Decompression and Débridement of Massive Rotator Cuff Tears: A Comprehensive Surgical Guide
Key Takeaway
Massive rotator cuff tears present a complex biomechanical challenge, often leading to superior humeral head migration and glenohumeral arthritis. When primary repair is impossible, surgical decompression and meticulous debridement serve as a viable salvage procedure. This approach focuses on alleviating impingement, preserving the coracoacromial arch, and resecting avascular tissue to restore functional kinematics and provide significant pain relief for carefully selected patients.
INTRODUCTION TO MASSIVE ROTATOR CUFF TEARS
The management of massive, irreparable rotator cuff tears remains one of the most formidable challenges in orthopedic surgery. Defined classically by Cofield as tears exceeding 5 centimeters in diameter, or by Gerber as tears involving two or more complete tendon units, these lesions severely disrupt the kinematic chain of the glenohumeral joint. While advancements in arthroscopic techniques, tendon transfers, and reverse total shoulder arthroplasty (RTSA) have expanded the reconstructive armamentarium, there remains a distinct subset of patients for whom open or mini-open decompression and débridement is the most appropriate, evidence-based intervention.
This procedure, heavily championed in the foundational works of Rockwood and colleagues, serves as a critical salvage operation. It is designed primarily to achieve pain relief and restore functional, albeit altered, shoulder mechanics in patients where anatomic repair is biologically or biomechanically impossible.
BIOMECHANICS AND PATHOPHYSIOLOGY
To master the surgical technique of decompression and débridement, the orthopedic surgeon must first possess a profound understanding of the altered biomechanics inherent to the rotator cuff-deficient shoulder.
Disruption of Force Couples
The stability of the glenohumeral joint relies on the delicate balance of coronal and transverse force couples.
* The Transverse Force Couple: Balanced anteriorly by the subscapularis and posteriorly by the infraspinatus and teres minor.
* The Coronal Force Couple: Balanced superiorly by the deltoid and inferiorly by the inferior rotator cuff (infraspinatus, teres minor, and subscapularis).
In the setting of a massive supraspinatus and infraspinatus tear, the coronal force couple is catastrophically uncoupled. The unopposed superior pull of the deltoid leads to superior subluxation of the humeral head.
Rotator Cuff Tear Arthropathy (CTA)
As the humeral head migrates superiorly, it begins to articulate directly with the undersurface of the acromion and the coracoacromial (CA) ligament. This abnormal articulation generates severe shearing forces across the glenoid. Because articular cartilage is biomechanically poorly suited to resist shear forces, rapid osteochondral degradation ensues.
Clinical Pearl: Neer’s Nutritional Hypothesis
Charles Neer postulated that mechanical wear is not the sole driver of rotator cuff tear arthropathy. The massive tear eliminates the closed joint space, leading to a profound loss of hydrostatic fluid pressure. This pressure drop causes a reduction in the quality and chemical content of the synovial fluid, ultimately accelerating cartilage and bone atrophy.
CLINICAL AND RADIOGRAPHIC EVALUATION
Patients typically present with chronic, debilitating shoulder pain, particularly at night, accompanied by profound weakness in forward elevation and external rotation. In severe cases, patients exhibit "pseudoparalysis," an inability to actively elevate the arm beyond 90 degrees despite intact axillary nerve function.
Radiographic Hallmarks
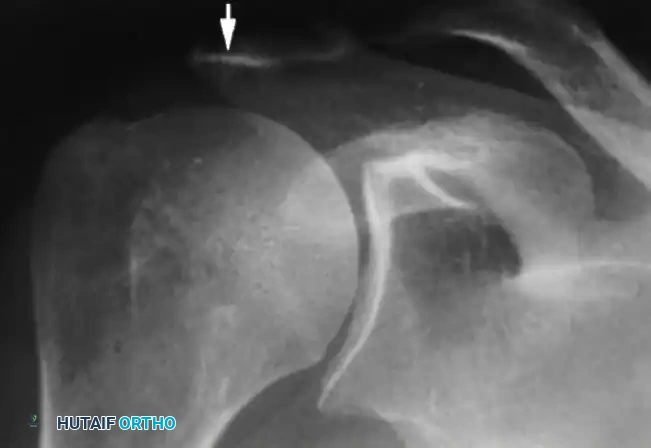
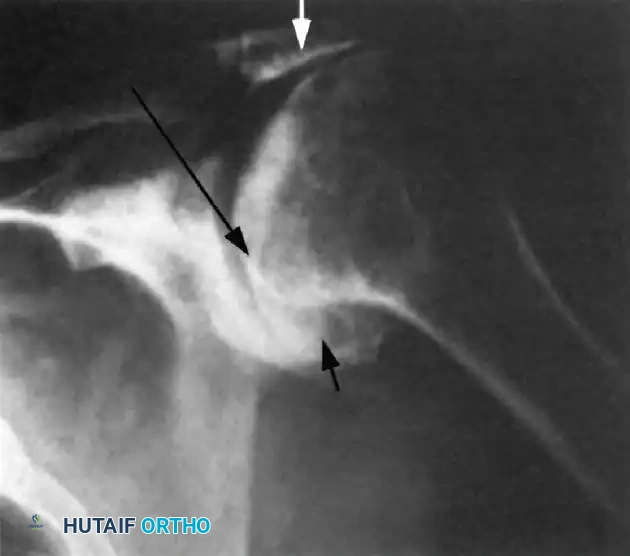
Standard radiographic evaluation must include a true anteroposterior (Grashey), scapular Y, and axillary lateral view. The classic radiographic findings of a chronic massive rotator cuff tear progressing to arthropathy include:
1. Superior Migration: An acromiohumeral interval (AHI) of less than 7 mm.
2. Loss of Joint Space: Progressive narrowing of the glenohumeral articulation.
3. Humeral Head Osteophytes: Inferior osteophyte formation due to altered loading.
4. The "Sourcil Sign": Sclerosis and erosion of the inferior acromial surface as the humeral head chronically "articulates" against the undersurface of the acromion.
INDICATIONS AND PATIENT SELECTION
Careful patient selection is the single most critical determinant of success for decompression and débridement. This procedure is not designed to restore normal strength; it is a pain-relieving operation.
Ideal Candidates:
* Elderly or low-demand patients with intractable pain.
* Patients with massive, retracted, and fatty-infiltrated tears (Goutallier Stage 3 or 4) deemed irreparable.
* Patients with preserved active forward elevation (intact force couples) but severe impingement pain.
* Patients who are medically unfit for prolonged reconstructive surgeries or arthroplasty.
Poor Candidates:
* Young, high-demand laborers.
* Patients with true pseudoparalysis (these patients are better served by RTSA).
* Patients with active workers' compensation claims.
Surgical Warning: Workers' Compensation Outcomes
A special subset of patients comprises those with active workers’ compensation claims. Extensive literature demonstrates that in this specific demographic, only a 40% to 50% success rate can be expected following decompression and débridement, compared to an 80% success rate in the general population.
SURGICAL TECHNIQUE: STEP-BY-STEP APPROACH
The following technique, adapted from Rockwood et al., details the open approach to decompression and débridement.
1. Patient Positioning and Anesthesia
- Position: Place the patient in a semi-seated (beach chair) position. Ensure the head and neck are securely stabilized in a neutral position to avoid cervical neurapraxia.
- Draping: The affected upper extremity must be draped free to allow for full, unhindered manipulation and dynamic intraoperative assessment of impingement.
- Anesthesia: General anesthesia combined with an interscalene regional block is highly recommended for optimal muscle relaxation and postoperative pain control.
2. Incision and Surgical Approach
- Make a 4 to 6 cm incision along the lateral border of the acromion, meticulously following the lines of Langer to ensure optimal cosmetic healing.
- Dissect down to the deltoid fascia.
- Open the interval between the anterior and lateral parts of the deltoid.
- Carefully resect the anterior part of the deltoid from the anterior edge of the acromion.
- Remove 1 to 2 cm of the lateral part of the deltoid from the lateral edge of the acromion to maximize exposure of the subacromial space.
3. Acromioplasty and Coracoacromial Arch Management
The management of the coracoacromial (CA) ligament in the setting of a massive rotator cuff tear is a subject of intense biomechanical importance.
- With an osteotome, remove the portion of the acromion that extends vertically beyond the anterior border of the clavicle.
- Remove the anteroinferior border of the acromion with an osteotome, and smooth the remaining surface with a surgical rasp.
Surgical Pitfall: The Coracoacromial Arch
Historically, the CA ligament was excised along with the acromial fragment. However, in the setting of a massive, irreparable rotator cuff tear, the CA ligament is the only remaining restraint preventing anterosuperior subluxation (escape) of the humeral head. We strongly prefer to preserve the ligament.
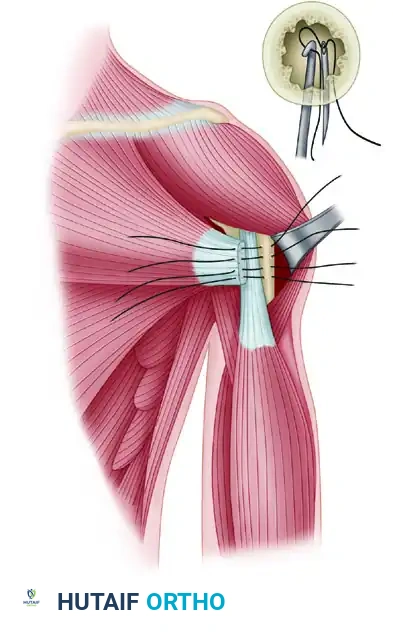
- Modified Technique for Preservation: Sharply detach the coracoacromial ligament from its acromial insertion. Perform the acromioplasty meticulously with an oscillating saw. Once the decompression is complete, use heavy nonabsorbable sutures through transosseous drill holes to rigidly reattach the CA ligament to the acromion, thereby preserving coracoacromial arch stability.
4. Débridement and Tendon Mobilization
- Inspect the rotator cuff footprint. Débride all avascular, friable, and necrotic tissue back to stable, bleeding tendon edges.
- Attempt to mobilize the vascularized tendons of the rotator cuff. The goal is to repair the tendon to the greater tuberosity, or at least to the articular margin (the sulcus), without tension while the arm is resting at the patient’s side.
- Mobilization Limits: This may be impossible if massive defects of 5 cm or more involving the supraspinatus and infraspinatus tendons are present.
Surgical Warning: Suprascapular Nerve At-Risk
During deep mobilization of the retracted rotator cuff, the surgeon must be acutely aware of the suprascapular nerve. The nerve lies a mere 1.8 cm medial to the posterosuperior glenoid rim. Medial mobilization or aggressive traction exceeding this 1.8 cm threshold places the nerve at high risk for traction neurapraxia or transection. If further excursion is required, capsular stripping should be performed instead of blind medial traction.
5. Tuberoplasty and Impingement Clearance
If adequate mobilization for a tension-free repair is impossible, the surgeon must transition fully to a salvage débridement.
- Sufficiently débride the remaining cuff edges so that no residual components of the supraspinatus or infraspinatus tendons can be caught, ground, or impinged between the humeral head and the acromion during active or passive flexion and rotation.
- Tuberoplasty: The greater tuberosity often becomes prominent and irregular. These bony prominences must be excised (smoothed) to prevent mechanical impingement against the acromion during passive flexion of the upper extremity.
- Apply bone wax to the base of the excised exostosis. This achieves local hemostasis and acts as a physical barrier to prevent the regrowth of the bony exostosis.
6. Closure
- Copiously irrigate the subacromial space to remove all bone debris, which could lead to heterotopic ossification.
- Meticulous repair of the deltoid origin is paramount. Use heavy, nonabsorbable sutures (e.g., #2 FiberWire or Ethibond) passed through transosseous bone tunnels in the acromion.
- Close the subcutaneous tissue and skin in a standard layered fashion.
COMPLICATIONS AND MANAGEMENT
Complications following rotator cuff surgery occur across tears of all sizes, but the incidence and severity rise exponentially with large and massive tears. The tissue is often retracted, friable, and of poor biological quality, making any attempted repair highly tenuous.
1. Fixation Failure
When partial repairs are attempted during the débridement process, fixation failure is a primary concern.
* Nonabsorbable suture material must be used for both deltoid and rotator cuff tendon repair.
* While modern suture anchors possess excellent pull-out strength and endurance, relying on anchors alone in osteoporotic bone (common in this demographic) can lead to failure.
* Recommendation: Combine modern suture anchors with traditional sutures pulled through transosseous bone tunnels to maximize the biomechanical footprint and distribute load.
2. Anterosuperior Escape
An unsolved and devastating complication of rotator cuff surgery involves coracoacromial arch deficiency. If the CA ligament is aggressively resected in the presence of an anterosuperior cuff tear, the humeral head loses its secondary superior restraint. This results in anterosuperior subluxation (escape) of the humeral head during attempted deltoid contraction.
* Treatment: There is no highly effective soft-tissue treatment for this once it occurs; salvage typically requires a Reverse Total Shoulder Arthroplasty.
* Prevention: Preservation and meticulous reattachment of the coracoacromial arch during the index procedure is the absolute best method to prevent this complication.
3. Iatrogenic Nerve Injury
As previously noted, the suprascapular nerve is highly vulnerable during aggressive medial mobilization of the supraspinatus and infraspinatus. Adherence to the 1.8 cm safe zone from the glenoid rim is mandatory.
4. Complications of Tendon Transposition
Historically, local tendon transfers were attempted to close massive defects during débridement procedures. These carry significant morbidity:
* Subscapularis Transposition: Transposing the upper portion of the subscapularis superiorly can result in devastating anterior instability and profound weakness in internal rotation.
* Infraspinatus/Teres Minor Transposition: Superior transposition of the posterior cuff can result in severe external rotation weakness, limiting the patient's ability to perform activities of daily living (e.g., reaching the mouth or back of the head).
* Free Grafts: The use of autograft or allograft free tissues to bridge massive gaps has historically yielded very little success, often failing due to lack of vascularity and integration. They are generally not recommended in standard practice.
5. Postoperative Stiffness and Persistent Pain
Despite an excellent technical execution, a subset of patients will not return to their previous activity levels.
* Postoperative stiffness can develop from prolonged immobilization. Early, controlled passive range of motion is critical.
* Persistent night pain remains a complaint in approximately 20% of patients.
* While careful preoperative patient selection can drastically decrease the frequency of these subjective failures, surgeons must counsel patients that only about 80% will achieve complete pain relief and return to near-normal function.
POSTOPERATIVE REHABILITATION PROTOCOL
Rehabilitation following a decompression and débridement (without structural repair) differs significantly from a standard rotator cuff repair protocol. Because there is no healing tendon-to-bone interface to protect, rehabilitation can be accelerated to prevent stiffness, provided the deltoid repair is secure.
- Phase I (Weeks 0-3): The patient is placed in a standard sling for comfort. Immediate passive range of motion (PROM) is initiated to prevent adhesive capsulitis. Pendulum exercises are encouraged. Active deltoid contraction is strictly avoided to protect the deltoid reattachment.
- Phase II (Weeks 3-6): Transition from PROM to active-assisted range of motion (AAROM). The sling is discontinued. Gentle isometric exercises for the intact portions of the rotator cuff (subscapularis, teres minor) are initiated to optimize the remaining transverse force couple.
- Phase III (Weeks 6-12): Active range of motion (AROM) is permitted. Progressive strengthening of the deltoid and periscapular stabilizers (rhomboids, trapezius, serratus anterior) begins. The goal is to train the deltoid and periscapular muscles to compensate for the deficient superior rotator cuff.
CONCLUSION
Decompression and débridement of massive rotator cuff tears remains a highly effective, time-tested procedure for a specific cohort of patients. By thoroughly understanding the altered biomechanics of the cuff-deficient shoulder, meticulously preserving the coracoacromial arch, and performing a thorough tuberoplasty and débridement, the orthopedic surgeon can reliably eliminate impingement. While it does not restore normal anatomy, this procedure provides profound pain relief and functional improvement, serving as a vital technique in the comprehensive management of complex shoulder pathology.
You Might Also Like