Flexor Hallucis Longus Pathology: Comprehensive Orthopedic Review & Surgical Reference
Key Takeaway
Flexor Hallucis Longus (FHL) pathology describes conditions like tendinopathy and tenosynovitis affecting the FHL muscle-tendon unit, causing posterior ankle pain. Prevalent in dancers and athletes, its management relies on understanding FHL surgical anatomy, biomechanics, and differentiation from other ankle pathologies to guide effective conservative or surgical interventions.
You are seeing a 22-year-old professional ballet dancer in the clinic. She complains of chronic, deep posteromedial ankle pain that is exacerbated by "en pointe" positions. She has failed 4 months of physiotherapy, NSAIDs, and activity modification. On clinical examination, she has pain on resisted plantarflexion of the hallux and pain with the "Dancer’s FHL Test."

How would you approach the diagnosis, and what are the critical anatomical structures you must protect if you were to proceed to surgery?
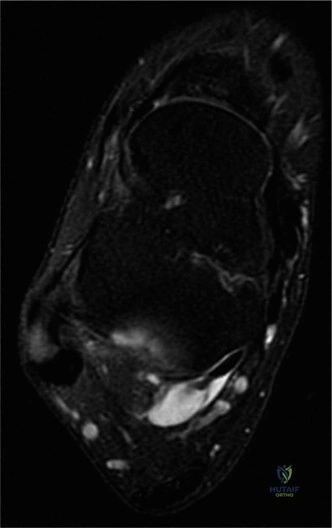
Candidate: I would start with an MRI to confirm FHL tenosynovitis and rule out an os trigonum. Clinically, I'd check for posterior impingement. If surgery is needed, I'd use a posteromedial approach. I need to be careful of the posterior tibial neurovascular bundle, which lies anterior and medial to the FHL tendon, and the medial calcaneal nerve branches.
Candidates often focus solely on the FHL tendon, failing to demonstrate a systematic approach to the "posteromedial danger zone." They often forget to mention the specific relationship of the posterior tibial neurovascular bundle (which is the most common iatrogenic injury site) or overlook the "knot of Henry" biomechanical implications in the midfoot.
The candidate structures the answer: 1) Diagnostics: MRI as gold standard to evaluate tendon integrity and bone marrow edema (impingement). 2) Anatomical Landmarks: Define the interval between the FDL and FHL. 3) Danger Zone: Explicitly mention the posterior tibial neurovascular bundle (tibial nerve/posterior tibial artery) lying superficial (anterior/medial) to the FDL, which must be retracted with care. 4) Surgical Pearls: Mentioning the release of the fibro-osseous tunnel at the sustentaculum tali and the need to evaluate for accessory ossicles (os trigonum) or hypertrophic soft tissues.
During the procedure, you have identified the FHL tendon, but you find significant fibrosis and a partial-thickness tear of the tendon measuring approximately 40% of its cross-sectional area. How does this change your management, and what are the implications for the patient's recovery?
Candidate: I would debride the frayed edges of the tendon. Since the tear is less than 50%, I would likely leave it after a thorough tenosynovectomy and decompression of the tunnel. I would advise the patient to have a longer period of immobilization and delayed return to full impact activity to allow the tendon to heal.
The candidate fails to provide a specific threshold for repair (often cited as >50%) or forgets to mention the importance of addressing the underlying "mechanical conflict" (e.g., the os trigonum or fibro-osseous constriction) that caused the tear in the first place. They also fail to mention the post-operative rehabilitation modification.
A high-scoring answer addresses: 1) Decision Matrix: Confirm that for <50% tears, debridement and decompression of the fibro-osseous tunnel is sufficient, whereas >50% often warrants repair (modified Kessler/Bunnell). 2) Mechanical Correction: Stress that if the impingement (os trigonum) isn't addressed, the tendon will continue to attrite regardless of debridement. 3) Rehab: Explicitly mention a staged, prolonged protocol—protected weight-bearing in a CAM boot for 2–6 weeks, with delayed introduction of great toe active plantarflexion to avoid tensile stress on the debrided area.
