Mastering Hand and Wrist Reconstruction: Pollicization and Macrodactyly Management

Key Takeaway
Hand and wrist reconstruction for complex congenital anomalies, such as macrodactyly and thumb hypoplasia, requires meticulous surgical planning. This guide details the step-by-step execution of pollicization, including neurovascular preservation and metacarpal rotation, alongside staged debulking and digital shortening techniques for macrodactyly. Emphasizing biomechanical restoration and soft tissue management, these advanced operative strategies aim to optimize both aesthetic appearance and functional outcomes in pediatric and adult patients.
RECONSTRUCTION OF THE HAND AND WRIST: ADVANCED CONGENITAL ANOMALIES
Reconstructive surgery of the hand and wrist for complex congenital anomalies demands a profound understanding of biomechanics, neurovascular anatomy, and spatial geometry. Among the most challenging procedures in this domain are pollicization—the creation of a functional thumb from an existing digit—and the surgical management of macrodactyly, a rare and often progressive overgrowth disorder.
The primary goal of these interventions is to restore prehension, optimize aesthetic appearance, and prevent secondary deformities such as carpal tunnel syndrome or severe angular contractures. This masterclass delineates the evidence-based surgical techniques, preoperative planning, and postoperative protocols required to execute these procedures with precision.
POLLICIZATION OF THE DIGIT
Pollicization is the gold standard for reconstructing a severely hypoplastic or absent thumb (Blauth Types IIIB, IV, and V). The procedure involves the transposition of a functional digit (most commonly the index finger) to the thumb position on a neurovascular pedicle. The success of this operation hinges on the meticulous preservation of the neurovascular bundles, precise skeletal shortening, and the rebalancing of the intrinsic and extrinsic musculature to replicate the complex kinematics of the trapeziometacarpal joint.
Preoperative Planning and Incision Design
Before the inflation of the tourniquet, the surgeon must carefully plan the incisions. The design must allow for the pollicization of the most functional digit, the fillet-type amputation of any excessive or non-functional digits, and the wide exposure of the neurovascular bundles supplying the chosen digit.
🔪 Surgical Pearl: Incision Architecture
The incision must be designed to create a generous first web space while avoiding linear scars that cross the new web space, which could lead to adduction contractures. A combination of palmar and dorsal rotational flaps is typically employed to ensure tension-free closure and adequate skin coverage over the transposed metacarpal.
Surgical Technique: Pollicization (Technique 79-30)
Step 1: Exsanguination and Tourniquet Application
After the incisions and skin flaps have been meticulously designed and marked with a surgical pen, exsanguinate the limb using an Esmarch bandage and inflate the pneumatic tourniquet to the appropriate pediatric or adult pressure.
Step 2: Neurovascular Dissection
Make the planned incisions through the dermis and carefully dissect the common neurovascular bundles to the middle digit in each web space.
- Identify the bifurcation of the common digital artery.
- Ligate and divide the proper digital artery to the adjacent (non-pollicized) digit to mobilize the neurovascular pedicle fully.
- Carefully dissect the common digital nerves proximally to the thenar level before any division.
- Critical Step: Meticulously preserve the proper digital nerves and the dorsal venous drainage system to the pollicized digit. Venous congestion is a primary cause of flap and digit failure.
Step 3: Tendon Dissection and Management of Extra Digits
Dissect out the extrinsic flexor and extensor tendons to the pollicized digit. If there are bifurcations or anomalous interconnections (juncturae tendinum) of these tendons, divide the abnormal insertions to the neighboring tendons to ensure independent excursion.
- Amputate any extra or non-functional digits, including their corresponding metacarpal and articulating carpal bones.
- Preserve the extensor tendons to the excised digits, if present. These can be utilized later as tendon transfers to reinforce finger extension or augment thumb abduction.
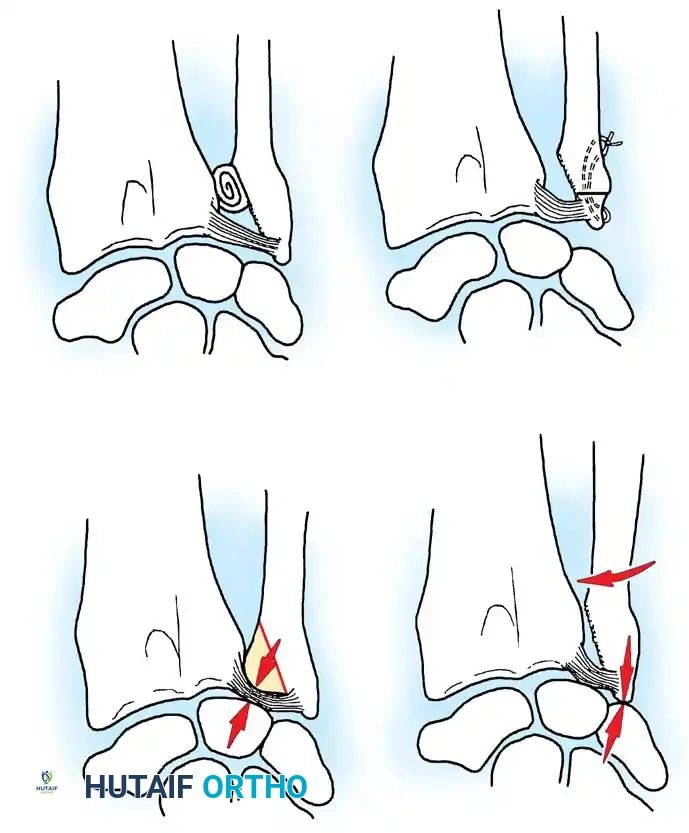
Step 4: Skeletal Shortening and Repositioning
The index finger is naturally longer than the thumb and possesses an extra phalanx. To mimic normal thumb anatomy, the metacarpal must be shortened, and the metacarpophalangeal (MCP) joint must be converted into the new carpometacarpal (CMC) joint.
- Shorten the metacarpal of the pollicized digit by performing a transverse or step-cut osteotomy just proximal to the metacarpal neck.
- Discard the remaining proximal metacarpal shaft.
- Biomechanical Rotation: Rotate the head of the metacarpal into 120 degrees of flexion and 90 degrees of pronation. This specific spatial orientation is paramount; it places the new thumb in a position of palmar abduction and opposition, allowing the pulp to face the remaining digits.
- Secure the metacarpal head in this precise position using two intraosseous sutures or a smooth Kirschner wire (K-wire). This allows for appropriate shortening and rigid stabilization.
Step 5: Intrinsic Muscle Transfer and Web Space Reconstruction
To provide dynamic stability and active motion to the new thumb, the intrinsic muscles must be reattached to the extensor mechanism.
- Suture the intrinsic muscles (the palmar and dorsal interossei of the transposed digit) to the lateral bands of the extensor mechanism of the pollicized digit. This augments adduction and abduction, simulating the function of the adductor pollicis and abductor pollicis brevis.
- Use the fillet flaps harvested from the deleted digits to reconstruct a deep, wide first web space.
- Remove any excess skin to allow appropriate, tension-free closure of the shortened, pollicized digit.
Step 6: Extrinsic Tendon Transfer (If Required)
If increased extension of the wrist or augmentation of the new thumb is needed:
- Divide the flexor digitorum sublimis (FDS) muscle at the level of the A1 pulley of the pollicized digit.
- Transfer it to the dorsal base of the second metacarpal to act as a wrist extensor, or route it to augment thumb kinematics depending on the specific preoperative deficit.
Step 7: Tourniquet Deflation and Closure
Deflate the tourniquet prior to final skin closure. Obtain meticulous hemostasis and verify the capillary refill and viability of the remaining digits and transposed flaps.
Postoperative Care and Rehabilitation
Apply a bulky, non-compressive dressing reinforced with a long-arm posterior splint.
- Positioning: The elbow is supported at 90 degrees of flexion, the wrist at neutral or in slight extension, and the new thumb in a fully abducted and opposed position.
- Duration: The rigid splint is worn continuously for 3 weeks. It may be carefully changed in the clinic for suture removal and wound inspection, ensuring the digit is not inadvertently displaced.
- Rehabilitation: After splint removal at 3 weeks, a targeted occupational therapy exercise program is initiated to encourage cortical plasticity and motor relearning. A removable thermoplastic night splint is used to hold the thumb in the opposed position for an additional 3 months to prevent adduction contractures.
MACRODACTYLY: PATHOLOGY AND CLINICAL PRESENTATION
Macrodactyly is a rare, complex congenital anomaly characterized by the disproportionate overgrowth of the soft tissue, bone, and neurovascular elements of one or more digits. It is frequently associated with somatic mutations in the PIK3CA gene, placing it within the PROS (PIK3CA-Related Overgrowth Spectrum) family of disorders.
It is generally believed that all the tissues of the involved finger are enlarged; however, some authors have noted the relative sparing of the tendons and blood vessels. The nerves that innervate the involved territory (most commonly the median nerve distribution) are characteristically and pathologically enlarged, often presenting as fibrolipomatous hamartomas. In a rare variant of macrodactyly (hyperostotic), there may be osteocartilaginous deposits around the joints; a traumatic etiology for this specific condition has been reported in the literature.
Static vs. Progressive Macrodactyly
- Static Macrodactyly: The deformity is present in infancy. There is usually diffuse enlargement of the digit; however, the distal and palmar tissues typically appear more enlarged than the dorsal and proximal tissues. The finger grows, but it grows in proportion to normal digital growth.
- Progressive Macrodactyly: This form occurs in early childhood as a rapidly and aggressively enlarging digit. It frequently presents with an angular deformity that makes the finger "banana-shaped." The skin may become thickened, and the nails are often hypertrophied.
FIGURE 79-59 A: Recurrent progressive macrodactyly in a 6-year-old child, presenting 2 years after an initial debulking procedure of the ring finger and amputation of the long finger. Note the severe angular deformity and soft tissue hypertrophy.
The phalanges are invariably involved, and the metacarpals may also be enlarged. With skeletal maturity, the enlarged digit begins to lose range of motion due to joint incongruity and massive soft tissue impedance. Later in life, symptoms of carpal tunnel syndrome may develop due to the massive proliferation of the median nerve within the unyielding carpal canal, leading to complaints of paresthesias, hypesthesias, and causalgia. Trophic ulcers may also develop over the involved digit due to altered sensation and abnormal mechanics.
Involvement is usually unilateral, and multiple digits are affected two to three times as often as single digits. If the thumb is involved, a characteristic abduction and hyperextension deformity results. Syndactyly is present in approximately 10% of patients. Furthermore, macrodactyly involving both the hands and the feet has been reported, and some patients with neurofibromatosis type 1 (NF1) may develop phenotypically similar macrodactyly.
SURGICAL MANAGEMENT OF MACRODACTYLY
Indications for Surgery
There are no satisfactory nonsurgical methods for controlling macrodactyly. Attempts to compress the digit with elastic wrapping or pressure garments have been universally unsuccessful and may induce ischemia.
Indications for surgical intervention include:
1. Progressive cosmetic and functional enlargement.
2. Severe angular deviation interfering with adjacent digits.
3. Compressive neuropathies (e.g., carpal tunnel syndrome).
4. Causalgia or intractable pain.
Soft Tissue Debulking Procedures
For a progressively enlarging digit, a staged excisional debulking procedure is usually required.
🚨 Surgical Warning: Staged Interventions
Never attempt to debulk both the radial and ulnar sides of a digit simultaneously. Doing so severely compromises the vascular supply and will almost certainly result in catastrophic flap necrosis and digital loss.
The Staged Approach:
As much excess fibro-fatty tissue as possible is excised from one half (e.g., the radial side) of the digit. The skin flaps must be handled with extreme care, preserving the subdermal plexus. Three months later, after adequate revascularization across the midline has occurred, the other half (the ulnar side) is debulked. This procedure may be required several times during the child's growth period.
Nerve Management During Debulking:
Tsuge proposed that the disproportionate growth is a direct result of excessive neural input. He recommended that the enlarged digital nerves be stripped of one-half of their fascicles at the time of debulking.
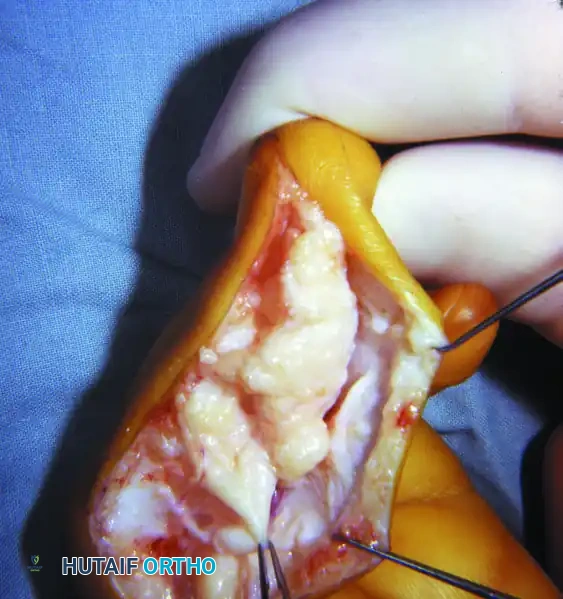
FIGURE 79-59 B: Intraoperative photograph demonstrating the massive, pathologically enlarged digital nerve (fibrolipomatous hamartoma) characteristic of macrodactyly.
Tsuge also recommended the complete excision of the enlarged digital nerves during debulking as the most effective way to control progressive macrodactyly, arguing that this causes only minimal functional neural impairment in young children due to overlapping sensory territories and neuroplasticity. Alternatively, Kelikian recommended the segmental resection of the tortuous, elongated digital nerves followed by end-to-end epineural repair to reduce the neural volume while attempting to preserve continuity.

FIGURE 79-59 C: Wound closure after extensive soft tissue and neural debulking. Note the redundant skin has been excised to contour the digit.
Skeletal Management: Physeal Arrest and Shortening
To address the longitudinal overgrowth, skeletal procedures are mandatory.
Physeal Arrest:
Once the affected digit has reached the estimated adult length of the corresponding normal digit (often determined by comparing it to the parent's hand), physeal arrest is frequently recommended. This can be achieved by:
- Drilling holes through the physes to destroy the growth plate.
- Formal resection of the physes.
- Epiphysiodesis of all involved phalanges.
Digital Shortening and Osteotomies:
In the angulated finger, closing wedge osteotomies through the proximal or middle phalanx are necessary to correct the deviation. Tan et al. performed complete middle phalangectomy in patients with severe macrodactyly as their preferred surgical option to achieve both shortening and joint reduction. Millesi described a highly complex technique for shortening the enlarged thumb, in which parts of the distal and middle phalanges are removed while preserving the distal interphalangeal joint.
Amputation (ray resection) is used to provide relief only as a last resort in an adult with a severe, non-functional, and bothersome deformity that has failed multiple reconstructive attempts.
Tsuge's Digital Shortening Technique (Technique 79-31)
Tsuge described an elegant method for digital shortening that preserves the nail complex while significantly reducing the length of the digit by telescoping the distal phalanx onto the middle phalanx.
Step 1: Bone Resection
Matching sections of bone are removed to allow for overlapping. Specifically, the volar (palmar) half of the distal phalanx and the dorsal half of the middle phalanx are resected using an oscillating saw.
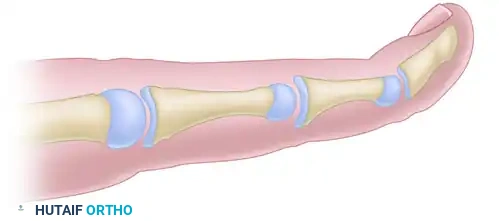
FIGURE 79-60 A: Digital shortening for macrodactyly (Tsuge). Matching sections (shaded areas) of the volar half of the distal phalanx and the dorsal half of the middle phalanx are marked for removal.
Step 2: Skeletal Reduction
The remaining dorsal half of the distal phalanx (carrying the nail bed) is reduced and telescoped onto the remaining volar half of the middle phalanx. This preserves the dorsal skin bridge and the germinal matrix of the nail. Excess volar soft tissue is excised.
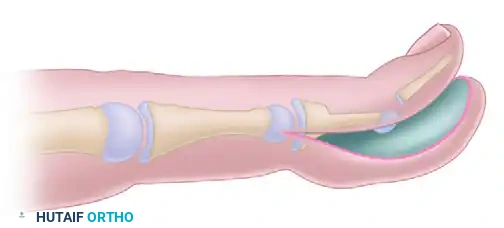
FIGURE 79-60 B: The distal phalanx is reduced onto the middle phalanx. The dorsal skin bridge is meticulously preserved, while the excess volar soft tissue is removed to match the new skeletal length.
Step 3: Fixation and Closure
The bone is stabilized with longitudinal K-wires. Soft tissue closure is completed. The surgeon must accept some excess dorsal soft tissue initially, which will remodel over time or can be addressed in a subsequent minor revision.
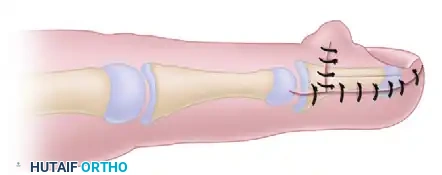
FIGURE 79-60 C: Soft tissue closure is completed. The digit is significantly shortened while preserving the aesthetic appearance of the nail complex.
Complications and Pitfalls in Macrodactyly Surgery
The most common complication in the treatment of macrodactyly is recurrence, which is almost expected after simple soft tissue debulking, particularly in the progressive variant. Parents must be counseled preoperatively that multiple surgeries will be required throughout the child's growth.
Flap necrosis is a major, devastating surgical complication. The hypertrophic skin often has an abnormal subdermal vascular network. Some authors have recommended the complete excision of the overlying abnormal skin and its replacement with a full-thickness skin graft to avoid the problem of ischemic necrosis entirely.
Careful attention to flap design, avoiding acute angles, and strictly adhering to the principle of operating on only one side of the finger at a time will minimize the risk of circulatory disturbance and optimize the chances of a successful reconstructive outcome.
📚 Medical References
- hand reconstruction, J Hand Surg 2:387, 1977.
- Morrison WA, O’Brien BM, MacLeod AM: Thumb reconstruction with a free neurovascular wrap-around fl ap from the big toe, J Hand Surg 5:575, 1980.
- Murray JF, Carman W, MacKenzie JK: Transmetacarpal amputation of the index fi nger: a clinical assessment of hand strength and complications, J Hand Surg 2:471, 1977.
- Nuzumlali E, Orhun E, Ozturk K, et al: Results of ray resection and amputation for ring avulsion injuries at the proximal interphalangeal joint, J Hand Surg 28:578, 2003.
- Omokawa S, Yajima H, Inada Y, et al: A reverse ulnar hypothenar fl ap for fi nger reconstruction, Plast Reconstr Surg 106:828, 2000.
- Peacock EE Jr: Metacarpal transfer following amputation of a central digit, Plast Reconstr Surg 29:345, 1962.
- Peimer CA, Wheeler DR, Barrett A, et al: Hand function following single ray amputation, J Hand Surg 24A:1245, 1999.
- Posner MA: Ray transposition for central digital loss, J Hand Surg 4:242, 1979.
- Riordan DC: Personal communication, 1969.
- Rose EH, Buncke HJ: Simultaneous transfer of the right and left second toes for reconstruction of amputated index and middle fi ngers in the same hand: case report, J Hand Surg 5:590, 1980.
- Rose EH, Norris NS, Kowalski TA, et al: The “cap” technique: nonmicrosurgical reattachment of fi ngertip amputations, J Hand Surg 14A:513, 1989.
- Rybka FJ, Pratt FE: Thumb reconstruction with a sensory fl ap from the dorsum of the index fi nger, Plast Reconstr Surg 64:141, 1979.
- Schlenker JD, Kleinert HE, Tsai T-M: Methods and results of replantation following traumatic amputation of the thumb in sixty-four patients, J Hand Surg 5:63, 1980.
- Shibu MM, Tarabe MA, Graham K, et al: Fingertip reconstruction with a dorsal island homodigital fl ap, Br J Plast Surg 50:121, 1997.
- Snowdy HA, Omer GE Jr, Sherman FC: Longitudinal growth of a free toe phalanx transplant to a fi nger, J Hand Surg 5:71, 1980.
- Stern PJ, Lister GD: Pollicization after traumatic amputation of the thumb, Clin Orthop Relat Res 155:85, 1981.
- Swanson AB: Restoration of hand function by the use of partial or total prosthetic replacement: I. the use of partial prostheses, J Bone Joint Surg 45A:276, 1963.
- Swanson AB: The Krukenberg procedure in the juvenile amputee, J Bone Joint Surg 46A:1540, 1964.
- Swanson AB, Boeve NR, Lumsden RM: The prevention and treatment of amputation neuromata by silicone capping, J Hand Surg 2:70, 1977.
- Tegtmeier RE: Thumb-to-thumb transfer following severe
You Might Also Like