Mastering Rotator Cuff Repair: Pathophysiology, Indications, and Surgical Techniques
Key Takeaway
Rotator cuff tears present a complex clinical challenge requiring a nuanced, evidence-based approach. This comprehensive guide details the natural history, biomechanics, and classification of both partial and full-thickness tears. It provides orthopedic surgeons with rigorous protocols for nonoperative management, precise surgical indications, and step-by-step operative techniques—including arthroscopic, mini-open, and open repairs—ensuring optimal functional recovery and pain relief in diverse patient populations.
PATHOPHYSIOLOGY AND CLINICAL PRESENTATION
Most patients presenting with a pathological condition of the rotator cuff describe an insidious onset of progressive pain and weakness, accompanied by a concomitant loss of active motion. Pain is classically exacerbated at night, frequently disrupting sleep, and is commonly referred to the lateral brachium at the deltoid insertion.
In the early stages of rotator cuff disease, passive motion typically remains full. However, as the condition progresses, pain limits active motion to such a degree that secondary adhesive capsulitis may develop. Notably, the majority of patients cannot recall a specific traumatic incident referable to the onset of their symptoms, highlighting the degenerative nature of most tears. Treatment recommendations must be highly individualized, based on the patient’s physiological age, symptom severity, functional demands, and a thorough understanding of the natural history of rotator cuff pathology.
The Natural History of Rotator Cuff Tears
The natural history of rotator cuff tears is notoriously unpredictable. While many patients with full-thickness rotator cuff tears remain entirely asymptomatic or respond favorably to nonoperative modalities, longitudinal studies indicate a clear risk of progression. Previously asymptomatic tears frequently become symptomatic, and existing tears can progress in size, eventually becoming irreparable.
Rotator cuff pathology is ubiquitous in the aging population. Cadaveric anatomical studies have reported rotator cuff tears in 30% to 50% of specimens, suggesting that tendon degeneration is, to some extent, a normal part of the aging process. Furthermore, the presence of rotator cuff disease correlates strongly with age; epidemiological data demonstrate that after the age of 66 years, there is a 50% likelihood of bilateral tears.
💡 Clinical Pearl: The Bilateral Phenomenon
When counseling a patient with a unilateral symptomatic rotator cuff tear, the surgeon must evaluate the contralateral shoulder. Studies of patients with bilateral tears reveal that even if one side is asymptomatic at presentation, over 50% of these patients will develop symptoms in the previously asymptomatic shoulder during long-term follow-up.
CLASSIFICATION OF ROTATOR CUFF TEARS
Accurate classification is essential for preoperative planning, standardizing research reporting, and determining the appropriate surgical intervention.
Classification of Full-Thickness Tears by Size (Box 46-2)
- Small tear: < 1 cm
- Medium tear: 1 to < 3 cm
- Large tear: 3 to < 5 cm
- Massive tear: ≥ 5 cm (often involving two or more entire tendons)
Partial-Thickness Tears
Partial-thickness tears are categorized by their anatomical location: articular-sided, bursal-sided, or intratendinous. Intratendinous tears are notoriously difficult to diagnose via arthroscopy, MRI, or ultrasound compared to their articular or bursal counterparts. Consequently, the true prevalence of partial-thickness tears is likely much higher than currently documented in the orthopedic literature.
NONOPERATIVE MANAGEMENT
Full-thickness rotator cuff tears are often compatible with normal, pain-free function. In 1962, McLaughlin advanced five foundational reasons to avoid early repair of the average rupture:
1. At least 25% of cadaver shoulders exhibited a torn or degenerated cuff.
2. Approximately 50% of patients recovered spontaneously without surgical intervention.
3. Immediate repair offered no distinct advantages because the rupture invariably occurred in diseased, degenerative tendon tissue.
4. The clinical results of early versus late repair were statistically similar.
5. Early clinical diagnosis was inherently difficult prior to advanced imaging.
Today, resolution of symptoms is reported in 33% to 90% of patients treated nonoperatively.
Indications for Conservative Care
Nonoperative treatment is the initial recommendation for elderly patients, low-demand individuals, and those with asymptomatic tears or tears that do not limit activities of daily living (ADLs).
For partial-thickness tears, an initial nonoperative program is mandatory. This includes:
* Activity modification and avoidance of overhead loading.
* Targeted stretching to address posterior capsular tightness.
* Strengthening exercises focusing on the periscapular stabilizers and remaining intact cuff.
* Judicious use of nonsteroidal anti-inflammatory drugs (NSAIDs) and subacromial corticosteroid injections.
⚠️ Clinical Pitfall: The Chronicity Factor
When the decision to treat nonoperatively is made, it must be instituted promptly and aggressively. The duration of symptoms correlates inversely with the long-term success of nonsurgical management. Patients experiencing symptoms for longer than 6 months demonstrate significantly poorer outcomes and higher rates of tear progression.
SURGICAL INDICATIONS AND CONTRAINDICATIONS
The primary goal of operative management is predictable, durable pain relief. Improvement of function and strength is a secondary, albeit highly important, consideration. Functional recovery is less predictable than pain relief and is heavily dependent on the patient's age, the chronicity and size of the tear (which dictates tissue quality and muscle fatty infiltration), and strict adherence to postoperative rehabilitation.
Indications for Surgery
- Acute Traumatic Tears: Surgery is highly appropriate for an acute rotator cuff injury in a young patient, or an older patient (60 to 70 years old) with a defined traumatic event who presents with sudden inability to externally rotate or elevate the arm against resistance. Early repair in this cohort yields excellent return of strength and function.
- Failure of Conservative Management: In elderly or low-activity patients, a conservative trial of 8 to 12 weeks is standard. If there is no improvement, surgical intervention is warranted to halt the progression of rotator cuff musculature atrophy and fatty infiltration.
- Progression of Partial Tears: Imaging and clinical studies suggest that partial-thickness tears progress in up to 80% of patients. Operative management is indicated when conservative measures fail.
Absolute Contraindications
- Concomitant Stiffness (Adhesive Capsulitis): Surgery is strictly contraindicated in the presence of significant preoperative stiffness. Any loss of passive range of motion must be aggressively corrected via physical therapy (or manipulation under anesthesia/capsular release) prior to rotator cuff repair. Operating on a stiff shoulder virtually guarantees severe, recalcitrant postoperative stiffness.
PREOPERATIVE PLANNING AND IMAGING
Before proceeding to rotator cuff repair, advanced imaging is required. Magnetic Resonance Imaging (MRI) without contrast is the gold standard for evaluating tear size, tendon retraction (Patte classification), and muscle atrophy/fatty infiltration (Goutallier classification). Ultrasound is a highly effective, dynamic alternative in experienced hands.
Despite the reliance on imaging, clinical results of repair are often good to excellent even when postoperative imaging demonstrates a lack of structural healing (rerupture).
SURGICAL APPROACHES AND TECHNIQUES
Historically, subacromial decompression alone was utilized for cuff disease. However, contemporary data demonstrate that decompression alone yields satisfactory outcomes in only 8% to 59% of cases, with results deteriorating significantly over time. Repair is vastly superior.
Diagnostic Arthroscopy
Before committing to a specific repair strategy, diagnostic arthroscopy is mandatory. It allows the surgeon to:
* Confirm the exact size, geometry, and mobility of the tear.
* Identify and treat concomitant intra-articular pathology (e.g., SLAP lesions, biceps tendinopathy, chondral defects).
* Determine whether the tear should be treated entirely arthroscopically, via an arthroscopic-assisted (mini-open) approach, or converted to a standard open procedure.
Management of Partial-Thickness Tears
The surgical approach to partial-thickness tears depends on the depth of the lesion, patient age, and activity level:
* < 50% Tendon Thickness: Arthroscopic debridement of the frayed tendon edges combined with an arthroscopic subacromial decompression (acromioplasty) is sufficient. Excellent and good results are reported in 80% to 90% of patients.
* > 50% Tendon Thickness: The remaining intact fibers are often degenerative and biomechanically compromised. The standard of care is elliptical excision of the diseased tendon (completion of the tear) followed by anatomical repair to the greater tuberosity footprint.
Arthroscopic Repair of Full-Thickness Tears
Arthroscopic repair is currently the gold standard for small, medium, and most large full-thickness tears. Advantages include comprehensive glenohumeral inspection, preservation of the deltoid origin, minimized soft tissue morbidity, and decreased postoperative pain.
🔪 Surgical Technique 46-2: Arthroscopic Rotator Cuff Repair
Step 1: Patient Positioning and Portal Placement
* The patient is positioned in either the beach-chair or lateral decubitus position, depending on surgeon preference.
* Standard posterior (viewing) and anterior (working) portals are established. A lateral portal is created for subacromial work.
Step 2: Diagnostic Sweep and Biceps Management
* Perform a systematic 15-point diagnostic arthroscopy.
* Evaluate the long head of the biceps tendon; if significant tenosynovitis, tearing, or subluxation is present, perform a biceps tenotomy or tenodesis.
Step 3: Subacromial Decompression (Acromioplasty)
* Perform an anterior acromioplasty. This is a critical component of rotator cuff surgery; historical data confirms that the results of repair without decompression are inferior to the combined procedure.
* Resect the coracoacromial ligament and use a motorized burr to flatten the undersurface of the anterior acromion, converting a Type II or III acromion to a flat Type I morphology.
Step 4: Tear Evaluation and Mobilization
* After standard acromioplasty, evaluate the rotator cuff tear carefully from the bursal side.
* Anatomical Note: Tears typically initiate at the supraspinatus insertion near the bicipital groove and retract medially into the supraspinatus fossa, often adhering to the acromioclavicular joint capsule or base of the coracoid.
* Perform extensive soft-tissue releases. Release the coracohumeral ligament and perform an intra-articular capsular release if the tendon is retracted and immobile. The goal is tension-free reduction of the tendon to the lateral edge of the footprint.
Step 5: Footprint Preparation
* Debride the greater tuberosity footprint using a curette or motorized burr to expose a bleeding cortical bed. Avoid excessive decortication, which weakens anchor purchase.
Step 6: Anchor Placement and Suture Passing
* Place suture anchors at the medial articular margin of the footprint (deadman's angle of 45 degrees).
* Pass sutures through the tendon using an antegrade or retrograde suture-passing device. For optimal biomechanical strength and footprint pressurization, a double-row or transosseous-equivalent (suture bridge) construct is preferred for medium to large tears.
* Tie the medial row, then bring the suture tails laterally to knotless anchors to compress the tendon against the tuberosity.
Mini-Open and Combined Approaches
Open rotator cuff repairs can be performed through a mini-arthrotomy deltoid-splitting approach. This is particularly useful for surgeons transitioning to arthroscopic techniques or for specific complex tear patterns.
An arthroscopic-plus-open technique is highly effective for massive, combined tears involving the subscapularis, supraspinatus, and infraspinatus.
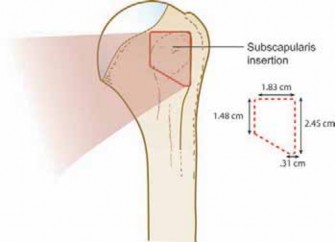
* Technique: The posterosuperior cuff (supraspinatus/infraspinatus) is mobilized and repaired arthroscopically. Subsequently, an open deltopectoral approach is utilized to directly visualize, mobilize, and repair the retracted subscapularis tendon.
* Advantages: This hybrid method allows for the treatment of concomitant intra-articular pathology, facilitates relative ease of subscapularis repair (which can be technically demanding arthroscopically), and creates a robust, reliable biomechanical construct.
OUTCOMES AND COMPLICATIONS
The clinical results of rotator cuff repair in symptomatic patients are highly favorable. Long-term studies (10-year follow-up) demonstrate good to excellent results in approximately 80% of cases.
In four landmark series (Hawkins et al., Neer et al., Ellman et al., and Cofield et al.) encompassing 476 patients, success rates ranged from 78% to 86%, with excellent or good results reported in 383 (80%) of the patients. Overall pain relief is achieved in 87% of patients, correlating with a 77% patient satisfaction rate. Outcomes are generally superior in patients younger than 60 years of age.
The Paradox of Rerupture
A critical concept in rotator cuff surgery is the disconnect between structural healing and clinical outcome. Postoperative imaging (ultrasound or MRI) reveals that rerupture or failure of healing occurs in 20% to 65% of repaired cuffs, particularly in massive tears or older patients.
⚠️ Surgical Warning: Managing Expectations
Despite high rerupture rates, clinical results often remain "good" to "excellent." Patients with structural failures typically maintain their pain relief and exhibit functional improvements compared to their preoperative baseline, likely due to the benefits of subacromial decompression, biceps management, and the re-establishment of a balanced transverse force couple.
POSTOPERATIVE REHABILITATION
The postoperative protocol is as critical as the surgical repair itself. Rehabilitation must balance the protection of the healing tendon-to-bone interface with the prevention of postoperative stiffness.
- Phase I (0-6 weeks): Protection. The shoulder is immobilized in an abduction sling. Only passive range of motion (PROM) is permitted. Active motion is strictly prohibited to prevent catastrophic failure of the repair construct.
- Phase II (6-12 weeks): Active-Assisted to Active Motion. The sling is discontinued. Patients begin active-assisted range of motion (AAROM) progressing to active range of motion (AROM).
- Phase III (12-24 weeks): Strengthening. Once full, painless AROM is achieved, progressive resistance exercises are initiated, focusing on the periscapular stabilizers and the rotator cuff.
-
Phase IV (6+ months): Return to Activity. Gradual return to heavy labor or overhead sports, dictated by the recovery of dynamic strength and functional stability.
📚 Medical References
- rotator cuff tearing, J Shoulder Elbow Surg 9:302, 2000.
- Nyffeler RW, Meyer D, Sheikh R, et al: The effect of cementing technique on structural fi xation of pegged glenoid components in total shoulder arthroplasty, J Shoulder Elbow Surg 15:106, 2006.
- Pearl ML, Romeo AA, Wirth MA, et al: Decision making in contemporary shoulder arthroplasty, Instr Course Lect 54:69, 2005.
- Pollock RG, Deliz ED, McIlveen SJ, et al: Prosthetic replacement in rotator cuff-defi cient shoulders, J Shoulder Elbow Surg 1:173, 1992.
- Post M, Haskell SS, Jablon M: Total shoulder replacement with a constrained prosthesis, J Bone Joint Surg 62A:327, 1980.
- Roche C, Angibaud L, Flurin PH, et al: Glenoid loosening in response to dynamic multi-axis eccentric loading: a comparison between keeled and pegged designs with an equivalent radial mismatch, Bull Hosp Jt Dis 63:88, 2006.
- Rozing PM, Brand R:
You Might Also Like