restoration of this specific region is the ultimate, uncompromising goal of surgical intervention, as even minor step-offs or gaps in the dome will lead to rapid, catastrophic joint wear and post-traumatic osteoarthritis. Medial to the acetabular fossa lies the quadrilateral surface (or quadrilateral plate), a remarkably thin, flat plate of bone that forms the lateral wall of the true pelvis. In osteoporotic patients, medial subluxation of the femoral head frequently completely blows out this fragile structure.
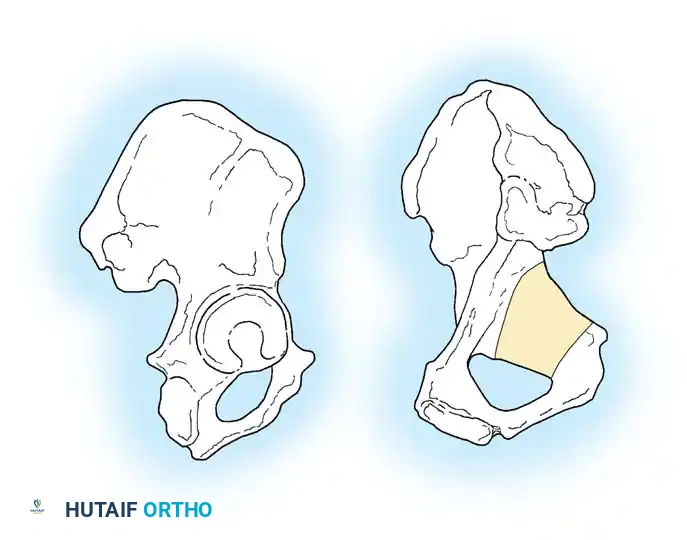
Directly overlying the femoral head anteriorly is the iliopectineal eminence. Because both the quadrilateral surface and the iliopectineal eminence consist of wafer-thin bone, they offer exceptionally poor purchase for standard cortical lag screws. Consequently, surgeons must rely on specialized fixation techniques to buttress these areas. This includes the use of under-contoured spring plates, which utilize the elastic recoil of the metal to provide a dynamic buttress against the quadrilateral plate, or the application of infra-pectineal pelvic brim plating techniques designed to span the comminution and hold the medial wall out to length.
Critical Neurovascular Anatomy
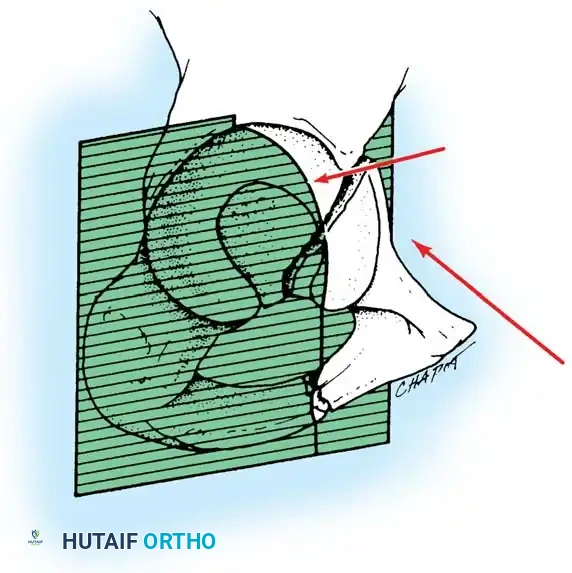
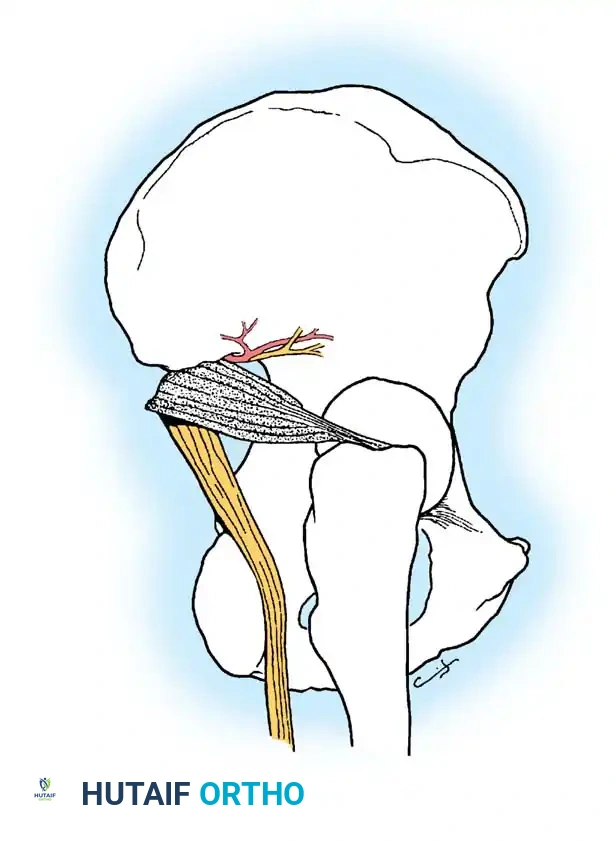
Surgical approaches to the acetabulum are fraught with peril due to the dense network of critical neurovascular structures intimately associated with the pelvis. The sciatic nerve is perhaps the most vulnerable, exiting the pelvis through the greater sciatic notch, typically coursing inferior to the piriformis muscle. It is highly susceptible to traumatic injury during posterior fracture-dislocations (due to direct compression or stretch) and is at significant iatrogenic risk during the Kocher-Langenbeck surgical approach, necessitating continuous, vigilant protection and often the use of intraoperative neuromonitoring (SSEP/MEP).
Furthermore, the superior gluteal artery and nerve exit the greater sciatic notch at its most superior apex. Fractures extending into the apex of the notch can lacerate this high-flow artery, leading to massive, life-threatening retroperitoneal hemorrhage that may require preoperative angiography and embolization. Anteriorly, the Corona Mortis represents a critical, highly variable vascular anastomosis between the external iliac (or inferior epigastric) system and the obturator system, coursing directly over the superior pubic ramus. Tornetta et al. demonstrated that this anastomosis is present in up to 84% of hemipelves. Failure to meticulously identify, isolate, and ligate the Corona Mortis during the ilioinguinal or modified Stoppa approach can result in catastrophic hemorrhage, as the severed vessel frequently retracts deep into the true pelvis, rendering hemostasis exceedingly difficult.

Exhaustive Indications and Contraindications
The decision-making process regarding the operative versus nonoperative management of acetabular fractures is highly nuanced, requiring a synthesis of patient-specific physiological factors, fracture geometry, and joint stability.
Indications for Nonoperative Management
Nonoperative management is strictly reserved for a highly specific and rigorously defined subset of fractures. The criteria, largely established and validated by Joel Matta, are uncompromising. First, there must be minimal displacement, strictly defined as less than 2 mm of displacement within the weight-bearing dome. Second, the weight-bearing dome must remain intact, which is assessed via roof arc angles on CT or plain radiographs; the medial, anterior, and posterior roof arc angles must all exceed 45 degrees. Third, absolute joint congruency is required; the femoral head must remain perfectly concentric with the intact portion of the acetabular roof on all radiographic views, both in and out of traction. Finally, there must be a complete absence of intra-articular fragments (incarcerated bone or cartilage). Nonoperative protocols demand immense patient compliance, typically involving 6 to 8 weeks of strict toe-touch weight-bearing (TTWB), aggressive deep vein thrombosis (DVT) prophylaxis, and serial radiographic monitoring to ensure no secondary displacement occurs during the healing phase.
Indications for Operative Management
Operative intervention is the standard of care for the vast majority of displaced acetabular fractures in physiologically capable patients. Absolute indications include displacement greater than 2 mm in the weight-bearing dome, any degree of incongruency of the hip joint (subluxation), and the presence of incarcerated intra-articular loose bodies that block concentric reduction. Furthermore, posterior wall fractures involving greater than 20% of the articular surface, or those demonstrating dynamic instability on examination under anesthesia (EUA) or fluoroscopic stress views, mandate open reduction and internal fixation (ORIF). Ipsilateral femoral fractures (the "floating hip") also strongly indicate operative fixation of the acetabulum to facilitate early mobilization and optimize the management of the femoral shaft fracture.
Contraindications and Geriatric Considerations
Contraindications to operative intervention include profound systemic instability where the patient cannot tolerate a prolonged, blood-loss-heavy surgical procedure, severe local soft tissue infection or massive degloving injuries (Morel-Lavallée lesions) over the planned surgical incision, and a non-ambulatory baseline status (e.g., severe dementia, paraplegia) where the risks of surgery far outweigh the functional benefits. In the geriatric population, extreme osteoporosis presents a relative contraindication to standard ORIF, as the bone may simply fail to hold hardware. In these complex scenarios, the paradigm has shifted toward acute Total Hip Arthroplasty (THA) combined with limited internal fixation (to stabilize the columns enough to support an acetabular component). This "fix and replace" strategy allows for immediate weight-bearing and avoids the high failure rates associated with ORIF in osteoporotic bone.
| Parameter | Indications for ORIF | Indications for Nonoperative Care | Contraindications to ORIF |
|---|---|---|---|
| Displacement | > 2 mm in weight-bearing dome | < 2 mm in weight-bearing dome | Severe osteopenia precluding fixation |
| Joint Stability | Subluxation / Dynamic instability | Concentric reduction maintained | Non-ambulatory baseline |
| Roof Arc Angles | Any angle < 45 degrees | All angles > 45 degrees | Systemic instability (Damage Control) |
| Intra-articular | Loose bodies present | Clear joint space | Active local infection / Morel-Lavallée |
Pre-Operative Planning, Templating, and Patient Positioning
Standardized Radiographic Evaluation
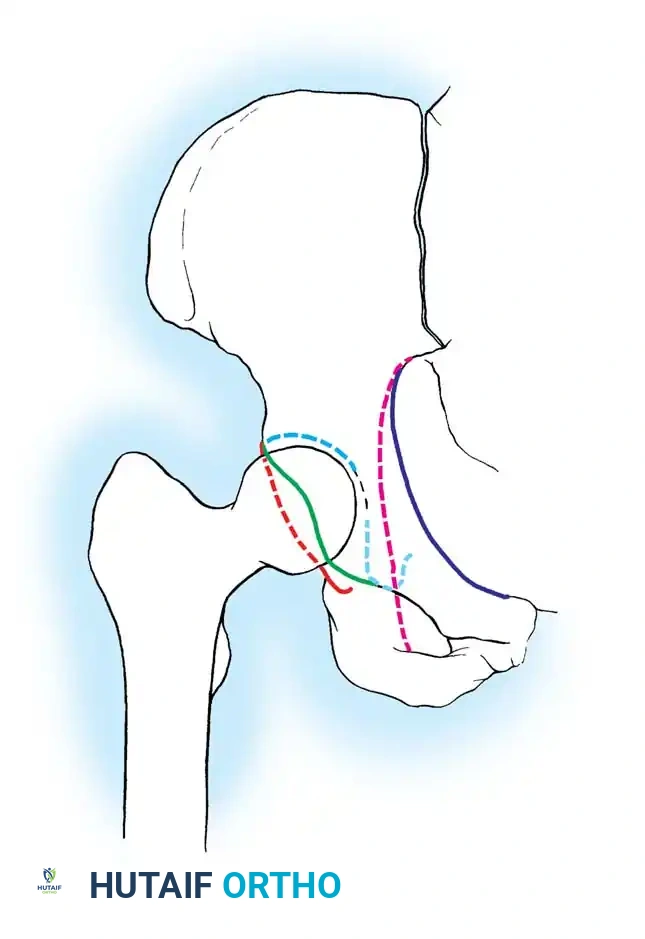
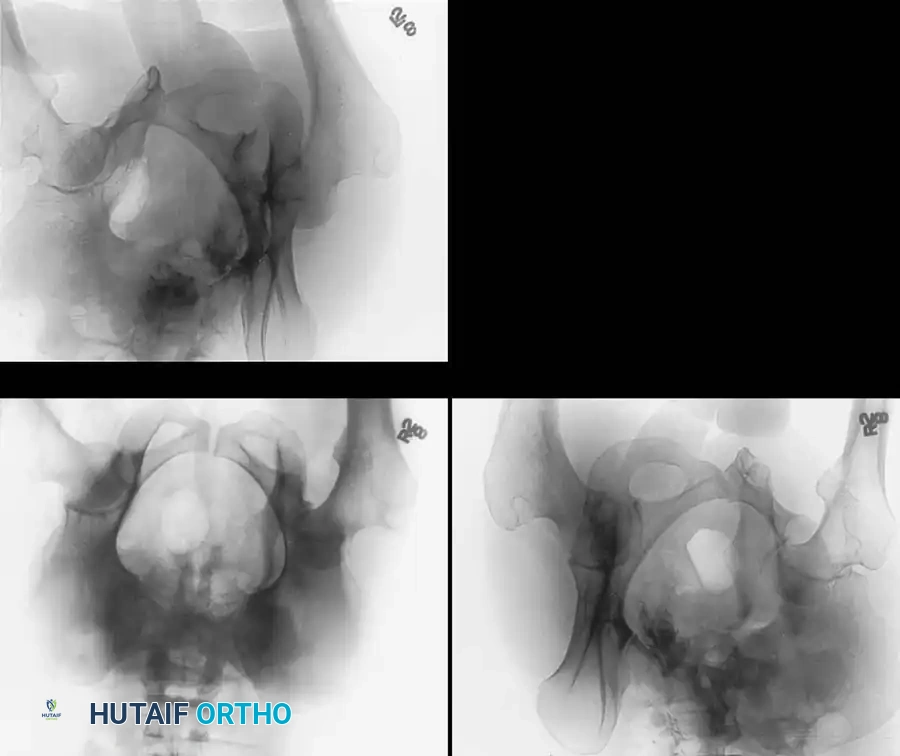
Accurate classification and meticulous surgical planning rely entirely on a standardized radiographic series, fundamentally supplemented by advanced cross-sectional imaging. The initial evaluation begins with a high-quality Anteroposterior (AP) view of the pelvis. The surgeon must systematically assess the six fundamental radiographic landmarks of the acetabulum: the iliopectineal line (representing the anterior column), the ilioischial line (representing the posterior column), the radiographic teardrop (representing the medial wall and inferior aspect of the acetabular fossa), the acetabular roof (the weight-bearing dome), the anterior lip, and the posterior lip of the acetabulum. Disruption of any of these lines provides the first clue to the underlying fracture pattern.
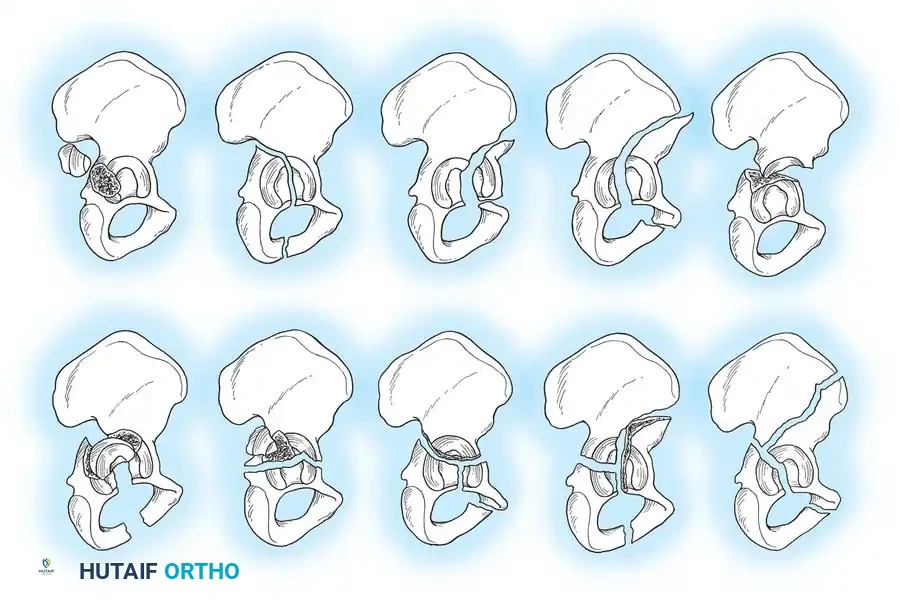
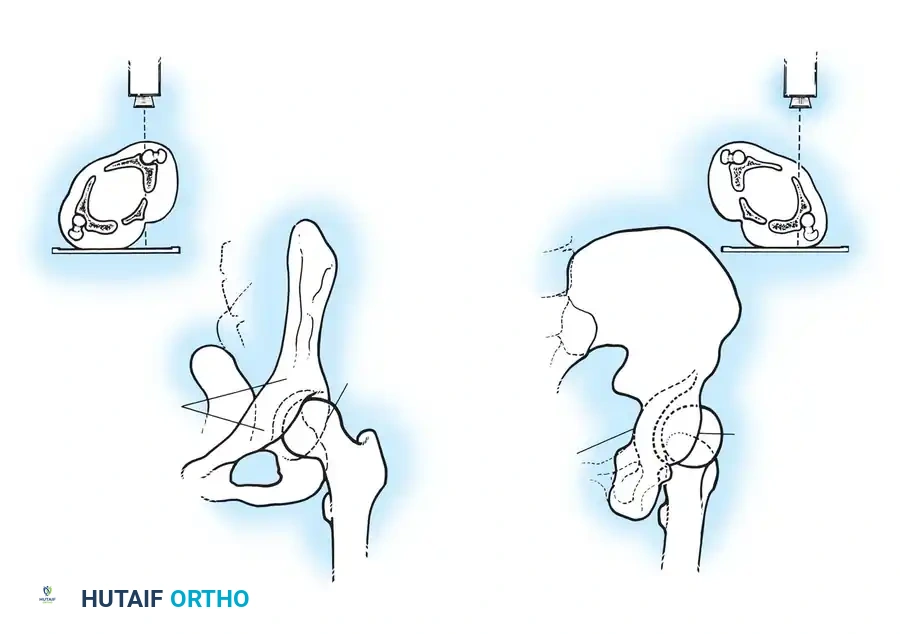
To fully conceptualize the fracture in three dimensions, the 45-degree oblique views described by Judet are absolutely mandatory. The Iliac Oblique View, obtained by rolling the patient 45 degrees toward the uninjured side, brilliantly profiles the posterior column and the anterior wall of the acetabulum. Conversely, the Obturator Oblique View, obtained by rolling the patient 45 degrees toward the injured side, profiles the anterior column and the posterior wall of the acetabulum. Mastery of these plain radiographic lines is the hallmark of a competent pelvic surgeon, as they form the basis of the Letournel classification system, which divides fractures into five elementary patterns (anterior wall, anterior column, posterior wall, posterior column, transverse) and five associated patterns (T-shaped, posterior column/posterior wall, transverse/posterior wall, anterior column/posterior hemitransverse, both-column).

Advanced Imaging and Digital Templating
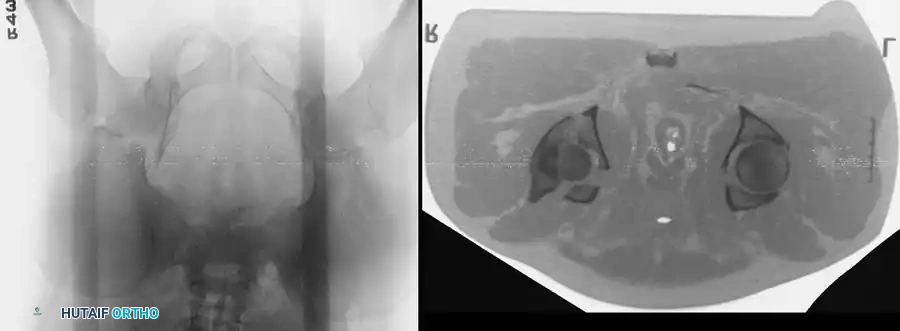
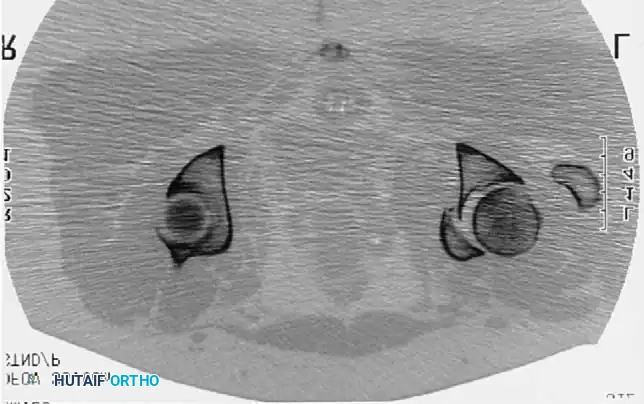
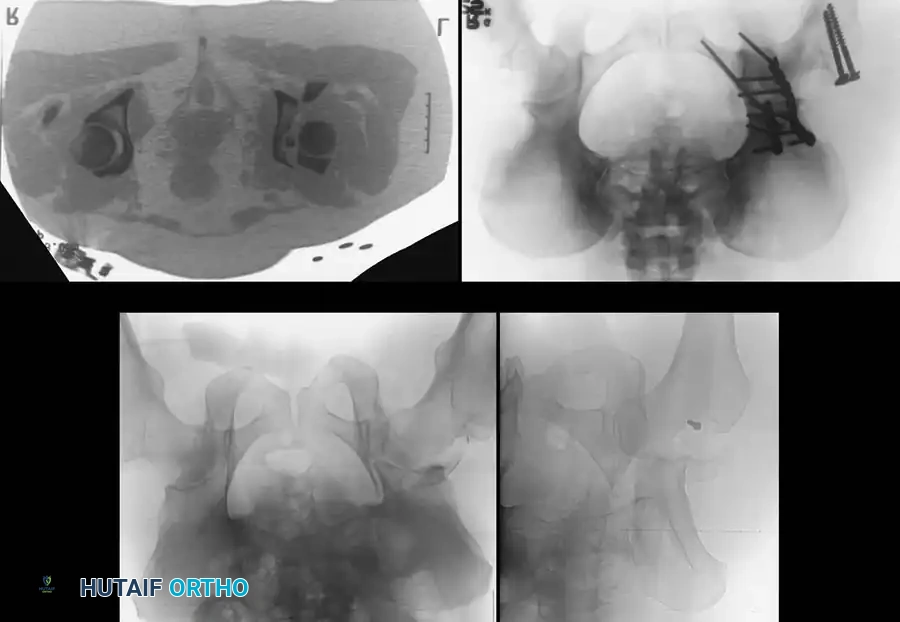
While plain radiographs provide the foundational understanding, fine-cut Computed Tomography (CT) scanning (2-3 mm slices) with 2D multiplanar (coronal and sagittal) and 3D surface-rendered reconstructions is the undisputed gold standard for modern surgical planning. CT imaging excels at identifying subtle intra-articular osteochondral fragments, assessing the degree of marginal impaction of the articular cartilage (which must be elevated and bone-grafted during surgery), and quantifying the exact size and comminution of posterior wall fragments. Furthermore, modern digital templating software allows the surgeon to perform virtual fracture reductions, select appropriate plate lengths and contours, and plan optimal screw trajectories, particularly for critical intraosseous column screws.

Patient Positioning and Operating Room Setup
Patient positioning is dictated entirely by the chosen surgical approach and must be executed with obsessive attention to detail. For the Kocher-Langenbeck approach, patients are typically positioned prone or in the lateral decubitus position on a radiolucent Jackson table. The prone position allows for easier reduction of the posterior column as gravity assists in pulling the femoral head anteriorly out of the defect, while the lateral position facilitates easier airway management and allows for a concurrent anterior approach if a "flop" is anticipated. For anterior approaches (Ilioinguinal or Stoppa), the patient is positioned supine. The entire lower extremity must be prepped and draped free to allow for intraoperative manipulation, traction, and assessment of joint stability. Fluoroscopy (C-arm) must be brought in prior to prepping to ensure that perfect AP, Iliac Oblique, and Obturator Oblique views can be obtained without obstruction from the table columns.

Step-by-Step Surgical Approach and Fixation Technique
The Kocher-Langenbeck Approach
The Kocher-Langenbeck (K-L) approach is the absolute workhorse for posterior pathology, providing unparalleled access to the posterior wall, posterior column, and the greater and lesser sciatic notches. The incision begins near the posterior superior iliac spine (PSIS), extends to the greater trochanter, and continues distally along the femoral shaft. The fascia lata and gluteus maximus fascia are incised in line with the skin. The gluteus maximus is split bluntly along its muscle fibers, taking immense care to identify and protect the sciatic nerve as it emerges distal to the piriformis. The short external rotators (obturator internus and gemelli) are identified, tagged, and tenotomized near their femoral insertion. Retracting these muscles posteriorly provides a muscular cushion that protects the sciatic nerve during retraction. The capsule is then incised, and the fracture is exposed.
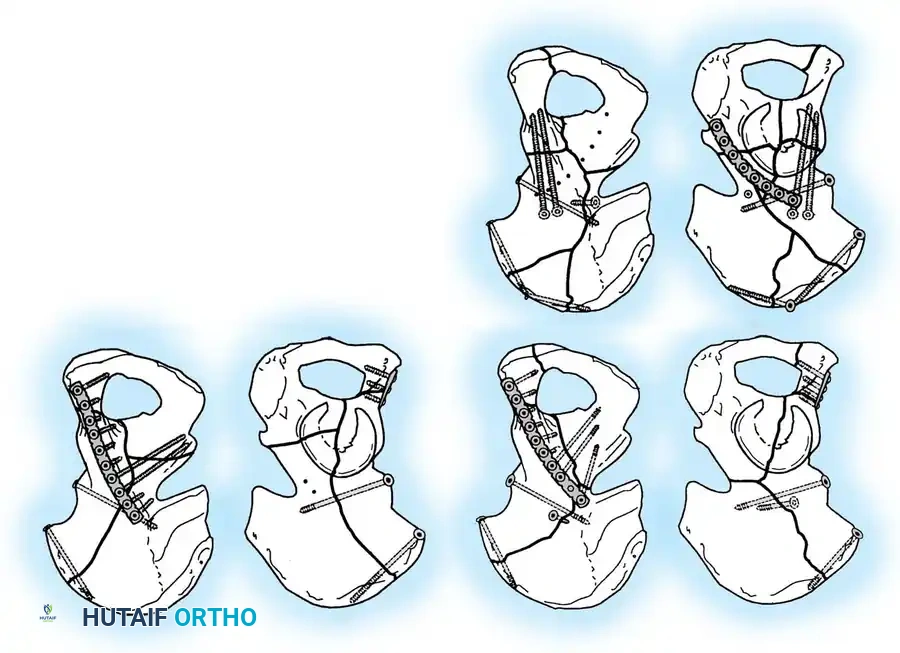
Reduction of posterior wall fragments often requires meticulous debridement of the fracture bed, removal of hematoma, and evaluation of the joint for loose bodies. Marginal impaction must be recognized; the impacted articular cartilage is carefully elevated using a periosteal elevator, and the resulting metaphyseal void is filled with cancellous autograft or allograft. The posterior wall is then reduced and provisionally held with K-wires or a ball-spike pusher. Definitive fixation typically involves interfragmentary lag screws (if the fragment is large enough) followed by a properly contoured reconstruction plate applied in a buttress mode along the posterior rim of the acetabulum. The plate must be under-contoured slightly to provide dynamic compression against the wall fragment when the screws are tightened.
Anterior Approaches: Ilioinguinal and Modified Stoppa
For anterior column, anterior wall, and certain both-column fractures, anterior approaches are mandated. The classic Ilioinguinal approach, described by Letournel, provides extensive access to the entire inner table of the innominate bone from the SI joint to the pubic symphysis. It utilizes three distinct windows defined by the neurovascular structures: the lateral window (lateral to the iliopsoas/femoral nerve), the middle window (between the iliopsoas and the external iliac vessels), and the medial window (medial to the vessels). This approach is highly technical, requiring meticulous dissection and mobilization of the external iliac artery and vein, and poses a risk of vascular injury or lymphatic disruption.
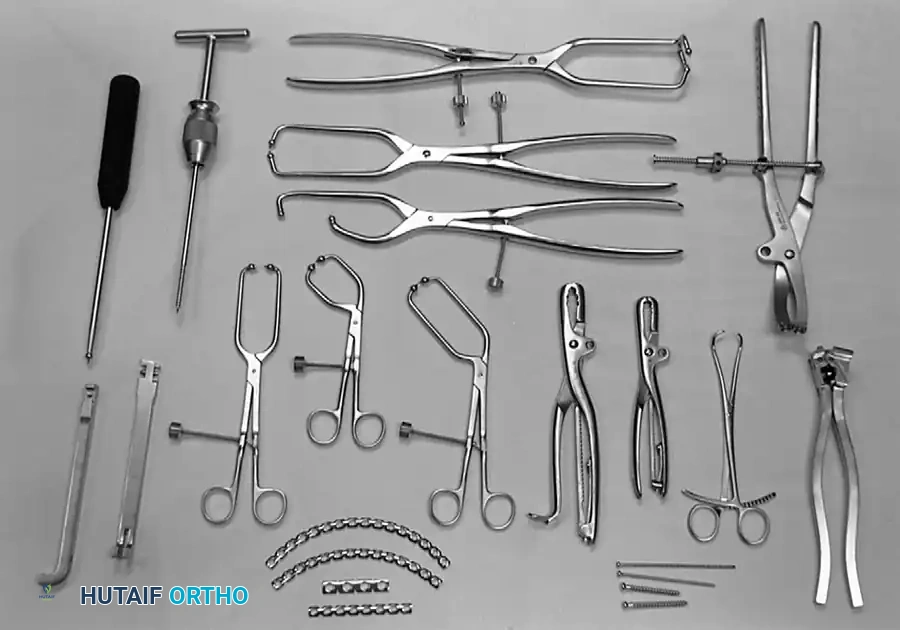
In recent years, the Modified Stoppa approach (often combined with a lateral window of the ilioinguinal) has gained immense popularity. This intrapelvic, extraperitoneal approach is performed through a Pfannenstiel incision. The rectus abdominis is split or elevated, and the surgeon dissects along the pelvic brim. This provides direct, orthogonal access to the quadrilateral plate and the medial aspect of the posterior column, which is exceptionally difficult to visualize through the standard ilioinguinal approach. The Corona Mortis must be identified and ligated early in this approach. Reduction techniques involve the use of specialized intrapelvic clamps (e.g., the Jungbluth clamp or Matta pelvic reduction instruments) and fixation is often achieved with infra-pectineal plating or quadrilateral surface buttress plates.

Complications, Incidence Rates, and Salvage Management
Neurologic and Thromboembolic Complications
The surgical management of acetabular fractures is fraught with a high incidence of severe complications. Neurologic injury, specifically to the sciatic nerve, is the most dreaded immediate complication. The incidence of iatrogenic sciatic nerve palsy following the Kocher-Langenbeck approach historically approaches 2-10%. The peroneal division of the nerve is particularly susceptible to stretch injury due to its lateral position and tethering at the fibular head. Intraoperative somatosensory and motor evoked potential (SSEP/MEP) monitoring is highly recommended to provide real-time feedback regarding nerve strain. If a palsy is noted post-operatively, management is generally expectant with the use of an ankle-foot orthosis (AFO) to prevent equinus contracture, though recovery is often incomplete.

Thromboembolic events, including deep vein thrombosis (DVT) and fatal pulmonary embolism (PE), are exceptionally common due to the convergence of Virchow’s triad: endothelial injury from massive pelvic trauma, venous stasis from immobility, and a hypercoagul
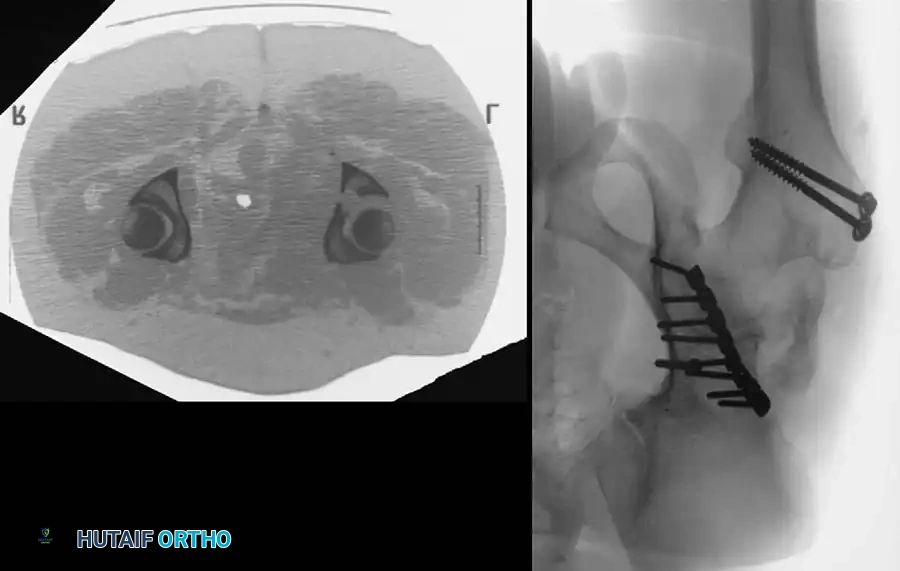
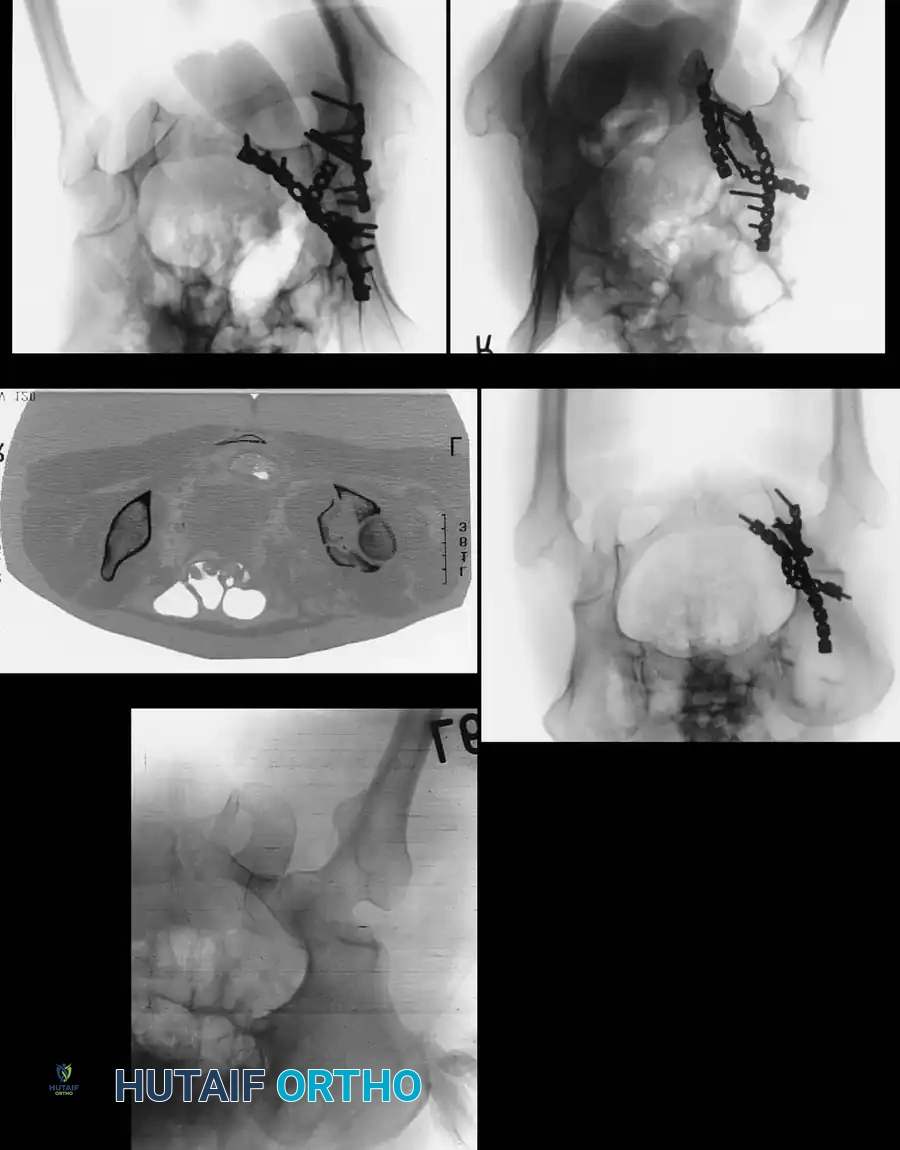
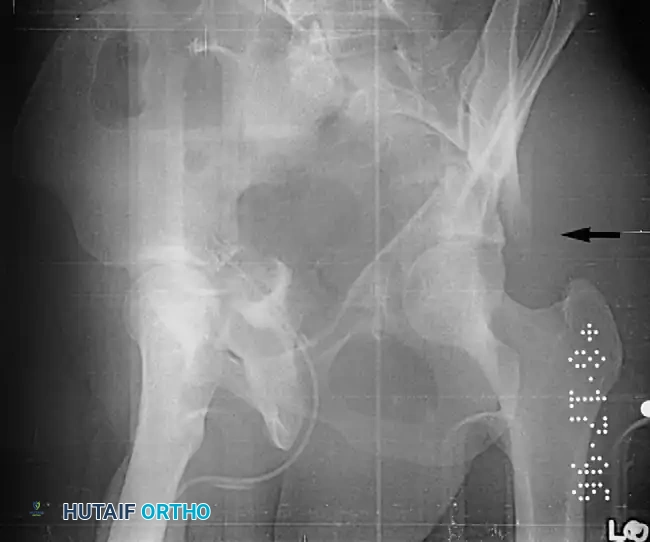
Clinical & Radiographic Imaging Archive