Keller Resection Arthroplasty: Principles and Surgical Technique
Key Takeaway
The Keller resection arthroplasty remains a valuable procedure for older patients with moderate-to-severe hallux valgus and first metatarsophalangeal joint arthritis. By combining resection hemiarthroplasty of the proximal phalanx base with medial eminence excision, surgeons can decompress the joint and correct deformity. Careful patient selection, meticulous soft-tissue handling, and precise K-wire stabilization are paramount to preventing complications such as transfer metatarsalgia or cock-up toe deformity.
COMBINED SOFT TISSUE AND BONY PROCEDURES
The surgical management of hallux valgus encompasses a broad spectrum of interventions, ranging from isolated soft tissue rebalancing to complex osseous realignments. Among these, combined soft tissue and bony procedures hold a distinct place, particularly in the management of rigid deformities accompanied by degenerative joint disease.
KELLER RESECTION ARTHROPLASTY: BIOMECHANICS AND RATIONALE
The Keller procedure is a classic, time-honored operation that combines a resection hemiarthroplasty of the first metatarsophalangeal (MTP) joint with the excision of the medial eminence of the first metatarsal. The fundamental biomechanical goal is to decompress the joint and mobilize the hallux by removing the base of the proximal phalanx. This allows for marked correction of the valgus deformity.
However, it is critical to understand the biomechanical trade-offs inherent to this procedure. Because the varus alignment of the first metatarsal is not directly corrected via osteotomy, maintaining the correction of the hallux valgus relies heavily on meticulous soft tissue reconstruction and postoperative scar tissue formation (encapsulation). Historically, complications such as "cock-up" toe deformity, transfer metatarsalgia, and recurrent valgus have been emphasized in the literature. These historical pitfalls often stemmed from over-resection of the phalanx, failure to stabilize the joint with Kirschner wires, or poor patient selection. In contemporary orthopedic practice, when patients are selected carefully and modern technical modifications are employed, complications are uncommon, and patient satisfaction is remarkably high.
Surgical Warning: The Keller procedure inherently destabilizes the intrinsic musculature of the hallux by detaching the insertion of the flexor hallucis brevis (FHB) and the adductor hallucis. Meticulous capsulorrhaphy and temporary axial K-wire fixation are absolute requirements to prevent postoperative dorsal subluxation (cock-up toe) driven by the unopposed pull of the extensor hallucis longus (EHL).
INDICATIONS AND PATIENT SELECTION
The success of the Keller procedure is inextricably linked to strict patient selection. It is not an operation for the young, active patient, nor is it appropriate for flexible deformities that can be managed with joint-sparing osteotomies.
Primary Candidates:
* Age: Patients older than 50 to 60 years with lower functional demands.
* Deformity Severity: Moderate-to-severe hallux valgus (30 to 45 degrees).
* Intermetatarsal Angle (IMA): 13 degrees or less, indicating mild-to-moderate metatarsus primus varus.
* Clinical Symptoms: Intractable pain over the medial eminence with any shoe wear, severely limiting footwear options. Intra-articular pain indicative of degenerative joint disease.
Radiographic Indications:
* An incongruous first MTP joint caused by lateral subluxation of the phalanx on the metatarsal head.
* Severe lateral displacement of the sesamoid apparatus.
* Evidence of degenerative cartilage changes (joint space narrowing, subchondral sclerosis, osteophytosis) within the first MTP joint.

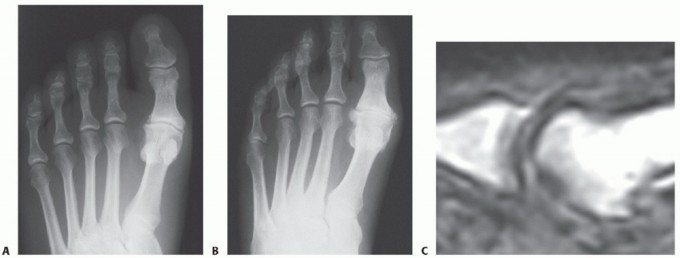
Figure 1: Anteroposterior radiograph of the right foot of a 65-year-old patient showing mild-to-moderate deformity and mild degenerative changes at the first MTP joint; the patient presented with both intra-articular and periarticular symptoms.

Figure 2: Twelve years post-Keller procedure with excision of the fibular sesamoid. Note the correction of the first metatarsal varus and the maintenance of sufficient joint space to allow a functional range of motion.
EXPANDED INDICATIONS: TECHNICAL MODIFICATIONS
While the classic Keller procedure is limited to the parameters above, two specific technical modifications can expand its utility to include older patients with far more severe deformities:
1. Fibular Sesamoidectomy
2. Lateral Displacement of the First Metatarsal
Patients presenting with 50 degrees or more of hallux valgus, 18 to 20 degrees of first metatarsal varus, complete lateral dislocation of the sesamoids, marked degenerative changes, and severe pronation of the hallux can achieve excellent functional and cosmetic outcomes when these modifications are integrated into the standard technique.


Figure 3: Severe hallux valgus with prominent bursa formation in a 70-year-old woman. Anteroposterior and lateral clinical photographs demonstrate the profound nature of the deformity.


Figure 4: Postoperative clinical photograph and weight-bearing radiographs of the same patient demonstrating excellent correction of the deformity utilizing the modified Keller procedure.
SURGICAL TECHNIQUE: STEP-BY-STEP
1. Anesthesia and Preparation
- Assess pedal pulses preoperatively. If vascular status is adequate, utilize an Esmarch wrap tourniquet at the ankle or calf to ensure a bloodless field.
- Administer a regional forefoot block using a 1:1 mixture of 1% lidocaine (Xylocaine) and 0.5% bupivacaine (Marcaine) without epinephrine, adhering to standard weight-based dose limits.
2. Incision and Superficial Dissection
- Make a straight, midline medial longitudinal incision. Begin 1 cm proximal to the interphalangeal (IP) joint of the hallux and extend it proximally to the junction of the distal and middle thirds of the first metatarsal.
- Clinical Pearl: This lengthy incision is deliberately chosen to avoid excessive traction tension on the skin edges during deep retraction, which can lead to marginal necrosis.
- Utilize blunt dissection to locate the most medial branch of the superficial peroneal nerve, typically found at the proximal-dorsal edge of the medial eminence. Gently retract it dorsally for protection.
3. Deep Exposure and Capsular Flap
- Carry the dissection down to the first metatarsal in the midline medially. Begin at the proximal limit of the wound, extending distally across the midline of the medial eminence, and continue along the proximal phalanx to the distal extent of the wound.
- Raise the deep flap of tissue (capsule and periosteum) by sharp dissection dorsally, starting at the junction of the medial eminence and the metatarsal shaft.
- Elevate the periosteum and capsule dorsally, exposing up to one-third to one-half the width of the metatarsal head and neck.
- At the joint level, continue capsular elevation along the extensor hallucis brevis (EHB) insertion until the proximal third of the proximal phalanx is exposed as far laterally as possible under direct vision.
- Surgical Tip: Have an assistant actively pronate the hallux as the dissection proceeds laterally. This maneuver significantly improves visualization of the lateral phalangeal base. Subperiosteal dissection should strictly expose only the portion of the proximal phalanx slated for resection.
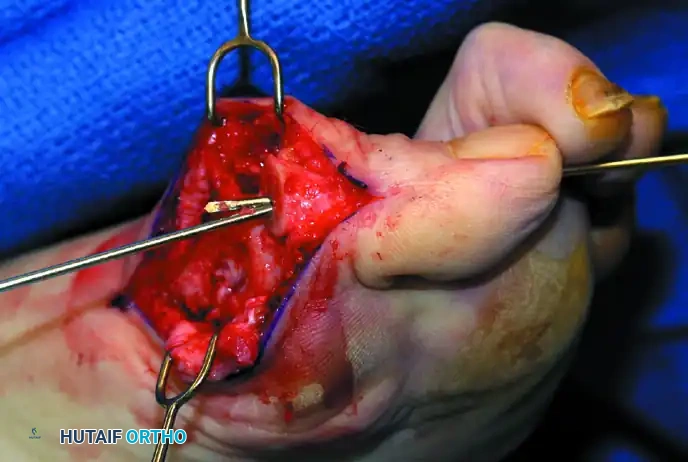
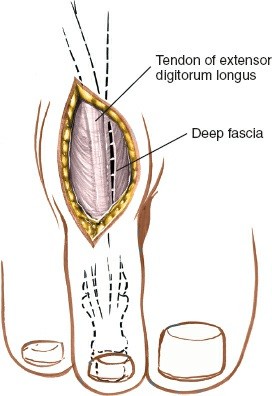
Figure 5: Intraoperative exposure demonstrating the medial capsular incision and initial elevation of the soft tissue envelope.
4. Plantar Dissection and FHL Protection
- Dissect plantarly just enough to expose the plantar aspect of the medial eminence proximally, the tibial sesamoid in the center of the wound, and the plantar-medial corner of the proximal phalanx.
- Supinate the proximal phalanx to expose its plantar corner and the proximal third of the shaft for sharp dissection.
🚨 CRITICAL ANATOMICAL PITFALL: The proximal phalanx is round on its dorsal, medial, and lateral sides, but its plantar surface is flat and becomes distinctly concave in the midline to accommodate the flexor hallucis longus (FHL) tendon. This contour change must be anticipated during dissection and osteotomy to avoid catastrophic iatrogenic transection of the FHL.
- By blunt dissection, identify the FHL tendon. Retract it plantarward using a small right-angle or malleable retractor to protect it throughout the subsequent bony resection.
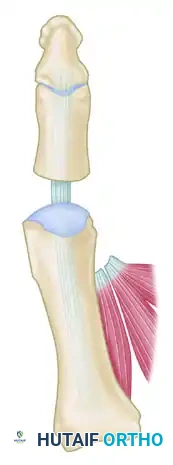
Figure 6: Anatomical diagram highlighting the course of the Flexor Hallucis Longus (FHL) beneath the concave plantar aspect of the proximal phalanx.
5. Bony Resection: Medial Eminence and Proximal Phalanx
- Medial Eminence: Resect the medial eminence at the sagittal groove. Begin dorsally at its distal edge and direct a 9-mm oscillating saw blade (or a sharp osteotome) plantarward and slightly medially (5 to 10 degrees) to avoid skiving into the articular surface.
- Proximal Phalanx: Remove the base of the proximal phalanx exactly at the metaphyseal-diaphyseal junction. This typically constitutes the proximal one-third of the phalanx.
- To prevent damage to the FHL and the plantar neurovascular bundles, place a retractor over the bone dorsally and plantarward, and rotate the phalanx into view. Do not allow the saw blade to exit the far cortex by more than 1 to 2 mm.
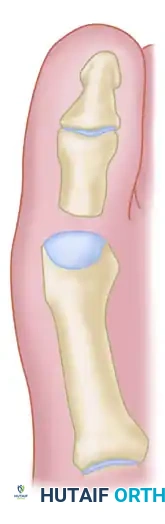
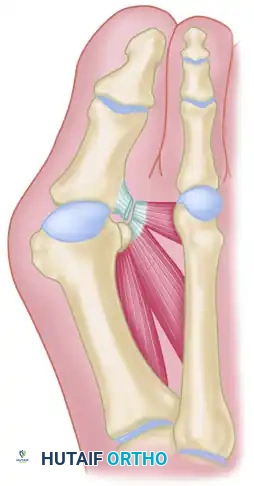
Figure 7: Diagrammatic representation of the Keller technique, illustrating the resection of the proximal phalanx, release of the adductor tendon, and resection of the medial eminence.


Figure 8: (Left) The metaphyseal-diaphyseal junction of the proximal phalanx dictates the level of resection. (Right) Cross-sectional view noting the concave plantar aspect of the proximal phalanx housing the FHL tendon.
- Once the osteotomy is complete, grasp the basilar fragment with a small Kocher clamp or towel clip. Rotate the fragment while applying medial traction to excise it. Lift it away from its lateral attachments, which primarily consist of the lateral collateral ligaments and the adductor hallucis tendinous insertion.
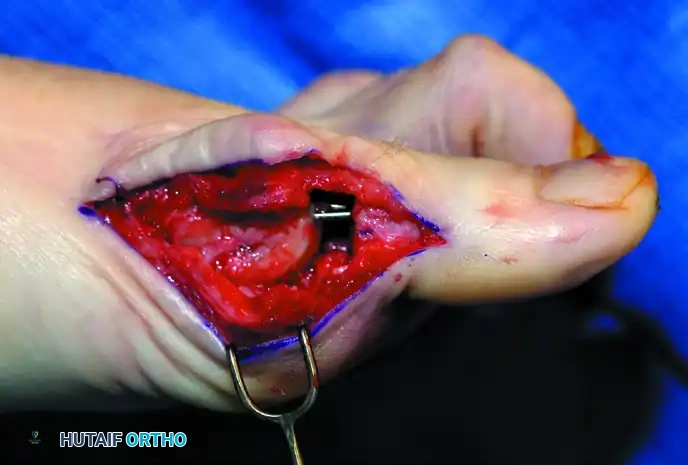

Figure 9: Intraoperative extraction of the resected proximal phalangeal base using a Kocher clamp.
MODIFICATION: REMOVAL OF THE FIBULAR SESAMOID
In cases of severe deformity (>50 degrees valgus) with complete lateral subluxation of the sesamoid apparatus, fibular sesamoidectomy is indicated to remove the deforming force of the adductor hallucis and allow the first metatarsal to translate laterally.
- After the medial eminence and phalangeal base have been excised, place a sturdy two-toothed retractor beneath the metatarsal head. Have an assistant lift the metatarsal dorsally to maximize plantar exposure.
- Using a Freer elevator or a small osteotome, mobilize the fibular sesamoid. This can be challenging in elderly patients due to severe deformity and fibrous adherence of the sesamoid to the plantar aspect of the metatarsal head.
- Once mobile, identify the FHL tendon by placing traction on the hallux and passively flexing/extending the IP joint. The tendon will be visible just distal to and straddled by the sesamoids.
- Identify and protect the lateral neurovascular bundle located just lateral to the tendon via blunt dissection.
- Apply firm medial traction to the plantar-medial capsule. This maneuver brings the intersesamoid ligament into clear view.
- Incise the intersesamoid ligament longitudinally using a No. 67 Beaver or No. 15 blade. If using tenotomy scissors, carefully place one arm under the ligament (resting dorsal to the FHL) and the other arm dorsal to the ligament.
- Grasp the fibular sesamoid firmly with a Kocher clamp. Flex the toe at the IP and MTP joints to relax the FHL tendon, and pull the fibular sesamoid distally and medially to excise it completely.
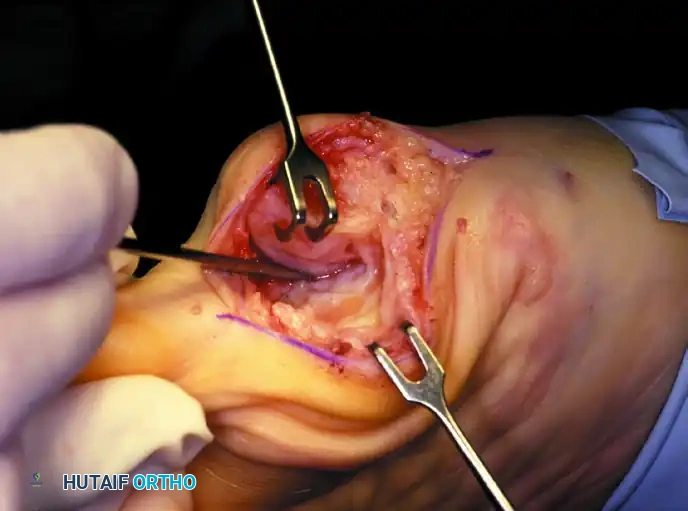
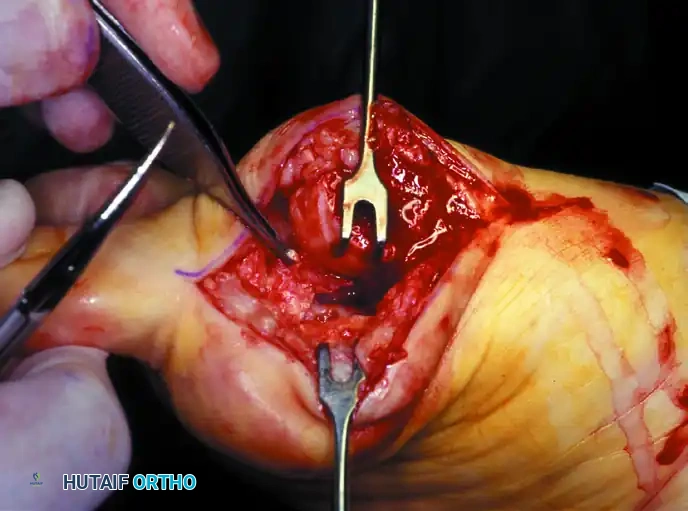
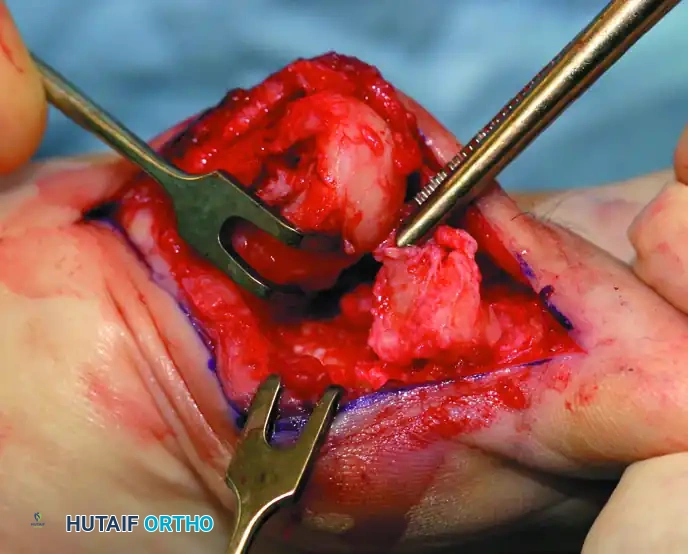
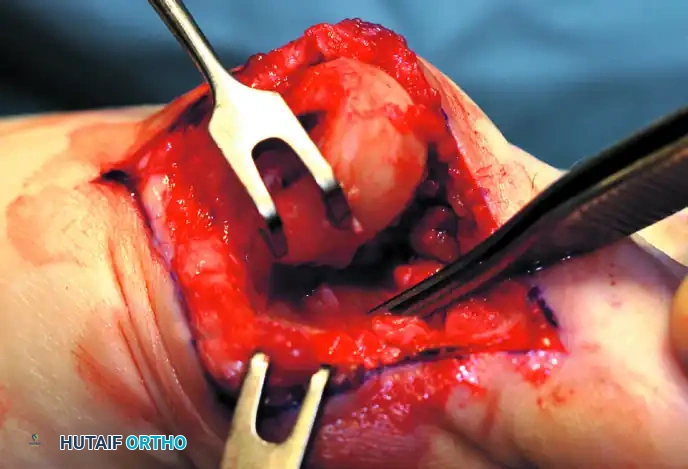
Figure 10: Stepwise diagrammatic representation of fibular sesamoidectomy. Note the relationship between the intersesamoid ligament, the tibial/fibular sesamoids, and the FHL.

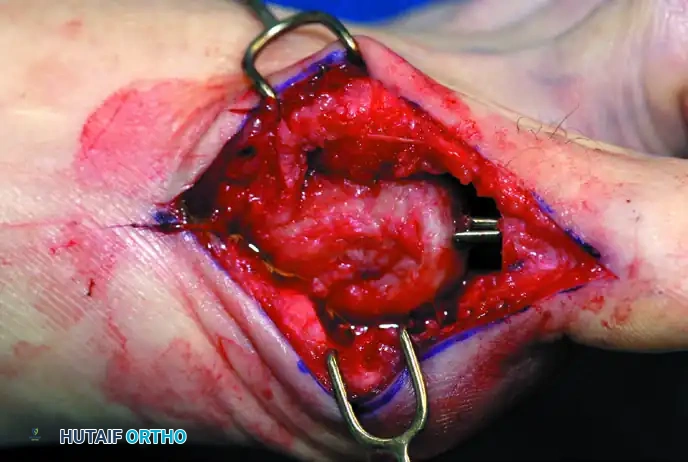
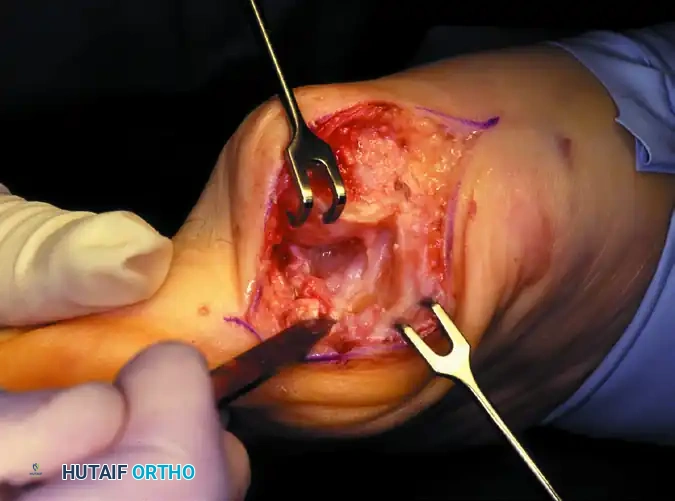
Figure 11: Intraoperative visualization of the sesamoid apparatus and subsequent excision of the fibular sesamoid.
6. Axial Pinning and Alignment
Stabilization of the pseudoarticulation is paramount to allow the capsule to heal at the correct length and tension, thereby preventing a cock-up deformity.
- With the ankle held at 90 degrees, bring
Associated Surgical & Radiographic Imaging
You Might Also Like