Mastering Posterior Wall Acetabular Fracture Fixation: An Intraoperative Guide

Key Takeaway
Join us in the OR for an immersive masterclass on posterior wall acetabular fracture ORIF. We'll meticulously cover comprehensive surgical anatomy, detailed preoperative planning, precise patient positioning on the fracture table, and the granular, step-by-step intraoperative execution via the Kocher-Langenbeck approach. Learn critical pearls, pitfalls, and postoperative management strategies for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of posterior wall acetabular fractures represents one of the most technically demanding challenges in modern orthopedic traumatology. As orthopedic surgeons, we recognize that this procedure is far more than the simple mechanical reassembly of osseous fragments; it is a meticulous reconstruction of a highly constrained, weight-bearing articulation. The overarching objective of open reduction and internal fixation (ORIF) in this context is the precise restoration of articular congruity and hip stability, which are the absolute prerequisites for mitigating the devastating long-term sequelae of post-traumatic osteoarthritis. When we enter the operating theater for these cases, we must operate with a profound respect for the complex biomechanics and delicate vascularity of the hip joint.
Posterior wall fractures are the most frequently encountered subset of acetabular fractures, accounting for approximately 25% to 33% of all cases according to the foundational epidemiological studies by Letournel and Judet. These injuries are classically the result of high-energy trauma, most commonly motor vehicle collisions where a severe axial load is transmitted longitudinally through the femoral shaft to the acetabulum. The classic "dashboard injury" occurs when the hip is positioned in approximately 90 degrees of flexion and neutral abduction; the resultant force vector drives the femoral head directly into the posterior rim of the acetabulum, leading to fracture, posterior subluxation, or complete posterior dislocation. The exact morphology of the fracture—whether it involves the posterosuperior roof, the posteroinferior horn, or presents as a highly comminuted multifragmentary pattern—is heavily dictated by the precise degree of hip flexion, adduction, and rotation at the exact moment of impact.
The pathogenesis of this injury goes beyond the bony disruption. Posterior fracture-dislocations are frequently associated with severe soft tissue trauma, including devastating capsuloligamentous tearing, labral avulsions, and severe contusions or impaction injuries to the femoral head articular cartilage. Marginal impaction of the acetabular articular cartilage and subchondral bone is observed in up to 50% of these cases. If this impaction is not identified and anatomically elevated during the index procedure, the resulting articular step-off will inevitably lead to rapid, accelerated joint destruction. Furthermore, the surgeon must maintain a high index of suspicion for concomitant injuries, including ipsilateral femoral shaft fractures, knee ligamentous disruptions, and occult pelvic ring instability, which can severely complicate patient positioning and post-operative rehabilitation.
Understanding the natural history of non-operatively managed displaced posterior wall fractures underscores the critical necessity of surgical intervention. Historical cohorts managed with prolonged skeletal traction demonstrated unacceptably high rates of chronic pain, recurrent instability, and rapid progression to end-stage arthritis. Today, our standard of care dictates that any posterior wall fracture resulting in dynamic hip instability or significant articular incongruity mandates urgent surgical stabilization. The operative endeavor requires an absolute mastery of three-dimensional pelvic osteology, a comprehensive understanding of the surrounding neurovascular topography, and a refined surgical technique capable of achieving rigid osteosynthesis without compromising the precarious blood supply to the femoral head or the acetabular fragments.
Detailed Surgical Anatomy and Biomechanics
Before a single incision is made, the operating surgeon must possess an absolute, uncompromising mastery of pelvic and acetabular anatomy. The hip joint is a highly constrained, multiaxial ball-and-socket synovial joint. The inherent stability of this articulation relies on the intricate interplay between the deep bony architecture of the acetabulum, the robust capsuloligamentous envelope, and the dynamic dynamic stabilization provided by the surrounding pelvifemoral musculature.
Osteology and Articular Geometry
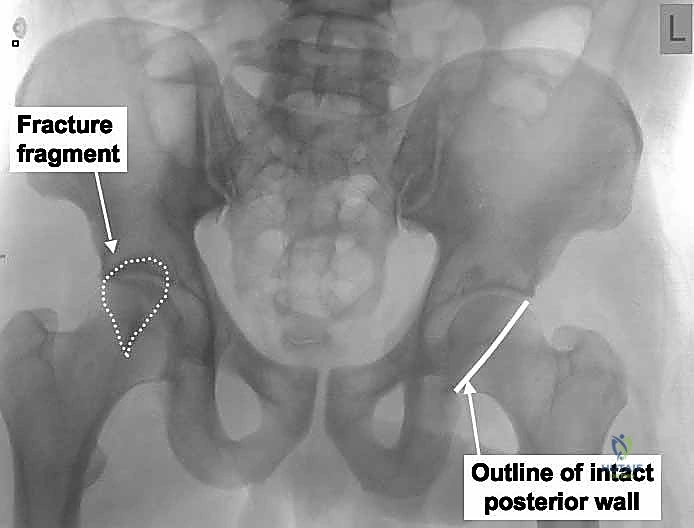
The acetabulum is a complex hemispherical cavity formed by the confluence of the ilium, ischium, and pubis, classically conceptualized by Letournel as a two-column structure. The anterior and posterior columns form an inverted 'Y' configuration, anchoring the acetabulum to the axial skeleton via the thick trabecular bone of the sciatic buttress. The posterior column, which descends from the sciatic notch to the ischial tuberosity, provides the structural foundation for the posterior wall. In a pure posterior wall fracture, the structural integrity of the posterior column itself—and thus the radiographic ilioischial line—remains completely intact. This is the critical radiographic distinction between an isolated wall fracture and a posterior column fracture.

The articular surface of the acetabulum is restricted to the horseshoe-shaped lunate facies, which surrounds the non-articular cotyloid fossa. The posterior wall forms the critical posterior rim of this socket. The most vital segment of the articular surface is the weight-bearing dome, or the anatomic roof, which is located superiorly between the anterior inferior iliac spine and the superior margin of the greater sciatic notch. The integrity of this dome is evaluated radiographically using the 45-degree roof arc measurements on AP and Judet views. The posterior wall can be further subdivided into a posterosuperior segment, which acts as the crucial bridge connecting the structural roof to the posterior column, and a posteroinferior segment, which encompasses the posterior horn of the articular cartilage. Comminution or displacement in the posterosuperior segment is particularly treacherous, as it directly compromises the weight-bearing capacity of the superior dome.
The geometry of the posterior wall is highly variable among individuals, but its biomechanical function is universal: it prevents posterior translation of the femoral head during the normal gait cycle, particularly during activities involving hip flexion and internal rotation, such as rising from a seated position or climbing stairs. Loss of this bony restraint, even if the fragment appears small on two-dimensional imaging, can lead to dynamic subluxation. The critical threshold for instability has historically been debated, but modern biomechanical studies indicate that fractures involving more than 20-30% of the posterior wall frequently result in gross instability, necessitating rigid internal fixation to restore the mechanical block to posterior dislocation.
Capsuloligamentous and Labral Contributions to Stability
The bony architecture is augmented by a dense, unyielding capsuloligamentous complex. The joint capsule extends from the bony rim of the acetabulum to the intertrochanteric line of the femur anteriorly, and to the base of the femoral neck posteriorly. This capsule is not a homogenous structure; it is heavily reinforced by distinct capsular ligaments. Anteriorly, the robust iliofemoral ligament (the Y ligament of Bigelow) provides massive resistance to hyperextension. Inferiorly, the pubofemoral ligament limits abduction. Posteriorly, the ischiofemoral ligament spirals from the ischial rim to the greater trochanter, tightening during internal rotation and extension. During a posterior fracture-dislocation, the ischiofemoral ligament and the posterior capsule are violently avulsed or torn, contributing significantly to post-injury instability.
Intimately associated with the capsular origin is the acetabular labrum, a dense ring of fibrocartilage attached to the bony rim. The labrum is not merely a static bumper; it deepens the acetabular socket, effectively increasing the articular surface area by approximately 10%. More importantly, the labrum functions as a vital fluid seal, maintaining a layer of pressurized synovial fluid that provides essential hydrodynamic lubrication and cartilage nutrition, while simultaneously creating a negative intra-articular pressure (the "suction seal" effect) that significantly enhances joint stability.
In the setting of a posterior wall fracture, the labrum is almost universally involved. It may be avulsed from the bony rim, incarcerated within the joint space, or remain attached to the displaced bony fragment. Meticulous preservation and repair of the labrum during surgical fixation are paramount. Excision of a torn labrum should be strictly avoided unless the tissue is irreparably macerated, as loss of the labral seal drastically alters joint contact mechanics, increases peak articular contact stresses, and accelerates the onset of degenerative joint disease.
Vascular Topography and Perfusion Dynamics
The acetabulum and the proximal femur reside within a rich, complex, and highly vulnerable vascular network. The surgeon must navigate this topography with extreme caution to prevent catastrophic hemorrhage and to preserve the delicate blood supply to the osseous structures. The pelvic bone itself receives its endosteal supply from nutrient vessels, but the critical periosteal supply is derived from the extensive muscular attachments. The iliolumbar artery provides constant nutrient vessels to the internal iliac fossa, while the superior gluteal artery (SGA) is the dominant supplier to the external iliac wing and the superior acetabular roof.
The superior gluteal artery exits the pelvis through the greater sciatic notch, intimately coursing superior to the piriformis muscle. It is at extreme risk of laceration during deep dissection or if the fracture pattern extends proximally into the sciatic notch. Retraction in this area must be carefully controlled. The obturator artery supplies the inferior aspects of the acetabulum and sends a critical acetabular branch through the obturator canal to feed the cotyloid fossa via the ligamentum teres. The inferior gluteal artery exits below the piriformis and contributes to the anastomotic ring around the posterior hip.
Perhaps the most critical vascular consideration during the posterior approach to the acetabulum is the preservation of the medial circumflex femoral artery (MCFA). The deep branch of the MCFA is the primary blood supply to the femoral head. It courses posterior to the obturator externus and anterior to the quadratus femoris, ascending along the posterosuperior femoral neck. When releasing the short external rotators during a Kocher-Langenbeck approach, the surgeon must meticulously preserve the obturator externus and leave a substantial cuff of the quadratus femoris intact at its femoral insertion. Overzealous dissection in this region will inevitably disrupt the MCFA, leading to devastating iatrogenic avascular necrosis (AVN) of the femoral head.
Neurovascular Proximity and Iatrogenic Risk Zones
Neurologic injury is a profound risk in acetabular surgery, both from the initial trauma and from iatrogenic surgical trauma. The sciatic nerve is the most frequently injured neural structure, with injury rates approaching 10-15% in posterior fracture-dislocations. The nerve exits the pelvis through the greater sciatic notch, typically inferior to the piriformis muscle, and courses distally deep to the gluteus maximus and superficial to the short external rotators (superior gemellus, obturator internus, inferior gemellus, and quadratus femoris).

The peroneal division of the sciatic nerve is particularly vulnerable due to its lateral and posterior position within the nerve sheath, its relative tethering at the fibular head, and its larger, less protected fascicular structure. During the Kocher-Langenbeck approach, the sciatic nerve must be visually identified early in the deep dissection, gently mobilized, and continuously protected. Retractors placed in the lesser sciatic notch or along the posterior column must be positioned with extreme care to avoid compression or excessive tension on the nerve. The knee must be kept flexed to at least 60-80 degrees throughout the procedure to minimize tension on the sciatic nerve.
While less commonly discussed, the pudendal nerve is also at significant risk, primarily due to positioning rather than direct surgical dissection. The pudendal nerve can be compressed against the perineal post of the fracture table, especially when heavy longitudinal traction is applied to the injured extremity. This can result in devastating pudendal neuralgia, perineal numbness, and erectile dysfunction. Meticulous padding of the perineal post and minimizing the duration and magnitude of traction are critical preventative measures.
Exhaustive Indications and Contraindications
The decision-making process for the surgical management of posterior wall acetabular fractures requires a nuanced synthesis of radiographic data, biomechanical principles, and patient-specific factors. Unlike many other skeletal injuries where a trial of conservative management is acceptable, displaced posterior wall fractures are predominantly surgical lesions. The threshold for operative intervention is low, driven by the universally poor functional outcomes associated with chronic hip instability and articular incongruity.
Evaluating Joint Stability and Articular Congruity
The primary, absolute indication for surgical intervention is dynamic hip instability. Instability is clinically and radiographically evident when the femoral head cannot be maintained concentrically within the acetabulum without continuous traction, or when dynamic stress fluoroscopy demonstrates subluxation. Historically, the size of the posterior wall fragment was used as a surrogate marker for stability; fractures involving greater than 50% of the posterior wall dimension on axial CT were deemed unstable, while those less than 20% were considered stable. However, modern orthopedic traumatology has largely abandoned rigid reliance on these two-dimensional measurements.

Today, dynamic stress fluoroscopy under general anesthesia is the gold standard for determining stability in equivocal cases. With the patient anesthetized, the hip is taken through a range of motion, specifically flexion to 90 degrees with superimposed adduction and axial loading. If the joint subluxates, surgical fixation is absolutely mandated, regardless of the calculated fragment size. Furthermore, any fracture that results in an intra-articular step-off or gap greater than 2 millimeters within the weight-bearing dome is an indication for ORIF.
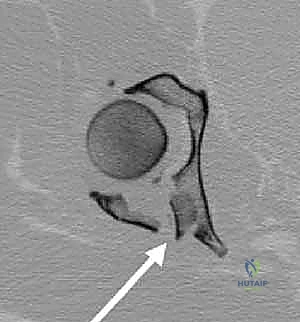
Marginal impaction is another critical indication. When the femoral head impacts the posterior wall, it frequently crushes the articular cartilage and subchondral bone into the underlying cancellous bed. This creates a severe articular defect that will not spontaneously remodel. Identification of marginal impaction on preoperative CT scans necessitates surgical intervention to elevate the impacted segment, graft the resulting metaphyseal void, and support the articular surface with a buttress plate. Finally, the presence of intra-articular loose bodies (bony or chondral fragments) that prevent concentric reduction of the femoral head mandates surgical arthrotomy and debridement.
| Indication / Contraindication Category | Specific Clinical / Radiographic Criteria | Rationale and Clinical Nuance |
|---|---|---|
| Absolute Indications for Surgery | Dynamic Hip Instability | Subluxation under stress fluoroscopy or inability to maintain concentric reduction guarantees rapid joint destruction. |
| Intra-articular Loose Bodies | Incarcerated fragments prevent anatomic reduction and cause severe third-body wear to the articular cartilage. | |
| Marginal Impaction | Impacted osteochondral fragments create a step-off that drastically increases contact stresses, mandating elevation and grafting. | |
| Articular Step-off > 2mm | Any incongruity in the weight-bearing dome > 2mm significantly alters joint biomechanics and accelerates osteoarthritis. | |
| Relative Indications | Fragment Size 20% - 50% | Gray zone requiring dynamic stress testing. Many of these will prove unstable and require fixation. |
| Associated Sciatic Nerve Palsy | Progressive neurologic deficit may warrant exploration and decompression, though routine exploration for static deficits is debated. | |
| Absolute Contraindications | Severe Systemic Instability | Hemodynamic instability, severe coagulopathy, or overwhelming sepsis precluding safe administration of anesthesia. |
| Local Soft Tissue Infection | Active infection at the planned surgical site (e.g., infected Morel-Lavallée lesion) requires prior debridement and clearance. | |
| Relative Contraindications | Extreme Osteoporosis | Poor bone stock may preclude rigid internal fixation; acute total hip arthroplasty (THA) may be considered in elderly patients. |
| Pre-existing Advanced OA | If the joint is already destroyed by severe osteoarthritis, reconstructing the fracture may be futile; acute THA is often preferred. |
Patient-Specific and Systemic Considerations
While the radiographic parameters heavily influence the decision, the patient's physiological status is equally paramount. Open reduction of the acetabulum is a major, blood-loss-heavy procedure. Patients presenting in extremis, with profound hemorrhagic shock from associated pelvic ring injuries or solid organ damage, must undergo aggressive resuscitation and damage control orthopedics before definitive acetabular reconstruction is considered.
Age and bone quality are critical determinants. In the young, high-demand patient, every effort must be made to anatomically reconstruct the native joint to delay or prevent the need for arthroplasty. Conversely, in the elderly patient with severe osteopenia or pre-existing symptomatic coxarthrosis, extensive internal fixation of a highly comminuted posterior wall may be destined to fail due to hardware pullout or rapid articular collapse. In these specific scenarios, acute total hip arthroplasty (THA)—often utilizing specialized acetabular cages or multi-hole revision shells to bypass the fracture—is increasingly recognized as a definitive, single-stage solution that permits immediate full weight-bearing and faster functional recovery.
Pre-Operative Planning, Templating, and Patient Positioning
The success of an acetabular fracture operation is largely determined before the patient ever enters the operating room. Meticulous preoperative planning is the blueprint for surgical execution. It allows the surgeon to anticipate the three-dimensional fracture morphology, select the optimal surgical approach, prepare the necessary instrumentation, and foresee potential intraoperative pitfalls.
Advanced Diagnostic Imaging Modalities
The initial evaluation begins with the standard anteroposterior (AP) radiograph of the pelvis. This provides a global overview of the injury, identifying dislocations, major fracture lines, and associated pelvic ring disruptions. However, the AP view alone is profoundly insufficient for surgical planning. The Judet views—the iliac oblique and the obturator oblique—are mandatory. These 45-degree angled projections orthogonally separate the anterior and posterior columns. The obturator oblique view profiles the anterior column and the posterior wall, while the iliac oblique view profiles the posterior column and the anterior wall.


Despite the utility of plain radiography, fine-cut Computed Tomography (CT) with two-dimensional multiplanar reformats and three-dimensional surface rendering is the absolute cornerstone of modern acetabular fracture planning. The CT scan must be obtained after the initial closed reduction of any hip dislocation to accurately assess the concentricity of the joint. Axial, coronal, and sagittal reformats allow the surgeon to precisely quantify the size of the posterior wall fragment, assess the degree of comminution, and, critically, identify the presence and depth of marginal articular impaction.
Three-dimensional CT reconstructions provide a topographical map of the fracture, allowing the surgeon to virtually rotate the hemipelvis and visualize the injury exactly as it will appear during the surgical exposure. Furthermore, modern software allows for digital subtraction of the femoral head, providing an unobstructed view of the acetabular articular surface and any incarcerated intra-articular fragments.
Digital Templating and Pre-Surgical Optimization
With the high-resolution imaging available, precise digital templating is performed. The surgeon must determine the anticipated trajectory of lag screws and the optimal position and contour of the buttress plates. Posterior wall fractures typically require a combination of interfragmentary lag screws (often 3.5mm or 4.0mm partially threaded screws) and a neutralizing buttress plate spanning from the ischial tuberosity to the intact ilium above the superior gluteal notch.
Pre-contouring plates using 3D-printed pelvic models based on the patient's specific CT data is an advanced technique that significantly reduces intraoperative time and minimizes soft tissue stripping. The surgeon must also anticipate the need for specialized implants, such as spring plates (minifragment plates cut and bent to provide a continuous compressive force) for highly comminuted, small rim fragments that cannot accommodate a standard lag screw. Additionally, preparation for bone grafting is essential; the surgical team must ensure the availability of autograft harvest tools (e.g., for harvesting from the greater trochanter) or appropriate structural and cancellous allograft to fill metaphyseal voids following the elevation of impacted fragments.
Prone Positioning on the Fracture Table
For the isolated posterior wall fracture, the Kocher-Langenbeck approach is universally utilized, and the patient is most optimally positioned prone on a specialized radiolucent fracture table. This positioning is a complex, orchestrated process that requires meticulous attention to detail to ensure adequate exposure, facilitate reduction, and prevent catastrophic iatrogenic nerve injuries.
The patient is carefully rolled prone onto the fracture table. The injured lower extremity is secured in a well-padded boot attached to a traction spar. Crucially, a distal femoral skeletal traction pin is routinely placed. This allows for powerful, controlled longitudinal traction that bypasses the knee joint, protecting the knee ligaments from excessive stretch. The hip is positioned in neutral extension to slight hyperextension to relax the anterior structures, and the knee is flexed to a minimum of 80 degrees. This knee flexion is absolutely critical; it drastically reduces tension on the sciatic nerve, allowing for safer retraction during the deep exposure.
The uninjured contralateral leg is positioned in neutral extension and secured in a boot, ensuring it is out of the way of the C-arm fluoroscopy unit. The perineal post, which provides counter-traction, is a major hazard zone. It must be heavily padded with specialized gel pads or foam to distribute pressure evenly and prevent pudendal nerve crush injuries. The post should be positioned against the contralateral inner thigh rather than directly in the perineum.

Before the patient is prepped and draped, the C-arm must be brought into the field to confirm that high-quality, unobstructed AP, iliac oblique, and obturator oblique views can be obtained. The ability to achieve these orthogonal views intraoperatively without compromising the sterile field is an absolute requirement for verifying the reduction and ensuring that hardware has not penetrated the articular surface.
Step-by-Step Surgical Approach and Fixation Technique
The execution of the surgical plan demands a seamless integration of anatomical knowledge, delicate tissue handling, and forceful yet precise reduction maneuvers. The operation is a sequential progression from superficial exposure to deep structural reconstruction.
The Kocher-Langenbeck Approach
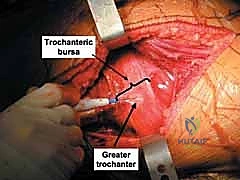
The Kocher-Langenbeck approach is the workhorse for posterior acetabular pathology. The incision begins near the posterior superior iliac spine (PSIS), extends distally toward the greater trochanter, and then curves longitudinally down the lateral aspect of the femoral shaft. The subcutaneous tissues are divided to expose the fascia lata and the gluteal fascia.
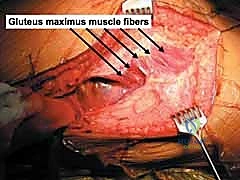
The fascia is incised in line with the skin incision. Proximally, the gluteus maximus is split bluntly in line with its muscle fibers. This split must not extend too far medially, as it risks denervating the proximal muscle bellies supplied by the inferior gluteal nerve and risks massive hemorrhage from branches of the superior gluteal artery. Distally, the iliotibial band is incised. A Charnley or similar self-retaining retractor is placed to hold the massive gluteus muscle retracted posteriorly.
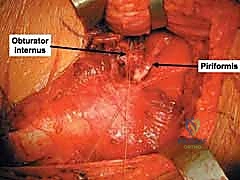
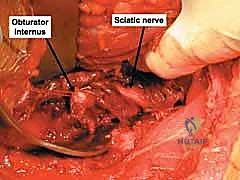
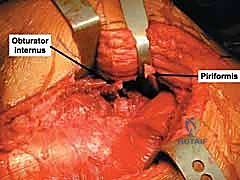
Deep to the gluteus maximus, the subgluteal space is developed. The first and most critical step at this depth is the visual identification of the sciatic nerve. It is typically found embedded in fat overlying the short external rotators. Once identified, it is gently mobilized using a vessel loop or a blunt retractor. No sharp instruments should be used near the nerve, and continuous, heavy retraction must be strictly avoided to prevent neuropraxia.
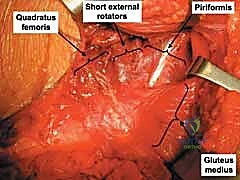
The short external rotators—the piriformis, superior gemellus, obturator internus, and inferior gemellus—are identified. These tendons are tagged with heavy non-absorbable sutures and transected approximately 1.5 to 2.0 centimeters from their insertion on the greater trochanter. The piriformis is reflected posteriorly, protecting the superior gluteal neurovascular bundle. The obturator internus and gemelli are reflected medially over the sciatic notch; they act as a vital muscular cushion, protecting the sciatic nerve from the edges of metallic retractors placed in the lesser sciatic notch.
The quadratus femoris is approached with extreme caution. To protect the ascending branch of the medial circumflex femoral artery, only the superior half to two-thirds of the quadratus femoris should be released, and the surgeon must leave a thick cuff of muscle attached to the femur. Complete release at the bony insertion is a common error that leads to catastrophic devascularization of the femoral head.
Joint Debridement and Articular Inspection
With the posterior column and joint capsule exposed, the true extent of the injury becomes apparent. The posterior capsule is typically torn or avulsed by the displaced bony fragments. The surgeon carefully mobilizes the major fracture fragments, reflecting them outward on their remaining capsular hinges to preserve their tenuous blood supply.
A formal capsulotomy is performed to visualize the interior of the joint. Longitudinal traction is applied via the distal femoral pin to distract the femoral head from the acetabulum. The joint space is thoroughly irrigated and inspected. All hematoma, small non-viable chondral fragments, and bony debris are meticulously evacuated. The femoral head is inspected for chondral shearing injuries or impaction fractures (Pipkin lesions).
The acetabular labrum is carefully evaluated. If it is avulsed from the rim but remains structurally intact, it is tagged with fine sutures for later repair. The most critical step at this juncture is the identification of marginal impaction. The surgeon must look deep into the subchondral bone of the posterior wall defect. Impacted fragments are often rotated and driven deeply into the cancellous bone of the posterior column, creating a severe incongruity that will completely thwart any attempt at anatomical reduction of the main wall fragments.
Reduction Maneuvers and Provisional Fixation
The reconstruction begins from the inside out. If marginal impaction is present, these osteochondral fragments must be carefully elevated using a dental pick or a small osteotome. They are gently levered back into their anatomic position, using the curvature of the reduced femoral head as a template for the articular surface. Once elevated, a significant cavitary void remains in the underlying cancellous bone. This void must be densely packed with bone graft—typically cancellous autograft harvested locally from the greater trochanter or high-quality allograft—to provide structural support and prevent the elevated fragment from subsiding.

Following the restoration of the articular surface, the main posterior wall fragments are reduced. This is achieved by carefully manipulating the fragments back into their bed using a combination of digital pressure, ball-spike pushers, and specialized reduction forceps (e.g., Jungbluth clamps or point-to-point clamps). The reduction must be absolutely anatomic; even a 1-2 millimeter step-off at the articular margin is unacceptable.
Once reduced, the fragments are provision
Clinical & Radiographic Imaging Archive