Radial Shortening and DRUJ Reconstruction: A Comprehensive Surgical Guide
Key Takeaway
Radial shortening osteotomy is a powerful surgical intervention for addressing ulnar-minus variance and associated distal radioulnar joint (DRUJ) incongruities. This comprehensive guide details the precise biomechanical principles, step-by-step volar surgical approach, and rigid internal fixation techniques required for successful outcomes. Furthermore, it explores the intricate anatomy of the triangular fibrocartilage complex (TFCC), diagnostic modalities, and arthroscopic evaluation methods essential for managing concurrent ulnocarpal instability and traumatic lesions.
INTRODUCTION TO DISTAL RADIOULNAR AND ULNOCARPAL JOINT INJURIES
The ulnar aspect of the wrist is a highly complex anatomical region, often referred to as the "black box" of the wrist due to its intricate ligamentous, cartilaginous, and osseous interplay. Pathologies in this region frequently manifest as debilitating ulnar-sided wrist pain, mechanical instability, and progressive degenerative changes. The primary structures responsible for stability and load transfer include the distal radioulnar joint (DRUJ), the ulnocarpal joint, and the triangular fibrocartilage complex (TFCC).
Surgical interventions in this region, such as radial shortening osteotomy, are biomechanically designed to alter load distribution across the radiocarpal and ulnocarpal joints. Radial shortening is particularly indicated in cases of symptomatic ulnar-minus variance (such as Kienböck's disease) to decompress the lunate and level the distal radioulnar articulation.
Biomechanics and Functional Anatomy of the DRUJ and TFCC
The TFCC, as classically described by Werner and Palmer, is the primary stabilizer of the DRUJ and the ulnar carpus. It is a multifaceted structure comprising:
* The Articular Disc (Fibrocartilage proper): Central avascular region that absorbs compressive forces.
* Dorsal and Volar Radioulnar Ligaments: The primary stabilizers of the DRUJ during forearm rotation.
* Ulnar Collateral Ligament (UCL) and Meniscal Homologue.
* Extensor Carpi Ulnaris (ECU) Subsheath.
The TFCC originates on the ulnar margin of the lunate fossa of the radius and inserts ulnarward into the fovea at the base of the ulnar styloid, as well as the ulnar head. Distally, it extends to the triquetrum, hamate, and the base of the fifth metacarpal.
Clinical Pearl: The articular surface contact within the shallow sigmoid notch of the radius accounts for only about 20% of DRUJ stability. The remaining 80% of stability is entirely dependent on the integrity of the soft tissues, primarily the TFCC and the dynamic stabilization of the ECU.
During normal forearm rotation, the kinematics of the DRUJ are complex. The ulnar head articulates with the sigmoid notch, translating from a dorsal and distal position in full pronation to a proximal and palmar position in full supination. Furthermore, biomechanical cadaveric studies by Palmer et al. demonstrated that axial loads applied to the wrist are distributed approximately 80% to the distal radius and 20% to the ulna. Alterations in ulnar variance—whether congenital or acquired post-trauma—drastically shift this load distribution, predisposing the joint to impaction syndromes or avascular necrosis of the carpal bones.
DIAGNOSTIC EVALUATION OF ULNAR-SIDED WRIST PAIN
Accurate localization of ulnar-sided wrist pain is paramount. The differential diagnosis includes TFCC tears, DRUJ instability, ulnocarpal abutment, lunotriquetral instability, and ECU tendinopathy.
Clinical Examination and Provocative Testing
Patients with TFCC injuries typically present following a traumatic event, such as a fall on an extended, pronated wrist, or repetitive axial loading (common in gymnasts and racquet sport athletes). Symptoms include ulnar-sided pain, mechanical clicking, and subjective weakness in grip strength.
Key provocative tests include:
* Ulnar Impaction Test: Hyperextension and ulnar deviation of the wrist combined with axial compression. Elicitation of pain indicates ulnocarpal abutment or a TFCC lesion.
* The Press Test: The patient attempts to lift their body weight off a chair using the affected wrist in an extended position. This creates a significant axial ulnar load. A positive test is highly sensitive for TFCC pathology.
* Piano Key Test: With the wrist in pronation, the examiner applies dorsal-to-palmar pressure on the ulnar head. Excessive translation compared to the contralateral side indicates DRUJ instability.
* Fovea Sign: Point tenderness directly in the soft spot between the ulnar styloid and the FCU tendon indicates a disruption of the foveal attachment of the TFCC.
* Shuck Test: Stabilizing the radius while applying anteroposterior shear stress to the ulna to assess DRUJ laxity.
Radiographic and Advanced Imaging Modalities
Standard radiographic evaluation must include a "zero-variance" posteroanterior (PA) view.
Radiographic Technique: To accurately assess radioulnar variance, the PA radiograph must be taken with the shoulder abducted to 90 degrees, the elbow flexed to 90 degrees, and the forearm and hand resting flat on the cassette in neutral rotation. Pronation artificially increases ulnar-plus variance, while supination decreases it.
While plain radiographs may reveal ulnar variance, sigmoid notch fractures, or ulnar styloid avulsions, advanced imaging is often required:
* Magnetic Resonance Imaging (MRI): High-resolution MRI (often with an intra-articular contrast arthrogram) approaches 100% sensitivity and specificity for detecting central TFCC tears, though peripheral tears may still be obscured.
* Computed Tomography (CT): Essential for evaluating the osseous architecture of the sigmoid notch, assessing malunions of the distal radius, and quantifying DRUJ subluxation in varying degrees of rotation.
ARTHROSCOPIC EVALUATION OF THE TFCC
Wrist arthroscopy remains the gold standard for the definitive diagnosis and concurrent management of TFCC lesions and DRUJ instability. It allows direct visualization of the articular disc, the radiocarpal ligaments, and the chondral surfaces of the lunate and triquetrum.
The Trampoline and Hook Tests
Arthroscopic evaluation utilizes standard radiocarpal portals, primarily the 3-4 portal for viewing and the 6R (or 4-5) portal for instrumentation.
1. The Trampoline Test:
A blunt probe is introduced through the 6R portal and used to apply a compressive load to the center of the articular disc. A normal, intact TFCC will exhibit a resilient, trampoline-like bounce. A loss of this tension indicates a peripheral tear or foveal avulsion.

Arthroscopic view demonstrating the Trampoline Test. The probe applies a compressive load to assess the resilience of the TFCC.
2. The Hook Test:
The probe is inserted into the prestyloid recess to engage the ulnar periphery of the TFCC. The surgeon attempts to pull the complex radially and proximally. If the TFCC can be displaced toward the center of the radiocarpal joint, it signifies a loss of its proximal foveal attachment.

Initial engagement of the probe during the Hook Test in the prestyloid recess.
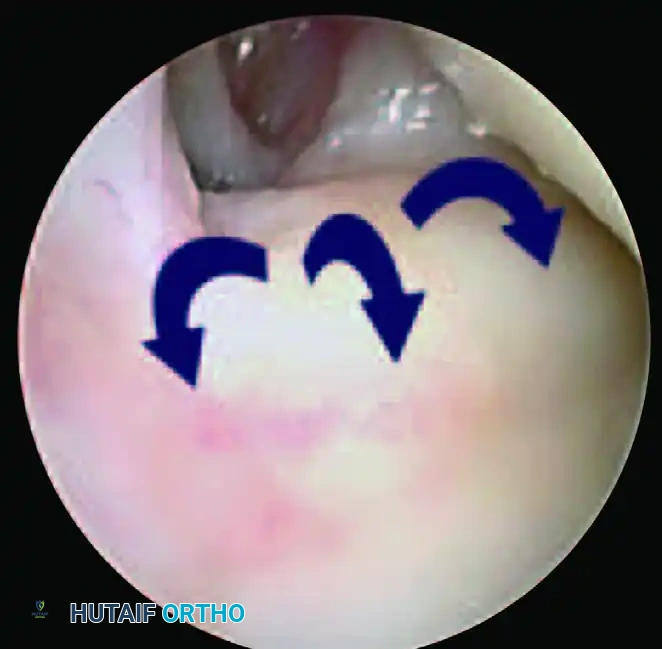
Positive Hook Test demonstrating abnormal displacement and laxity of the TFCC, confirming a peripheral tear.
According to the Atzei and Luchetti classification, an isolated distal TFCC tear will yield a positive trampoline test but a negative hook test. Conversely, complete or proximal foveal tears will render both tests positive, necessitating foveal reattachment.
Palmer Classification of TFCC Lesions
The Palmer classification divides TFCC abnormalities into traumatic and degenerative categories, guiding the surgical decision-making process.
Class 1: Traumatic Lesions
* 1A: Central perforation (avascular zone; treated with arthroscopic debridement).
* 1B: Ulnar avulsion (with or without ulnar styloid fracture; requires repair to the fovea).
* 1C: Distal avulsion (involving ulnocarpal ligaments).
* 1D: Radial avulsion (with or without sigmoid notch fracture; requires repair to the radius).
Class 2: Degenerative Lesions (Ulnocarpal Abutment Syndrome)
* 2A: TFCC wear without perforation.
* 2B: TFCC wear with lunate and/or ulnar chondromalacia.
* 2C: TFCC perforation with chondromalacia.
* 2D: TFCC perforation, chondromalacia, and lunotriquetral ligament perforation.
* 2E: All of the above with advanced ulnocarpal arthritis.
RADIAL SHORTENING OSTEOTOMY: SURGICAL TECHNIQUE
While ulnar shortening is utilized for ulnar-plus variance, Radial Shortening Osteotomy is a powerful procedure indicated primarily for symptomatic ulnar-minus variance (e.g., early-stage Kienböck's disease) to decompress the lunate by leveling the radiocarpal joint. It is also utilized to correct specific DRUJ incongruities where lengthening the ulna is contraindicated.
Preoperative Planning and Indications
Meticulous preoperative planning is required. The exact amount of shortening (typically 2 to 3 mm) is calculated from the zero-variance PA radiograph. The goal is to achieve neutral variance, thereby redistributing the axial load away from the radiolunate articulation and transferring it to the ulnocarpal joint.
Patient Positioning and Anesthesia
- The patient is placed in the supine position on the operating table with the affected arm extended on a radiolucent hand table.
- Regional anesthesia (brachial plexus block) or general anesthesia is administered.
- A well-padded pneumatic tourniquet is applied to the proximal arm.
- The limb is exsanguinated using an Esmarch bandage, and the tourniquet is inflated to the appropriate pressure (typically 250 mm Hg).
Step-by-Step Surgical Approach
The procedure utilizes a modified volar Henry approach to the distal radius.
- Incision: Make a longitudinal incision on the palmar aspect of the distal forearm, extending distally to the wrist flexion crease, overlying the flexor carpi radialis (FCR) tendon.
- Superficial Dissection: Incise the superficial fascia and the superficial sheath of the FCR. Retract the FCR tendon radiolaterally to protect the palmar cutaneous branch of the median nerve.
- Protecting the Radial Artery:
> Surgical Warning: The radial artery lies immediately radial to the FCR tendon. To protect it, carefully incise the dorsal surface of the FCR sheath. Mobilize and gently retract the radial artery laterally. Avoid excessive traction to prevent vasospasm or intimal injury. - Deep Dissection: Identify the radial insertion of the pronator quadratus (PQ) muscle. Dissect proximally to identify the flexor pollicis longus (FPL) muscle belly.
- Subperiosteal Elevation: Elevate the pronator quadratus and the FPL subperiosteally from radial to ulnar. Retract these muscles ulnarly to expose the distal diaphysis and the metaphyseal-diaphyseal junction of the radius.
Osteotomy and Rigid Internal Fixation
The location of the osteotomy is critical. While metaphyseal bone heals faster due to its cancellous nature, the palmar flare of the distal radius makes plate contouring and rigid fixation difficult. Therefore, a diaphyseal osteotomy, as recommended by Almquist and Burns, is preferred to ensure adequate cortical purchase for the screws.
- Plate Templating: Select a dynamic compression plate (DCP) or a specialized radial shortening plate. Position the plate proximal enough to allow the placement of at least three bicortical screws in the distal fragment.
- Pre-drilling: Before making the osteotomy cut, apply the plate to the intact radius. Drill, tap, and insert the distal two screws to establish the exact rotational alignment and trajectory.
- Osteotomy Execution: Remove the plate and screws. Using a thin-bladed oscillating saw under continuous saline irrigation (to prevent thermal necrosis), perform a transverse osteotomy at the planned diaphyseal site.
- Shortening: Resect the pre-calculated segment of bone (usually 2 to 3 mm) based on the preoperative ulnar-minus variance measurements.
- Reattachment and Compression: Reattach the plate to the distal fragment using the pre-drilled holes. This guarantees that the original rotational alignment of the radius is perfectly restored.
- Applying Compression: Before placing the proximal screws, use an articulated tension device or eccentric drilling in the dynamic compression holes to strictly compress the osteotomy site. Secure the reduction with bone forceps.
- Fluoroscopic Verification: Obtain intraoperative C-arm fluoroscopic images (PA and Lateral) to confirm the exact radioulnar length, neutral variance, and hardware placement. Ensure no screws are penetrating the DRUJ.
- Final Fixation: Insert the remaining proximal screws to achieve rigid, absolute stability.
Closure and Postoperative Rehabilitation Protocol
- Hemostasis: Deflate the tourniquet and obtain meticulous hemostasis using bipolar electrocautery. Insert a closed suction drain if significant dead space or oozing is present.
- Muscle Repair: Allow the pronator quadratus to fall back over the plate. It may be loosely tacked, but do not close it under tension.
- Fascial Closure:
> Surgical Pitfall: Leave the deep forearm fascia open. Closing the antebrachial fascia tightly over the hardware and swollen tissues significantly increases the risk of postoperative acute compartment syndrome. - Skin Closure: Close the subcutaneous tissues with absorbable sutures and the skin with non-absorbable monofilament or staples.
- Immobilization: Apply a sterile dressing and immobilize the forearm in a well-padded sugar-tong splint to prevent forearm rotation while allowing digital swelling.
Postoperative Care Timeline:
* Days 1-2: The surgical drain is removed. Immediate active range of motion of the fingers and thumb is highly encouraged to prevent tendon adhesions and reduce edema.
* Days 10-14: The sugar-tong splint is removed for wound inspection and suture removal. A solid long-arm cast (extending above the elbow) or a rigid custom sugar-tong splint is applied to strictly control pronosupination.
* Week 4: The cast is removed, and interval radiographs are obtained to assess early callus formation and maintenance of hardware position. The patient is placed back into a long-arm cast for an additional 4 weeks.
* Weeks 8-10: Immobilization is discontinued based on the radiographic evidence of solid bony union at the osteotomy site. The patient is transitioned to a removable wrist splint and begins a formal physical therapy program focusing on restoring wrist flexion/extension and forearm pronation/supination. Light use of the hand is encouraged throughout the convalescent period, with a gradual return to heavy loading and sports permitted only after complete radiographic consolidation and restoration of dynamic strength.
You Might Also Like

