Surgical Management of Rheumatoid and Osteoarthritic Thumb Deformities
Key Takeaway
Thumb deformities, particularly in rheumatoid arthritis and osteoarthritis, present complex biomechanical challenges. The Nalebuff classification categorizes rheumatoid thumb deformities into four types, guiding surgical intervention based on joint correctability and destruction. Treatment ranges from synovectomy and soft-tissue reconstruction to arthrodesis and arthroplasty. This guide details the pathomechanics, indications, and step-by-step surgical techniques required to restore thumb stability, alignment, and function in the arthritic hand.
INTRODUCTION TO THUMB DEFORMITIES
The thumb is responsible for approximately 40% to 50% of overall hand function, serving as the critical post for pinch, grasp, and fine motor manipulation. Deformities of the thumb, whether driven by the inflammatory synovitis of rheumatoid arthritis (RA) or the degenerative articular wear of osteoarthritis (OA), severely compromise hand biomechanics.
Rheumatoid thumb deformities are frequently complex, involving the trapeziometacarpal (CMC), metacarpophalangeal (MCP), and interphalangeal (IP) joints either individually or in a cascading combination. Successful surgical management requires a profound understanding of the underlying pathomechanics, a precise assessment of joint correctability, and a tailored approach that balances motion preservation with structural stability.
CLASSIFICATION OF RHEUMATOID THUMB DEFORMITIES
The classification system proposed by Nalebuff remains the gold standard for understanding the predictable patterns of rheumatoid thumb collapse. This system divides thumb deformities into four distinct types, providing a vital framework for developing a comprehensive treatment algorithm.
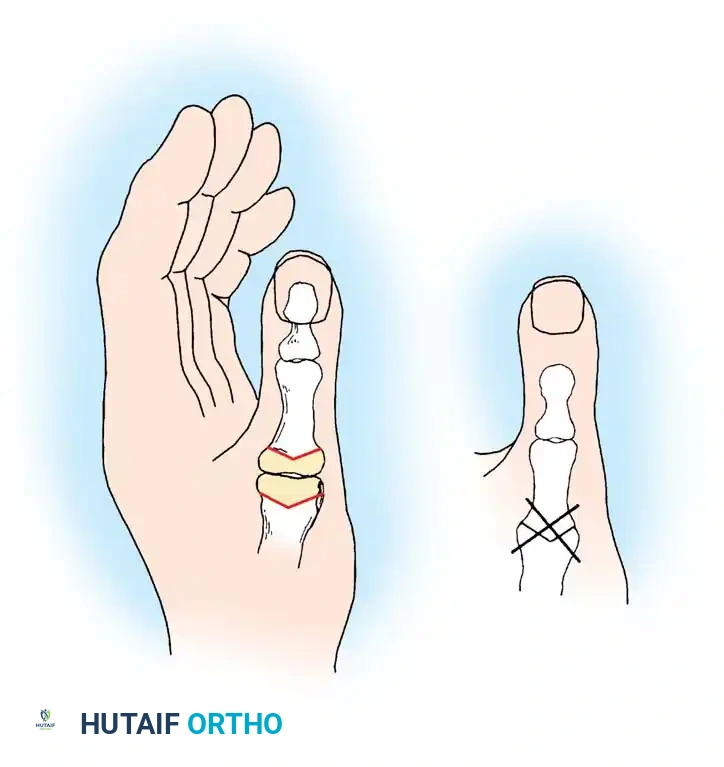
Type I: Boutonnière Deformity
The Type I deformity is the most common rheumatoid thumb presentation. It is characterized by MCP joint flexion and IP joint hyperextension.
Pathomechanics:
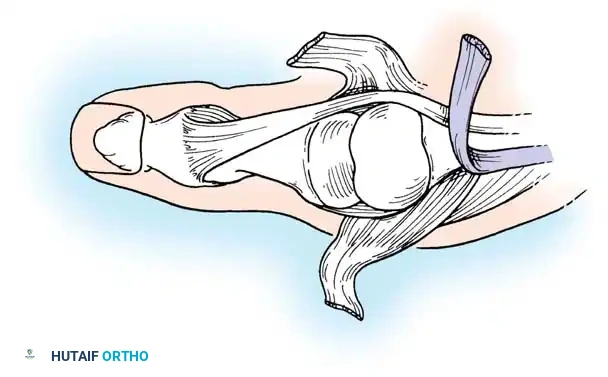
The deformity initiates with aggressive synovitis at the MCP joint. The proliferating pannus bulges dorsally, stretching the dorsal capsule and the extensor hood. This leads to the attenuation and eventual rupture of the extensor pollicis brevis (EPB) insertion at the base of the proximal phalanx. Concurrently, the extensor pollicis longus (EPL) tendon subluxates ulnarly and volarly, dropping below the axis of rotation of the MCP joint to act as a paradoxical flexor.
The resulting biomechanical imbalance forces the MCP joint into fixed flexion and palmar subluxation. The intrinsic muscles (abductor pollicis brevis and adductor pollicis) bypass the MCP joint, concentrating their extension force on the IP joint, driving it into severe hyperextension. Early in the disease process, these joints can be passively corrected; however, with chronicity, the volar plate contracts, and the deformity becomes rigidly fixed.
Treatment Algorithm:
* Early/Correctable (Normal Radiographs): MCP synovectomy combined with extensor tendon reconstruction (EPB advancement and EPL rerouting).
* Fixed MCP Contracture (Correctable IP, Joint Destruction): MCP arthrodesis provides a highly functional, stable pillar for pinch.
* Pan-Articular Destruction: In older, low-demand patients, MCP arthroplasty combined with IP arthrodesis may be indicated. If bone stock is severely compromised, combined MCP and IP arthrodesis is the most reliable salvage procedure.
Type II Deformity
Type II is a rare variant that combines the features of a Boutonnière deformity with concurrent CMC joint disease.
Pathomechanics:
Patients present with MCP joint flexion, IP joint hyperextension, and subluxation or dislocation of the trapeziometacarpal joint.
Treatment Algorithm:
Management requires addressing the entire ray. Combinations of IP fusion, MCP arthroplasty or fusion, and CMC arthroplasty (resection or implant) are utilized to restore the longitudinal axis of the thumb.
Type III: Swan-Neck Deformity
The Type III deformity is the second most common pattern and represents the inverse of the Boutonnière collapse.
Pathomechanics:
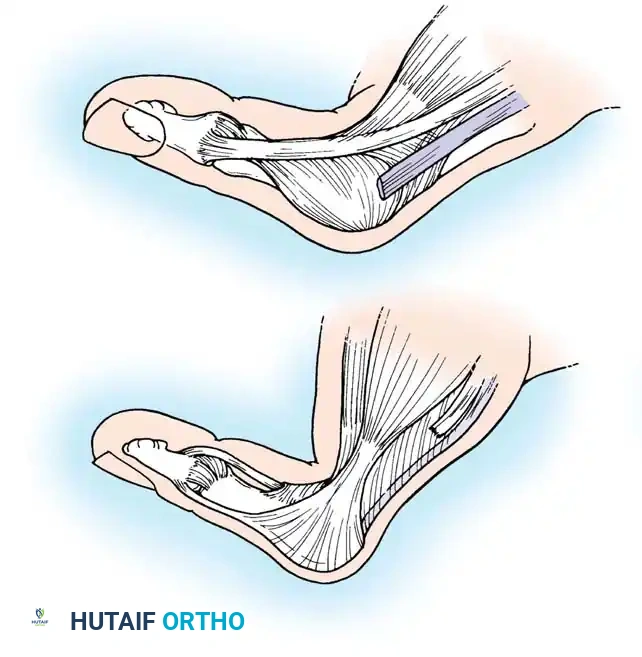
The primary driver of a Type III deformity is disease at the trapeziometacarpal (CMC) joint. Chronic synovitis leads to capsular attenuation and lateral/dorsal subluxation of the metacarpal base. As the CMC joint dislocates, the first metacarpal falls into a fixed adduction contracture.
To clear the thumb from the palm and maintain a functional grasp, the patient forcefully hyperextends the MCP joint. Over time, this constant extension force stretches the volar plate of the MCP joint, leading to severe hyperextension, while the IP joint subsequently falls into flexion due to the tension on the flexor pollicis longus (FPL).
Treatment Algorithm:
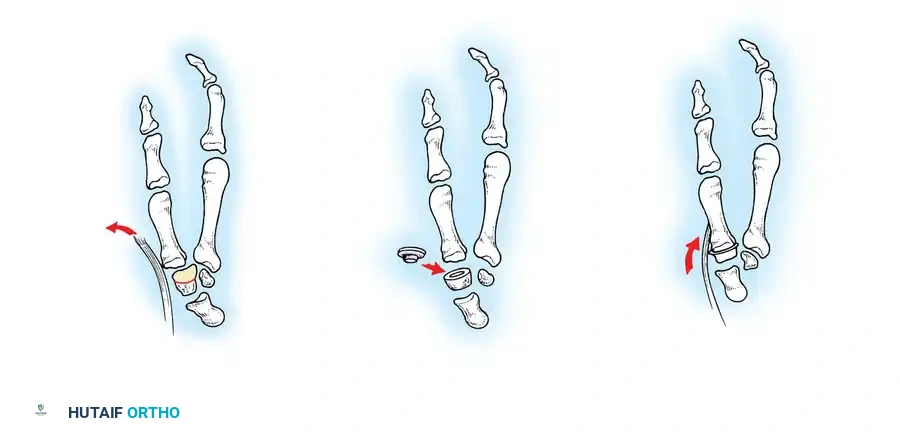
* Mild Deformity (Mobile Joints): CMC hemiarthroplasty or resection arthroplasty (e.g., LRTI). Total trapezial resection with unconstrained replacement is generally avoided due to the high risk of instability.
* Advanced Deformity (Fixed MCP Hyperextension): CMC resection arthroplasty combined with MCP joint arthrodesis. Fusing the MCP joint in 15 degrees of flexion effectively shortens the ray, often relieving the metacarpal adduction contracture without requiring a formal release of the first web space or first dorsal interosseous muscle.
Type IV: Gamekeeper Deformity
The Type IV deformity is characterized by profound instability of the MCP joint, specifically mimicking a chronic ulnar collateral ligament (UCL) injury.
Pathomechanics:
Chronic rheumatoid synovitis distends the MCP joint capsule, selectively attenuating the UCL. This results in severe radial deviation (abduction) of the proximal phalanx and a compensatory adduction of the first metacarpal.
Treatment Algorithm:
* Mild Deformity: MCP synovectomy, UCL reconstruction, and adductor release.
* Advanced Deformity: MCP arthrodesis is the gold standard to provide a stable post for index finger pinch.
OSTEOARTHRITIS OF THE THUMB
Unlike rheumatoid arthritis, which is primarily a synovial disease, osteoarthritis (OA) is driven by articular cartilage degeneration and altered joint kinematics. The thumb joints affected by OA are, in descending order of frequency: the trapeziometacarpal (CMC), metacarpophalangeal (MCP), and distal interphalangeal (DIP) joints.
Biomechanics of CMC Osteoarthritis:
The CMC joint is a highly mobile biconcave saddle joint. Pelligrini’s seminal studies demonstrated a consistent pattern of trapezial articular eburnation that exceeds the wear on the first metacarpal articular surface. This supports the concept that trapeziometacarpal translational instability—specifically attenuation of the anterior oblique ligament (beak ligament)—is the primary precipitating factor in CMC osteoarthritis.
At the MCP joint, osteoarthritic disability is most frequently caused by ligamentous instability, predominantly of the UCL, leading to a degenerative Gamekeeper-type presentation.
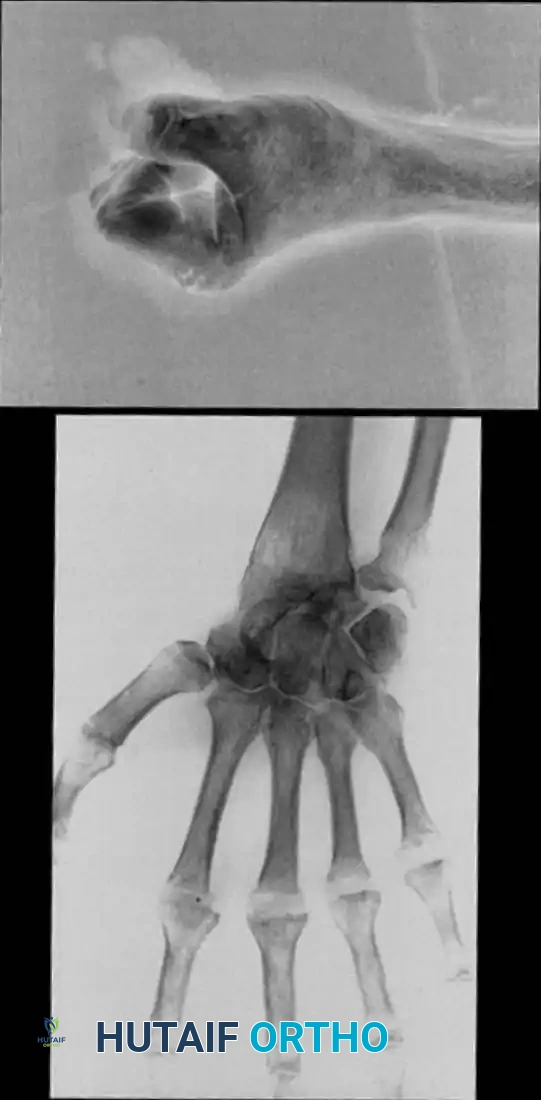
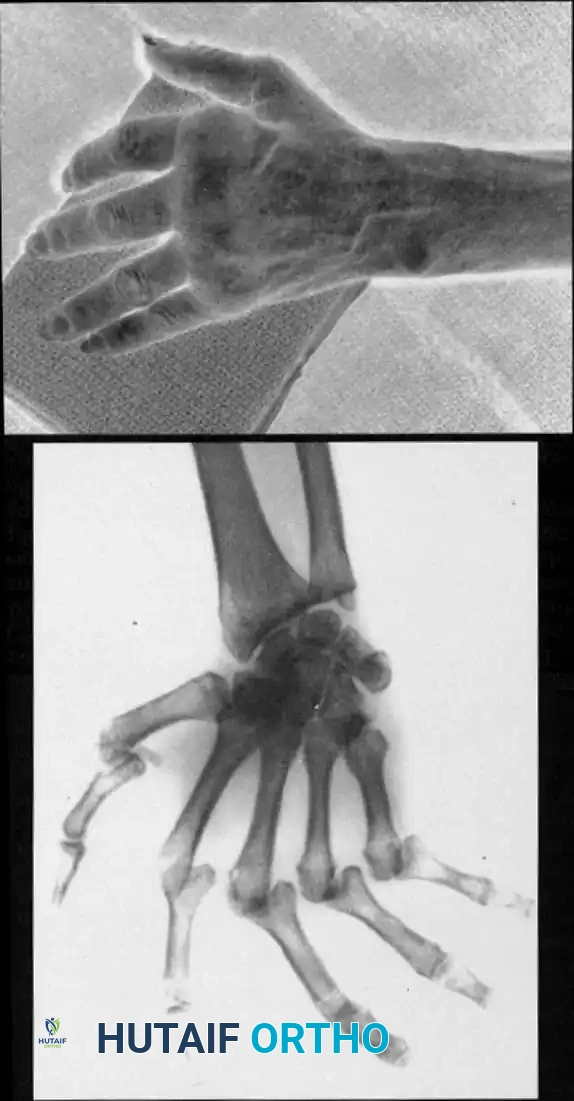
💡 Clinical Pearl: Radiographic Assessment
Always obtain a true Robert's view (hyperpronated AP of the thumb) and stress views to accurately assess the degree of CMC joint subluxation and the presence of pantrapezial arthritis before finalizing a surgical plan.
SURGICAL TECHNIQUES: SYNOVECTOMY
Synovectomy is a joint-preserving procedure indicated for early rheumatoid disease where there is painful, boggy synovitis that has failed medical management (DMARDs/biologics) for 6 months, provided there is no significant radiographic joint destruction or fixed instability.
Technique 70-14: Thumb Interphalangeal Joint Synovectomy
- Approach: Utilize a straight dorsal incision or a longitudinal curved incision over the IP joint. If a prominent palmar synovial bulge is present, a radial midaxial incision is preferred to allow access to the volar pouch.
- Exposure: If using the dorsal approach, carefully elevate the skin flaps protecting the terminal branches of the superficial radial nerve. Release the extensor tendon longitudinally on either the radial or ulnar margin.
- Synovectomy: Open the joint capsule dorsally. Use a fine curet and a micro-rongeur to meticulously excise the hypertrophic synovium from the dorsal, lateral, and volar recesses.
- Ligament Management: If the radial collateral ligament must be released for adequate exposure, reattach it securely to the base of the distal phalanx using a micro-suture anchor or a pull-out wire.
- Stabilization: Fix the IP joint temporarily with a 0.045-inch Kirschner wire (K-wire) in full extension to protect the ligamentous repair.
- Closure: Repair the extensor mechanism with 4-0 non-absorbable sutures. Close the skin and apply a volar splint.
Postoperative Protocol:
Sutures and the K-wire are removed at 10 to 14 days. Active range of motion (ROM) is initiated. The IP joint is splinted in extension between exercise sessions for an additional 2 weeks.
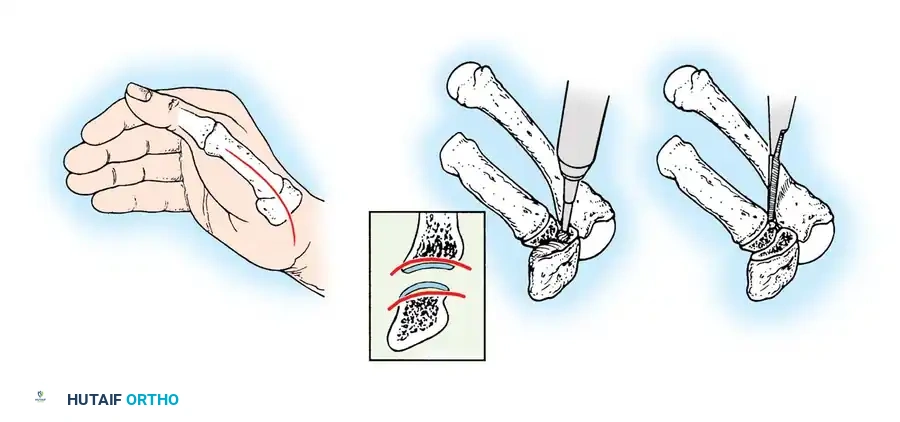
Technique 70-15: Thumb Metacarpophalangeal Joint Synovectomy
- Approach: Make a dorsal curved or lazy-S incision over the MCP joint.
- Exposure: Identify the EPL and EPB tendons. In rheumatoid disease, these are often displaced ulnarly. Incise the dorsal joint capsule longitudinally between the EPB and EPL tendons, retracting them radially and ulnarly, respectively.
- Synovectomy: Perform a thorough synovectomy using a rongeur and curet.
- Volar Access: Apply longitudinal traction to the proximal phalanx to distract the joint. Flex the MCP joint to 45 degrees to visualize and clear the volar synovial recesses. Meticulously debride the synovium surrounding the collateral ligaments without compromising their structural integrity.
- Closure: Close the capsule and the extensor mechanism anatomically. Apply a thumb spica splint maintaining the MCP joint in full extension.
Postoperative Protocol:
Splint and sutures are removed at 10 to 14 days. Active ROM exercises begin immediately, but static splinting in extension is continued at night and between exercises for 2 more weeks.
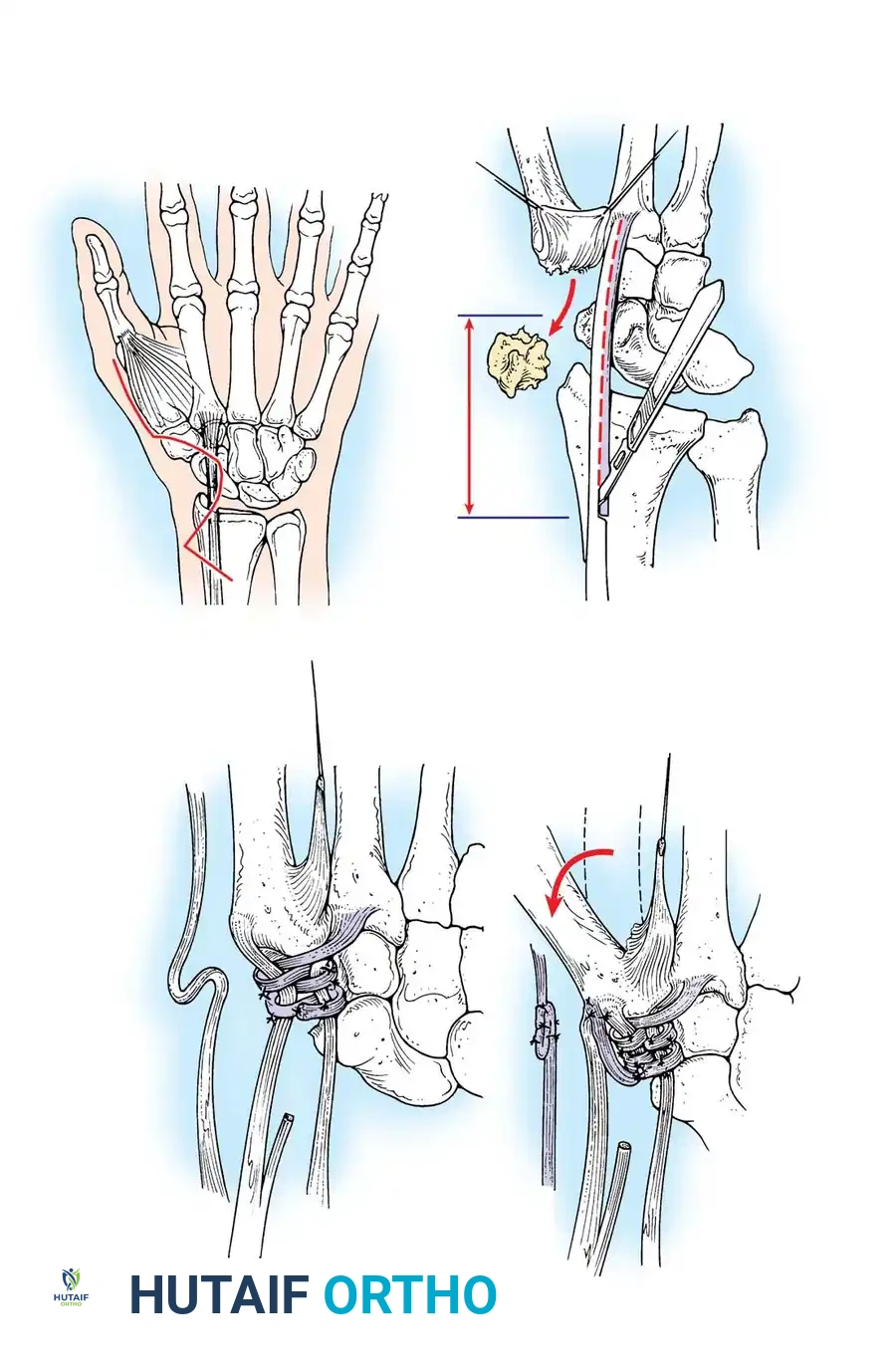
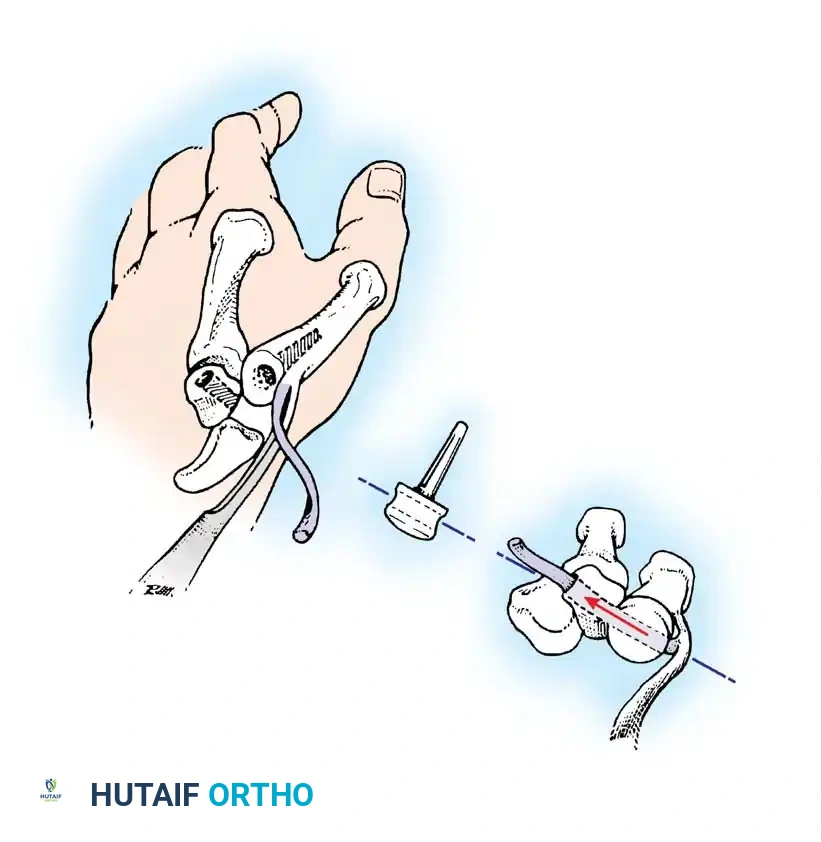
Technique 70-16: Thumb Trapeziometacarpal Joint Synovectomy
- Approach: Make a straight dorsal incision curving slightly volar-ward over the CMC joint (Wagner approach).
- Nerve Protection: Carefully retract the skin flaps. Surgical Warning: The sensory branches of the superficial radial nerve and the lateral antebrachial cutaneous nerve are highly vulnerable here. Retract them gently with vessel loops.
- Exposure: Identify the abductor pollicis longus (APL) and EPB. Open the CMC capsule longitudinally on the dorsal aspect of the APL.
- Synovectomy: Clear the joint of all proliferative synovium. Inspect the articular cartilage and the anterior oblique ligament.
- Closure: Imbricate the capsule during closure if laxity is noted. Splint the thumb in palmar abduction and extension.
🔪 Surgical Warning
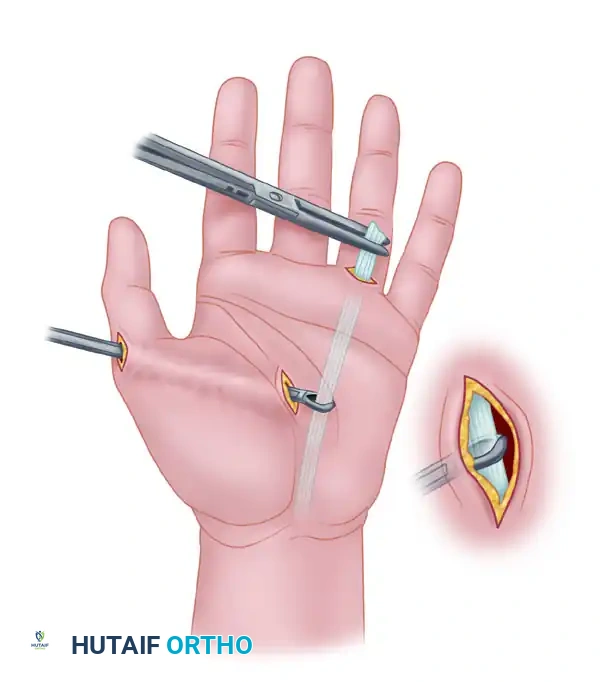
If extensive ligamentous laxity is noted during CMC synovectomy, simple capsulorrhaphy will fail. Proceed directly to a ligament reconstruction (e.g., Eaton-Littler reconstruction using the FCR tendon) to stabilize the basal joint.
SURGICAL TECHNIQUES: SOFT-TISSUE RECONSTRUCTION
Soft-tissue reconstructions are indicated for passively correctable deformities where the articular cartilage remains radiographically preserved.
Technique 70-17: Interphalangeal Soft-Tissue Reconstruction
- Indications: Passively correctable IP joint deformity without severe radiographic destruction.
- Approach: Make a longitudinal dorsal incision over the IP joint. If severe skin contracture is present, design the incision to allow for a Z-plasty closure.
- Release: Perform a meticulous tenolysis of the extensor tendon. Retract the extensor apparatus laterally and incise the dorsal capsule and the dorsal fibers of the collateral ligaments to release the extension contracture.
- Fixation: Flex the IP joint to 20 to 30 degrees and stabilize it with a transarticular K-wire.
- Closure: Perform a Z-plasty closure if dorsal skin coverage is inadequate. Small distal defects can be left to heal by secondary intention.
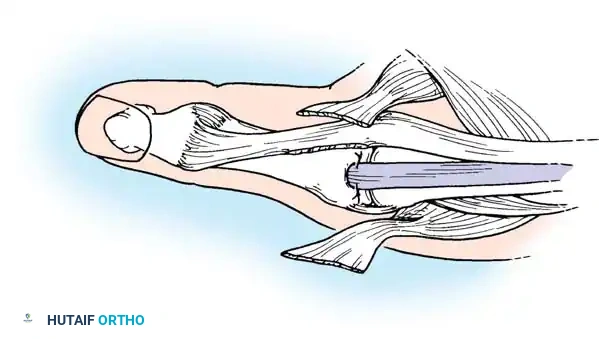
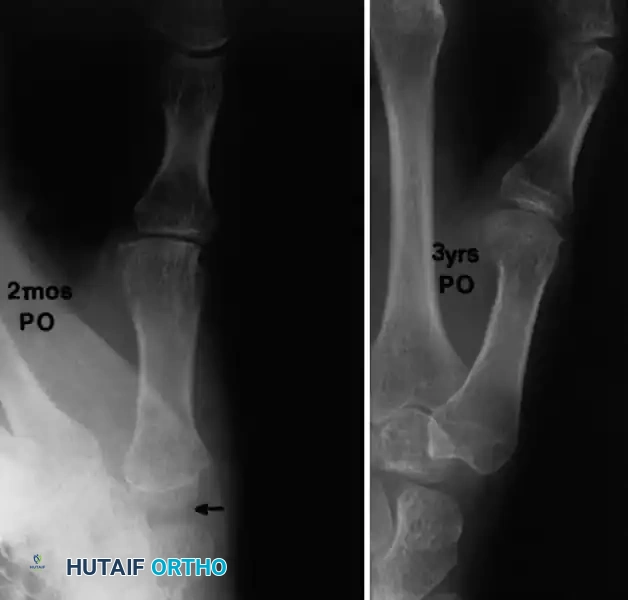
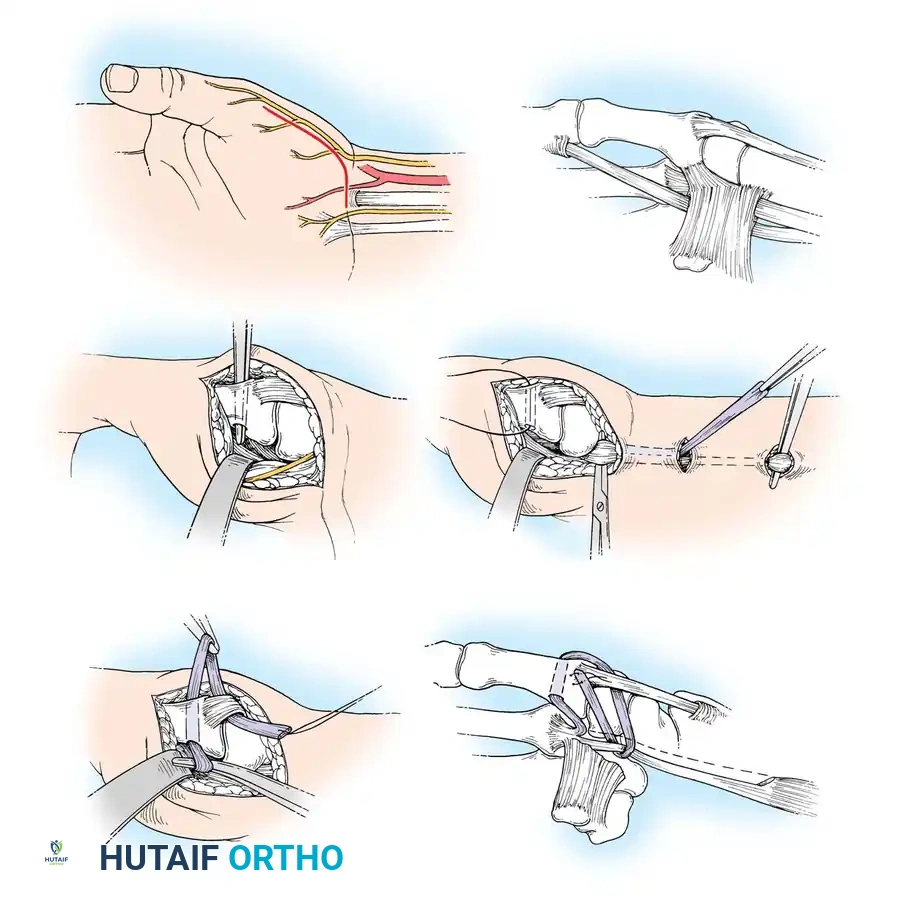
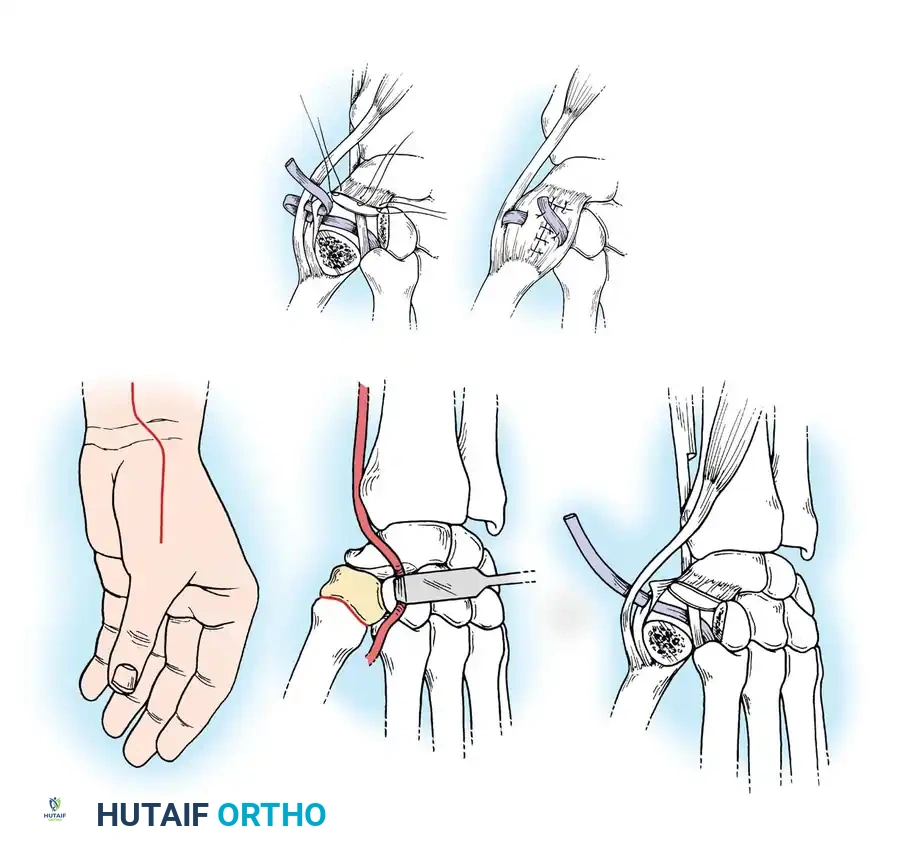
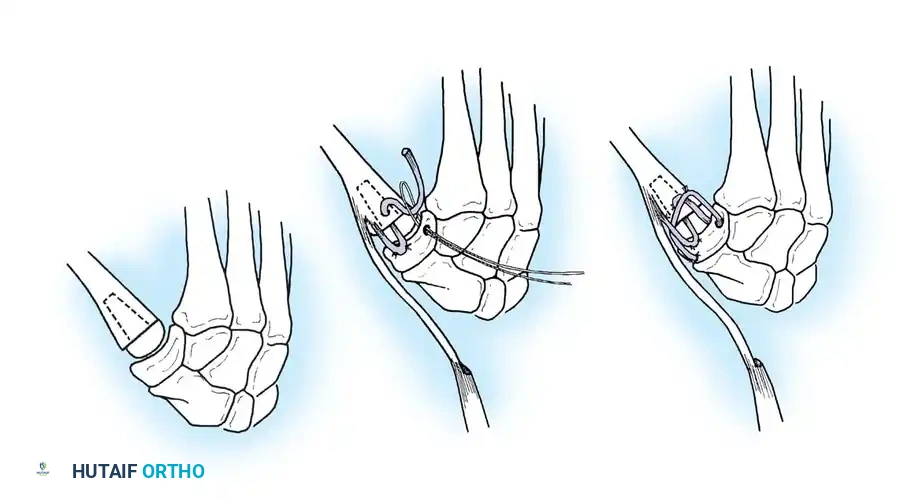
Technique 70-18: Metacarpophalangeal Synovectomy with Extensor Tendon Reconstruction
This procedure is the workhorse for early, correctable Type I (Boutonnière) deformities.
- Assessment: Confirm under anesthesia that the MCP flexion deformity is passively correctable.
- Approach: Make a curved dorsal incision over the MCP joint. Protect the cutaneous nerves.
- Tendon Isolation: Identify the EPL and EPB. The EPL is typically subluxated ulnarly. Make a longitudinal incision between them.
- EPL Release: Incise along both sides of the EPL to free it from the intrinsic muscle attachments (adductor expansion). Transect the EPL over the distal third of the proximal phalanx.
- EPB Release: Dissect the EPB from its attenuated insertion at the base of the proximal phalanx and detach it from the extensor mechanism.
- Capsular Flap: Create a transverse incision in the dorsal capsule. Mobilize a distally based capsular flap attached to the proximal phalanx. Make a transverse slit in the base of this flap.
- Synovectomy: Perform a comprehensive MCP joint synovectomy.
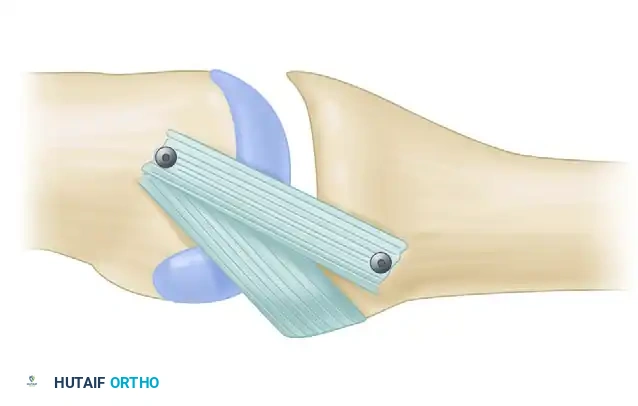
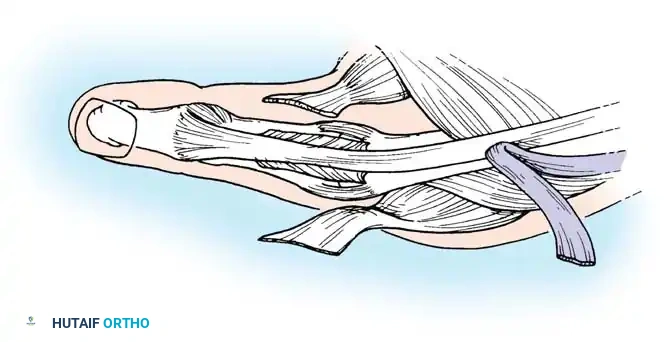
- EPL Rerouting: Pass the proximal stump of the EPL through the transverse slit in the capsular flap. Reflect it back onto itself. Hold the MCP joint in full extension and suture the EPL to itself under appropriate tension. This effectively uses the EPL to reconstruct the dorsal capsule and provide a robust extension force to the proximal phalanx.
- EPB Transfer: Apply distal traction to the EPB tendon and weave it into the side of the rerouted EPL.
- Intrinsic Balancing: Ensure the intrinsic tendon insertions are positioned dorsally to maintain active IP extension and prevent volar subluxation. Tighten the transverse fibers over the distal phalanx if an extensor lag is present.
- Fixation: Pin the MCP joint in full extension with a 0.045-inch K-wire.
Postoperative Protocol:
The K-wire is removed at 4 weeks. Splinting of the MCP joint in extension continues for an additional 2 weeks, while IP joint motion is encouraged early.
Technique 70-19: Reconstruction of the Metacarpophalangeal Joint for Rheumatoid Arthritis (Inglis et al.)
- Approach: Make a longitudinal incision over the dorsum of the metacarpophalangeal joint from the middle of the proximal phalanx to the mid-shaft of the first metacarpal.
- Exposure: Identify and meticulously protect the sensory branches of the radial nerve. Isolate the extensor pollicis longus (EPL) and extensor pollicis brevis (EPB) tendons.
- Tendon Management: In severe deformities, the EPL is displaced volarly and ulnarly. Mobilize the EPL and release any adherent intrinsic expansions.
- Joint Preparation: Perform a radical synovectomy. If the joint surfaces
Associated Surgical & Radiographic Imaging

📚 Medical References
You Might Also Like