Advanced Arthroscopy and Tendoscopy of the Foot and Ankle: First MTP Joint and Hindfoot Tendons

Key Takeaway
First metatarsophalangeal (MTP) joint arthroscopy and hindfoot tendoscopy are advanced, minimally invasive techniques used to treat osteochondral lesions, synovitis, and tendon pathology. This guide details the precise portal placements, surgical anatomy, and operative steps required for successful first MTP arthroscopy, peroneal tendoscopy, and posterior tibial tendoscopy, providing orthopedic surgeons with evidence-based protocols to optimize patient outcomes and minimize iatrogenic complications.
INTRODUCTION TO SMALL JOINT ARTHROSCOPY OF THE FOOT AND ANKLE
The evolution of small joint arthroscopy and tendoscopy has revolutionized the management of foot and ankle pathology. Historically, open arthrotomies and extensive tenolyses were required to address intra-articular and peritendinous lesions, often resulting in significant postoperative morbidity, arthrofibrosis, and prolonged rehabilitation. Today, first metatarsophalangeal (MTP) joint arthroscopy, alongside peroneal and posterior tibial tendoscopy, offers orthopedic surgeons a minimally invasive armamentarium to diagnose and treat complex conditions with unparalleled visualization.
This comprehensive guide delineates the indications, precise anatomical portal placements, and step-by-step surgical techniques for first MTP joint arthroscopy and hindfoot tendoscopy, adhering to the highest standards of contemporary operative orthopedics.
FIRST METATARSOPHALANGEAL JOINT ARTHROSCOPY
First metatarsophalangeal joint arthroscopy is a technically demanding but highly rewarding procedure. The constrained nature of the joint requires meticulous technique, specialized equipment, and a profound understanding of the local neurovascular anatomy to avoid iatrogenic injury.
Indications and Patient Selection
Arthroscopic intervention in the first MTP joint is indicated for a variety of intra-articular pathologies. Careful patient selection and preoperative advanced imaging (MRI or CT arthrography) are paramount.
- Osteochondral Lesions (OCLs): Primarily affecting the first metatarsal head. Arthroscopy allows for precise debridement, microfracture, or marrow stimulation techniques.
- Early Hallux Rigidus (Grades I and II): Management of early osteophytosis (cheilectomy) and chondromalacia before the onset of end-stage joint space obliteration.
- Loose Bodies: Extraction of osteochondral fragments or synovial chondromatosis.
- Inflammatory and Crystalline Arthropathies: Synovectomy and joint lavage for rheumatoid arthritis, synovitis, and gouty arthritis (removal of tophaceous deposits).
- Arthrofibrosis: Lysis of adhesions following previous trauma or open surgery.
- Adjunctive Procedures: Arthroscopic or arthroscopic-assisted techniques are increasingly utilized for first MTP joint arthrodesis (cartilage denudation) and soft tissue releases (lateral release) for hallux valgus prior to a distal first metatarsal osteotomy.
Clinical Pearl: Arthroscopic preparation for first MTP arthrodesis preserves the soft tissue envelope, potentially enhancing fusion rates and reducing wound complications in high-risk patients (e.g., diabetics, smokers).
Clinical Anatomy and Portal Placement
The primary landmarks for first MTP joint arthroscopy are the extensor hallucis longus (EHL) tendon, the extensor hallucis brevis (EHB) tendon, and the joint line.
- Dorsomedial Portal: Established medial to the EHL tendon at the level of the joint line. The primary risk here is injury to the dorsomedial cutaneous nerve (a branch of the superficial peroneal nerve).
- Dorsolateral Portal: Established lateral to the EHL tendon. The surgeon must be cognizant of the deep peroneal nerve and the dorsal metatarsal artery, which lie in close proximity.
Surgical Technique: First MTP Arthroscopy
- Anesthesia and Positioning: The procedure is typically performed under regional anesthesia (ankle block) or general anesthesia. The patient is positioned supine. A non-invasive distraction device (e.g., Chinese finger trap on the hallux) is applied to the great toe, utilizing 5 to 10 lbs of traction to open the joint space.
- Equipment: A 1.9-mm or 2.7-mm 30-degree short arthroscope is standard. Small joint shavers (2.0-mm or 2.9-mm) and radiofrequency wands are utilized for debridement.
- Portal Establishment: The joint is insufflated with 2 to 3 mL of normal saline using an 18-gauge needle to distend the capsule. The dorsomedial portal is created first using a #11 blade, incising only the skin. A small hemostat is used for blunt dissection down to the capsule to protect cutaneous nerves. The trocar is introduced with a sweeping motion.
- Diagnostic Round: A systematic evaluation of the articular cartilage of the metatarsal head and proximal phalanx, the medial and lateral gutters, and the sesamoid complex is performed.
- Therapeutic Intervention:
- For OCLs: Unstable cartilage is debrided to a stable rim, and the subchondral bone is microfractured using a specialized awl or K-wire.
- For Hallux Rigidus: Dorsal osteophytes are resected using a small burr, ensuring adequate dorsiflexion is restored intraoperatively.
- For Hallux Valgus: A lateral soft tissue release can be performed by sectioning the lateral capsule and the adductor hallucis tendon insertion under direct visualization.
PERONEAL TENDOSCOPY
Peroneal tendoscopy allows for the direct visualization and treatment of the peroneus longus and brevis tendons within the retromalleolar groove and the lateral calcaneal wall.
Indications
- Chronic tenosynovitis refractory to conservative management.
- Evaluation and debridement of partial-thickness tendon tears.
- Assessment of peroneal tendon subluxation and superior peroneal retinaculum (SPR) integrity.
- Removal of low-lying muscle bellies or anomalous muscles (e.g., peroneus quartus) causing impingement.
Positioning and Portal Placement
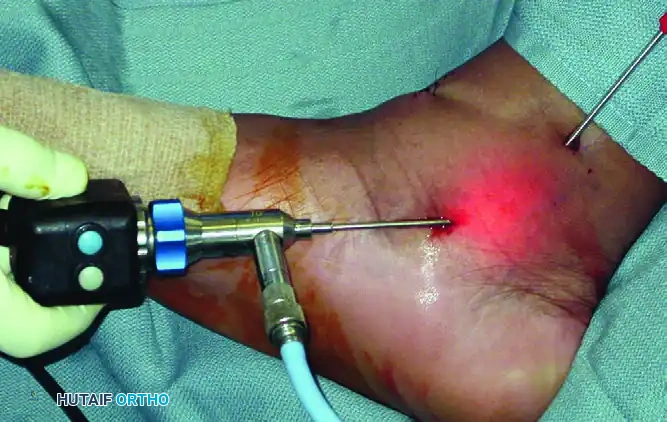
The patient is positioned in the lateral decubitus position or supine with a large bump under the ipsilateral hip to internally rotate the leg, providing excellent access to the lateral hindfoot. A thigh tourniquet is applied.
As demonstrated in the surgical setup above, portal placement is critical. The portals are typically placed approximately 4 cm apart along the course of the peroneal tendon sheath.
* Distal Portal: Located approximately 1.5 to 2 cm distal to the tip of the lateral malleolus.
* Proximal Portal: Located 2 to 3 cm proximal to the tip of the lateral malleolus, directly over the tendon sheath.
Surgical Warning: The sural nerve courses in close proximity to the peroneal tendon sheath, particularly near the distal portal. Blunt dissection with a mosquito hemostat down to the tendon sheath is mandatory to prevent iatrogenic neuroma formation.
Diagnostic and Therapeutic Technique
A 2.7-mm 30-degree arthroscope is introduced into the proximal portal, and fluid flow is established. The tendon sheath is often filled with hypertrophic synovium in pathologic states, requiring immediate limited synovectomy with a 2.9-mm shaver introduced through the distal portal to establish a clear visual field.
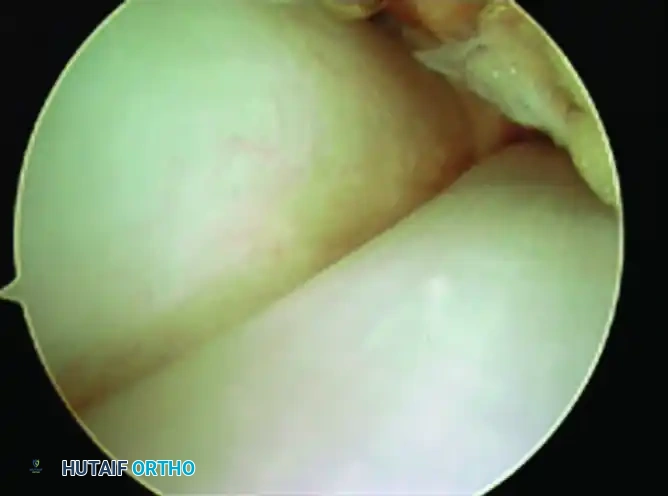
Once the sheath is cleared, the anatomical relationship between the tendons becomes evident. As seen in the arthroscopic view above, the peroneal brevis tendon (a) is situated medial and deep to the peroneus longus tendon (b) when viewed from the portal proximal to the fibula.
The surgeon must dynamically examine the tendons by passively everting and inverting the ankle. Fraying or longitudinal split tears of the peroneus brevis (often caused by impingement against the fibula) can be debrided using a motorized shaver or thermal wand. If a massive tear requiring tubularization is identified, the tendoscopic procedure is easily converted to an open approach.
POSTERIOR TIBIAL TENDOSCOPY
Posterior tibial tendon (PTT) dysfunction is a leading cause of adult-acquired flatfoot deformity. Tendoscopy of the PTT is an invaluable tool for early-stage disease, allowing for aggressive synovectomy and tendon debridement before structural failure occurs.
Indications
- Stage I Posterior Tibial Tendon Dysfunction (PTTD) characterized by tenosynovitis without deformity.
- Early Stage II PTTD (as an adjunct to bony procedures like medializing calcaneal osteotomy).
- Post-traumatic adhesions or partial tears of the PTT.
Positioning and Portal Placement
The patient is positioned supine with the leg externally rotated (frog-leg position) to expose the medial ankle.
The portals are established along the anatomical course of the PTT, posterior and distal to the medial malleolus.
* Proximal Portal: Placed 2 to 3 cm proximal to the tip of the medial malleolus.
* Distal Portal: Placed near the navicular insertion of the tendon.
As illustrated in the operative image above, the arthroscope is typically placed in the distal portal, while the motorized shaver is introduced through the proximal portal in the right ankle. This configuration allows the surgeon to work antegrade along the tendon sheath.
Surgical Warning: The great saphenous vein and saphenous nerve run anterior to the medial malleolus, while the posterior tibial neurovascular bundle lies immediately posterior and lateral to the PTT. Strict adherence to the "nick and spread" technique is required to avoid catastrophic vascular injury or nerve transection.
Surgical Technique
Following insufflation of the tendon sheath, the 2.7-mm arthroscope is introduced. The normal PTT should appear glistening and white. In cases of Stage I PTTD, the surgeon will encounter florid, hypervascular synovitis.
A thorough tenosynovectomy is performed using a shaver. The tendon is inspected circumferentially by rotating the scope and applying passive inversion/eversion to the foot. Any degenerative, fibrillated tendon tissue is carefully debrided. If a significant longitudinal tear is identified that compromises more than 50% of the tendon's cross-sectional area, tendoscopy should be abandoned in favor of an open exploration and potential tendon transfer (e.g., FDL transfer).
POSTOPERATIVE REHABILITATION PROTOCOLS
Rehabilitation following small joint arthroscopy and tendoscopy is dictated by the specific pathology treated rather than the surgical approach itself. However, the minimally invasive nature of these procedures generally allows for accelerated recovery.
First MTP Joint Arthroscopy
- Debridement/Synovectomy: Patients are typically allowed immediate heel-weight-bearing in a stiff-soled postoperative shoe. Active and passive range of motion (ROM) exercises of the hallux begin at 3 to 5 days postoperatively to prevent arthrofibrosis. Transition to normal footwear occurs at 2 to 3 weeks.
- Microfracture for OCL: Patients are kept strictly non-weight-bearing or heel-weight-bearing only for 4 to 6 weeks to allow the fibrocartilage clot to mature. Early, protected ROM is encouraged.
Peroneal and Posterior Tibial Tendoscopy
- Isolated Synovectomy: Patients are placed in a controlled ankle motion (CAM) boot and allowed progressive weight-bearing as tolerated. Physical therapy focuses on edema control, early active ROM, and eccentric strengthening beginning at week 2.
- Tendon Debridement: If significant intra-substance debridement was performed, the ankle may be immobilized in a short-leg cast or CAM boot in a neutral position for 2 to 3 weeks to protect the tendon, followed by a graduated stretching and strengthening program. Return to high-impact sports is typically anticipated between 8 to 12 weeks.
COMPLICATIONS AND AVOIDANCE
While minimally invasive, foot and ankle arthroscopy carries specific risks that the orthopedic surgeon must actively mitigate:
- Neurological Injury: The most common complication. Superficial peroneal nerve branches (1st MTP), sural nerve (peroneal tendoscopy), and saphenous nerve (PTT tendoscopy) are at high risk. Avoidance: Always use superficial skin incisions followed by blunt hemostat dissection down to the capsule or sheath.
- Tendon Laceration: Aggressive use of the motorized shaver within the confined space of a tendon sheath can inadvertently damage healthy tendon fibers. Avoidance: Always keep the shaver blade facing away from the tendon, utilizing the smooth side of the shaver hood to protect the tendon while resecting synovium.
- Infection and Wound Healing: Though rare in arthroscopy, diabetic patients and smokers are at higher risk. Avoidance: Meticulous closure of portals (often with simple nylon sutures or adhesive strips) and appropriate perioperative antibiotic prophylaxis.
- Fluid Extravasation: Excessive fluid pressure can lead to compartment syndrome of the foot or calf, particularly during tendoscopy. Avoidance: Use gravity flow or low-pressure pump systems (typically under 40 mmHg). Limit procedure time and monitor the soft tissue tension of the calf and foot throughout the surgery.
You Might Also Like


