Mastering Limited Intercarpal Fusions: Scaphocapitate, Scaphocapitolunate, and Lunotriquetral Arthrodesis

Key Takeaway
Scaphocapitate and scaphocapitolunate arthrodesis are highly effective salvage procedures for localized carpal arthritis, midcarpal instability, and specific patterns of carpal collapse. Success relies on meticulous joint decortication, precise restoration of carpal alignment—particularly achieving a radioscaphoid angle of 50 degrees—and rigid internal fixation using lag screws or Kirschner wires supplemented with robust autologous bone grafting.
INTRODUCTION TO LIMITED INTERCARPAL ARTHRODESIS
Limited intercarpal arthrodesis represents a cornerstone in the surgical management of localized carpal arthritis, carpal instability, and specific patterns of carpal collapse, such as Scapholunate Advanced Collapse (SLAC) or Scaphoid Nonunion Advanced Collapse (SNAC). The primary biomechanical objective of these procedures is to eliminate painful motion at arthritic or unstable articulations while preserving functional, pain-free motion at the remaining unaffected radiocarpal and midcarpal joints.
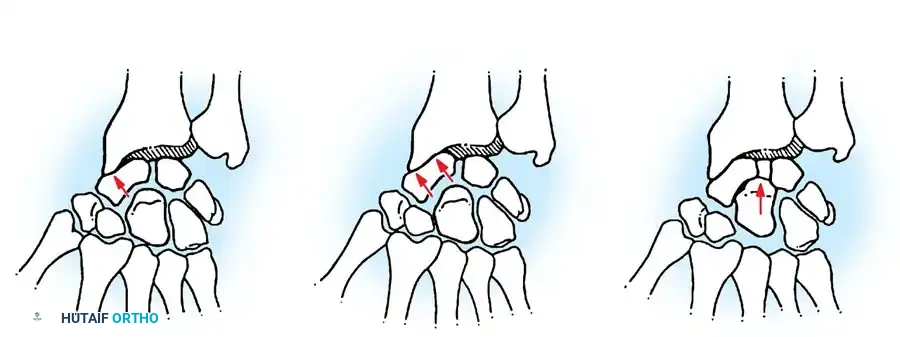
The scaphoid acts as the critical mechanical link between the proximal and distal carpal rows. When its integrity is compromised—either through ligamentous dissociation (scapholunate tear) or fracture nonunion—the carpus undergoes predictable, progressive degenerative changes. Procedures such as scaphocapitate arthrodesis, scaphocapitolunate arthrodesis, and lunotriquetral arthrodesis are designed to stabilize this complex intercalated segment, redistribute axial loads across the radiocarpal joint, and halt the progression of arthrosis.
Clinical Pearl: The success of any limited carpal arthrodesis hinges on the precise restoration of carpal alignment prior to fixation. Fusing the carpus in a malaligned position (e.g., excessive scaphoid flexion) will inevitably lead to restricted radiocarpal motion, impingement, and accelerated adjacent-segment degeneration.
BIOMECHANICAL PRINCIPLES AND INDICATIONS
Biomechanics of the Scaphocapitate Articulation
The scaphocapitate joint is central to midcarpal kinematics. During wrist deviation and flexion/extension, the scaphoid must rotate to accommodate the changing geometry of the radiocarpal and midcarpal spaces. Arthrodesis of the scaphoid to the capitate effectively locks the midcarpal joint, converting the scaphoid and capitate into a single functional unit. This transfers loads directly from the metacarpals through the capitate and scaphoid into the scaphoid fossa of the distal radius.
Indications for Surgery
- Midcarpal Instability: Chronic, symptomatic instability that has failed conservative management and soft-tissue reconstruction.
- Localized Osteoarthritis: Degenerative changes isolated to the scaphocapitate or scaphocapitolunate joints.
- Rotatory Subluxation of the Scaphoid: In cases where ligamentous reconstruction is no longer viable due to chronicity or fixed deformity.
- Spasticity or Paralytic Deformities: To provide a stable central column for the hand in neuromuscular disorders.
Contraindications
- Radioscaphoid Arthritis: If the articular cartilage of the scaphoid fossa of the distal radius is compromised, a scaphocapitate fusion will fail to relieve pain. In such cases, a proximal row carpectomy (PRC) or scaphoid excision with four-corner fusion is indicated.
- Active Infection: Absolute contraindication.
- Severe Osteopenia: May compromise hardware purchase and graft incorporation.
PREOPERATIVE EVALUATION
A meticulous preoperative evaluation is mandatory. Standard posteroanterior (PA), lateral, and scaphoid-view radiographs are required to assess the extent of arthrosis and measure carpal angles.
- Radioscaphoid Angle: Normal is 30 to 60 degrees. Restoration of this angle (targeting approximately 50 degrees) is critical during surgery.
- Capitolunate Angle: Normal is less than 15 degrees.
- Advanced Imaging: Computed Tomography (CT) is highly recommended to evaluate bone stock, confirm the exact location of arthritic changes, and plan the trajectory of internal fixation. Magnetic Resonance Imaging (MRI) may be utilized to assess the vascularity of the proximal scaphoid pole, particularly in SNAC wrists.
SCAPHOCAPITATE ARTHRODESIS (SENNWALD AND UFENAST TECHNIQUE)
The Sennwald and Ufenast technique for scaphocapitate arthrodesis is a robust procedure that utilizes a dorsal approach, meticulous joint decortication, and rigid lag screw fixation supplemented with a local corticocancellous bone graft.
Patient Positioning and Preparation
- Place the patient in the supine position with the operative arm extended on a radiolucent hand table.
- Apply a well-padded pneumatic tourniquet to the proximal arm.
- Following standard skin preparation and draping, exsanguinate the limb using an Esmarch bandage and inflate the tourniquet to the appropriate pressure (typically 250 mm Hg or 100 mm Hg above systolic blood pressure).
Surgical Approach and Exposure
- Make a straight dorsal longitudinal incision over the central aspect of the wrist, centered over Lister's tubercle and extending distally over the capitate.
- Carefully dissect through the subcutaneous tissues, identifying and protecting the dorsal sensory branches of the radial nerve and the dorsal branch of the ulnar nerve.
- Incise and reflect the extensor retinaculum. Typically, the retinaculum is opened over the third extensor compartment.
- Transpose the extensor pollicis longus (EPL) tendon radially.
- Retract the tendons of the fourth extensor compartment (extensor digitorum communis and extensor indicis proprius) ulnarly to expose the dorsal wrist capsule.
- Make a longitudinal incision in the dorsal wrist capsule. Dissect distally and radially, elevating the capsule as full-thickness flaps to clearly identify the scaphocapitate joint.
Joint Preparation
- Inspect the scaphocapitate articulation.
- Using a combination of a sharp awl, osteotomes, and a rongeur, meticulously remove all articular cartilage between the scaphoid and the capitate.
- It is imperative to decorticate down to healthy, bleeding subchondral bone to maximize the osteogenic potential of the fusion site.
Surgical Warning: Do not over-resect the subchondral bone, as this will alter the anatomical dimensions of the carpus and make rigid screw fixation difficult. Preserve the overall architecture of the joint space.
Bone Graft Harvesting
- A corticocancellous bone graft is required to fill the prepared scaphocapitate interval.
- Mobilize the proximal skin flap to allow exposure of the dorsoradial aspect of the distal radius metaphysis.
- Identify the interval between the first extensor compartment (abductor pollicis longus and extensor pollicis brevis) and the second extensor compartment (extensor carpi radialis longus and brevis).
- Using a sharp osteotome or an oscillating saw, harvest a suitably sized corticocancellous bone block from the distal radius.
- Pack the donor site with bone wax or allograft if necessary to minimize postoperative bleeding.
Graft Placement and Fixation
- Place the harvested corticocancellous bone graft directly into the decorticated space between the scaphoid and the capitate.
- Reduce the scaphoid onto the capitate. Crucial Step: Ensure the scaphoid is not fused in a flexed position. Use fluoroscopy to confirm that the radioscaphoid angle is restored to approximately 50 degrees.
- Provisionally hold the reduction with 0.045-inch Kirschner wires.
- Use two headless compression screws or standard lag screws to secure the scaphocapitate arthrodesis. The trajectory should typically run from the distal pole of the scaphoid into the body of the capitate, ensuring maximum thread purchase.
- Obtain multi-planar intraoperative radiographs to ascertain satisfactory bone alignment, graft position, and screw placement. Ensure no hardware penetrates the radiocarpal or capitolunate joints.
Closure
- Irrigate the wound copiously with sterile saline.
- Close the dorsal capsule meticulously with interrupted absorbable sutures (e.g., 3-0 Vicryl) to prevent extensor tendon bowstringing and provide a smooth gliding surface.
- Repair the extensor retinaculum, leaving the EPL tendon transposed subcutaneously to prevent attrition rupture.
- Close the skin with non-absorbable monofilament sutures.
Postoperative Care Protocol
- Immediate Post-op: Apply a sterile, nonadherent dressing and a bulky short-arm plaster splint or cast. Elevate the limb strictly for the first 48-72 hours to minimize edema.
- 2 Weeks: The initial cast and skin sutures are removed. A new, well-molded short-arm cast is applied.
- 2 to 10 Weeks: The short-arm cast is worn continuously for an additional 8 weeks (total 10 weeks of rigid immobilization).
- 10 to 12 Weeks: After cast removal, clinical and radiographic evaluation of union is performed. A removable protective thermoplastic splint is fabricated and worn for another 2 weeks, particularly during strenuous activities.
- Rehabilitation: A graduated exercise program is begun under the guidance of a certified hand therapist, focusing on restoring digital range of motion, radiocarpal motion, and grip strength.
SCAPHOCAPITOLUNATE ARTHRODESIS (ROTMAN ET AL. TECHNIQUE)
When degenerative changes or instability extend to involve the lunate, a scaphocapitolunate (SCL) arthrodesis is indicated. This procedure stabilizes the entire proximal carpal row to the capitate, effectively treating complex midcarpal instability patterns.
Patient Positioning and Exposure
- With the patient supine and the hand secured on the hand table, inflate the tourniquet after elastic wrap limb exsanguination.
- Make an oblique dorsal wrist incision, extending from the ulnar aspect of the distal radius, angling distally and radially toward the distal pole of the scaphoid.
- Develop the subcutaneous flaps, protecting the dorsal sensory nerve branches.
- Expose the wrist capsule by developing the interval between the third (EPL) and fourth (EDC) extensor compartments.
- Open the wrist capsule with an inverted T-shaped incision. The transverse limb of the "T" runs parallel to the dorsal rim of the radius, and the longitudinal limb extends distally over the capitate.
Articular Preparation
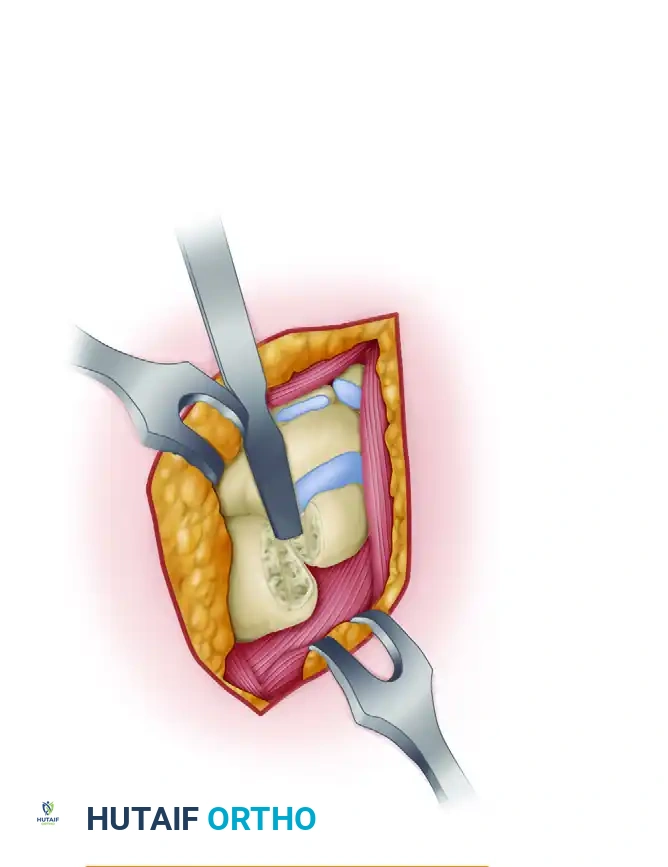
- Reflect the capsular flaps to expose the adjoining articular surfaces of the scaphoid, capitate, and lunate.
The complex articular anatomy of the carpus is exposed, highlighting the scaphoid, capitate, and lunate interfaces that require preparation.
- Using a combination of fine rongeurs, sharp curets, and a high-speed burr, meticulously remove the articular cartilage and subchondral bone from the adjoining articular surfaces of the scaphoid, capitate, and lunate.
Decortication of the midcarpal joint spaces using an osteotome and curet. It is vital to reach bleeding cancellous bone while preserving the structural geometry of the carpal bones.
- Preserve Architecture: It is critical to preserve the overall architecture and volumetric dimensions of the articular spaces. Excessive bone resection will lead to carpal collapse and loss of the normal carpal arch.
Bone Grafting and Fixation
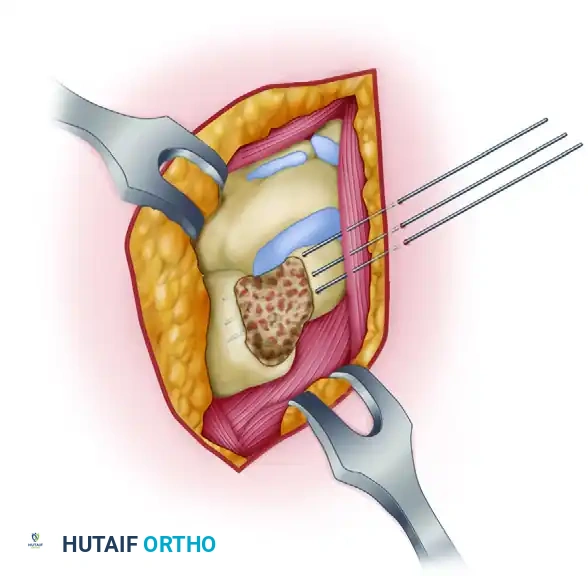
- Harvest copious amounts of cancellous bone graft. Depending on the volume required, this can be taken from the distal radius metaphysis (via a separate cortical window) or from the iliac crest if a larger volume of highly osteogenic graft is needed.

Rich, autologous cancellous bone graft harvested and prepared for packing into the decorticated carpal intervals.
- Firmly pack the cancellous bone graft into the prepared spaces between the scaphoid, capitate, and lunate.
- Reduce the carpal bones into their anatomic alignment. Correct any dorsal intercalated segment instability (DISI) or volar intercalated segment instability (VISI) deformity of the lunate prior to fixation.
- Secure the arthrodesis using multiple 0.045-inch or 0.062-inch Kirschner wires.
Insertion of Kirschner wires across the prepared carpal joints to provide rigid provisional and definitive stabilization.
- The K-wires should be driven across the scaphocapitate and capitolunate intervals. Ensure the wires are buried beneath the articular surface of the radiocarpal joint to prevent cartilage scoring during postoperative mobilization.
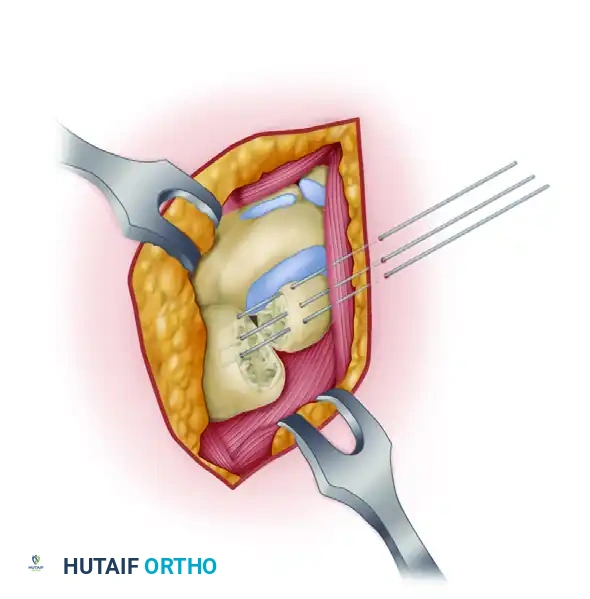
Final construct demonstrating K-wire fixation with the cancellous bone graft densely packed into the SCL intervals, ensuring a stable, osteogenic environment for fusion.
- Confirm the reduction, hardware placement, and carpal angles with intraoperative fluoroscopy.
- Close the capsule, retinaculum, and skin in layers as described previously. Postoperative care mirrors that of the scaphocapitate arthrodesis, though K-wires may require removal at 8 to 10 weeks once radiographic union is confirmed.
LUNOTRIQUETRAL ARTHRODESIS
Lunotriquetral (LT) arthrodesis is specifically indicated for chronic, symptomatic lunotriquetral instability (often presenting with a VISI deformity) or isolated LT osteoarthritis that has failed conservative management and soft-tissue repair.
Surgical Technique
The procedure is typically performed through a dorsal approach, utilizing the interval between the fourth and fifth extensor compartments to access the ulnar aspect of the midcarpal joint.
-
A. Decortication of the Joint: Following capsulotomy, the lunotriquetral joint is identified. Using a fine osteotome, burr, or curet, perform a thorough decortication of both the lunate and triquetral articular surfaces. All cartilage must be removed down to bleeding subchondral bone. Care must be taken not to violate the proximal articular surfaces that interface with the radius and triangular fibrocartilage complex (TFCC).
-
B. Kirschner Wire Fixation: The lunate and triquetrum are reduced. If a VISI deformity is present, the lunate must be extended and the triquetrum flexed to restore the normal collinear relationship. Once reduced, the joint is stabilized using parallel or crossed Kirschner wires driven from the ulnar aspect of the triquetrum into the lunate. Compression screws may also be utilized if bone stock permits.
-
C. Bone Grafting: The decorticated lunotriquetral space is densely packed with autologous cancellous bone graft, typically harvested from the distal radius. The graft acts as an osteoconductive scaffold and provides osteoinductive factors to ensure a solid arthrodesis.
Pitfall: Failure to correct a VISI deformity prior to LT fixation will result in a malaligned carpus, leading to persistent pain, altered radiocarpal kinematics, and a high risk of nonunion. Always verify the capitolunate angle fluoroscopically before final fixation.
COMPLICATIONS AND MANAGEMENT
While limited intercarpal arthrodesis is highly effective, surgeons must be prepared to manage potential complications:
- Nonunion: The most common complication, particularly in SCL and LT fusions, due to the small surface area of the joints and complex multi-planar forces. Management requires revision arthrodesis with robust iliac crest bone grafting and rigid revision fixation (often upgrading from K-wires to compression screws or specialized carpal fusion plates).
- Hardware Prominence or Migration: K-wires may migrate or cause soft-tissue irritation. Headless compression screws reduce this risk but must be countersunk appropriately. Symptomatic hardware should be removed only after solid radiographic union is achieved.
- Carpal Malalignment: Fusing the scaphoid in excessive flexion restricts wrist extension and radial deviation. Prevention through meticulous intraoperative fluoroscopic assessment is paramount.
- Adjacent Segment Disease: Altered kinematics can lead to accelerated radiocarpal arthrosis over time. Patients should be counseled preoperatively that limited fusions are salvage procedures, and future interventions (such as total wrist arthrodesis) may eventually be required.
By adhering to strict biomechanical principles, executing meticulous joint preparation, and ensuring rigid fixation with adequate bone grafting, orthopedic surgeons can achieve high rates of successful union and significant functional improvement in patients undergoing limited intercarpal arthrodesis.
You Might Also Like