Mastering Arthrodesis of the Thumb Interphalangeal and Metacarpophalangeal Joints
Key Takeaway
Arthrodesis of the thumb interphalangeal (IP) and metacarpophalangeal (MCP) joints is a highly reliable salvage procedure for advanced arthritis, instability, or severe deformity. Achieving a stable, painless pinch requires meticulous joint preparation, precise positioning—typically 15 to 20 degrees of flexion with appropriate pronation—and rigid internal fixation. This guide details the dorsal surgical approaches, joint preparation techniques including cup-and-cone and tongue-in-groove methods, and comprehensive postoperative rehabilitation protocols to ensure optimal functional outcomes.
INTRODUCTION AND BIOMECHANICAL PRINCIPLES
The thumb is the cornerstone of hand function, contributing to approximately 40% to 50% of overall hand capability. Its unique spatial orientation allows for opposition, key pinch, and power grasp. When the interphalangeal (IP) or metacarpophalangeal (MCP) joints of the thumb are compromised by advanced osteoarthritis, rheumatoid arthritis, post-traumatic arthrosis, or paralytic instability, arthrodesis remains the gold standard salvage procedure.
Unlike the carpometacarpal (CMC) joint, where mobility is paramount for opposition, the IP and MCP joints primarily provide stability during pinch and grasp. Consequently, arthrodesis of these distal joints is exceptionally well-tolerated by patients, provided the CMC joint remains mobile and the fusion is performed in an optimal biomechanical position. The primary goals of thumb arthrodesis are the eradication of pain, the restoration of a stable post for pinch, and the correction of deformity.
Clinical Pearl: The success of a thumb arthrodesis relies heavily on the compensatory mobility of the adjacent joints. Before fusing the MCP or IP joint, meticulously evaluate the basal (CMC) joint. Fusing the MCP joint in the presence of severe, untreated CMC arthritis will exacerbate basal joint pain due to increased lever-arm forces.
PREOPERATIVE EVALUATION AND PLANNING
Clinical Assessment
A thorough clinical examination must assess the integrity of the skin, the neurovascular status, and the functional demands of the patient. Evaluate the degree of deformity, noting any hyperextension (often seen in rheumatoid swan-neck or boutonnière deformities) or lateral instability (collateral ligament incompetence).
Radiographic Evaluation
Standard posteroanterior (PA), lateral, and oblique radiographs of the thumb are mandatory.
* Assess the degree of joint space narrowing, osteophyte formation, and subchondral sclerosis.
* Evaluate bone stock, particularly in rheumatoid patients who may present with arthritis mutilans (severe osteolysis and telescoping of the digits).
* Templating should be performed to determine the size of internal fixation devices, such as cannulated headless compression screws or Kirschner wires (K-wires).
INTERPHALANGEAL (IP) ARTHRODESIS OF THE THUMB
Arthrodesis of the thumb IP joint is most commonly indicated for post-traumatic arthritis, chronic instability, or severe flexion contractures. The goal is to provide a stable, painless tip for fine pinch.
Surgical Anatomy and Approach
The IP joint is approached dorsally. Care must be taken to protect the terminal branches of the radial sensory nerve and the dorsal venous network.
- Incision: Make a dorsal longitudinal, transverse, or H-shaped incision over the IP joint. A longitudinal incision is generally preferred as it allows for extensile exposure and minimizes the risk of skin necrosis.
- Tendon Management: Identify and divide the extensor pollicis longus (EPL) tendon longitudinally or transversely to open the joint capsule.
- Exposure: Flex the IP joint acutely to expose the articular surfaces of the proximal and distal phalanges.
Joint Preparation
Meticulous preparation of the arthrodesis site is critical for achieving a high union rate.
- Ligament Release: Release the collateral ligaments to allow complete visualization and mobilization of the joint surfaces.
- Cartilage Resection: Using a microsaw or sharp osteotome, remove the articular cartilage and a small amount of subchondral bone from both the distal and proximal phalanges. The cuts must be parallel to ensure maximum cancellous bone contact.
- Alternative Preparation: A cup-and-cone reamer system can be utilized to preserve bone length and allow for micro-adjustments in positioning before definitive fixation.
Surgical Pitfall: Avoid excessive bone resection. Over-shortening the distal phalanx compromises the nail bed and the aesthetic appearance of the thumb, while also reducing the lever arm for pinch.
Positioning and Fixation
The optimal position for IP joint arthrodesis is 15 to 20 degrees of flexion with neutral rotation. This slight flexion accommodates pulp-to-pulp pinch with the index and middle fingers.
- Provisional Fixation: Once the joint is appropriately positioned, drive a small K-wire distally through the distal phalanx, exiting the tip of the thumb. Reduce the joint, and drive the wire proximally into the proximal phalanx.
- Definitive Fixation Options:
- Kirschner Wires: Two crossed K-wires or a single longitudinal wire supplemented by an oblique wire provide adequate stability.
- Headless Compression Screws: If bone size and stock allow, cannulated headless compression screws are the modern implant of choice. They provide dynamic interfragmentary compression, allow for early mobilization, and eliminate the need for hardware removal.
- Management of Bone Loss: In patients with arthritis mutilans or severe traumatic bone loss, the thumb may be excessively shortened. To restore length and optimize biomechanics, harvest a small corticocancellous bone graft from the iliac crest. Interpose the graft between the phalanges and transfix the construct with K-wires.
METACARPOPHALANGEAL (MCP) ARTHRODESIS OF THE THUMB
The MCP joint of the thumb is a condyloid joint with a highly variable arc of motion. Arthrodesis is indicated for chronic ulnar collateral ligament (UCL) or radial collateral ligament (RCL) instability, rheumatoid arthritis (often presenting with a severe flexion or extension deformity), and primary osteoarthritis.
Surgical Anatomy and Approach
- Incision: Make a dorsal longitudinal incision centered over the MCP joint.
- Soft Tissue Dissection: Carefully dissect through the subcutaneous tissues, identifying and retracting the dorsal sensory branches of the radial nerve.
- Tendon Retraction: Incise the extensor hood. Displace the extensor pollicis longus (EPL) tendon to the ulnar side and the extensor pollicis brevis (EPB) to the radial side to expose the dorsal capsule.
Joint Preparation Techniques
Several techniques exist for preparing the MCP joint surfaces. The choice depends on the surgeon's preference, the presence of deformity, and the quality of the bone stock.
Technique 1: Flat Osteotomy Cuts
- With an oscillating saw or sharp osteotome, cut across the articular surface of the proximal phalanx in a straight line at exactly 90 degrees to its long axis.
- To achieve the desired 15 degrees of flexion at the MCP joint, the metacarpal cut must be angled. Do not osteotomize the distal metacarpal at 90 degrees; instead, angle the cut to remove more bone toward the palmar aspect.
- When the two raw surfaces are brought together, they should fit flush, naturally resting the phalanx at a 15-degree flexion angle relative to the metacarpal.
Technique 2: Cup-and-Cone Configuration
- The articular surfaces can be prepared using specialized cup-and-cone reamers.
- This technique is highly advantageous as it preserves bone length, maximizes cancellous bone contact area, and allows the surgeon to dial in the exact degree of flexion, abduction, and pronation before deploying fixation.
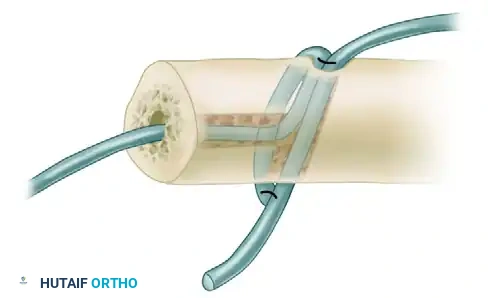
Technique 3: Tongue-in-Groove (For Subluxation or Shortening)
When the joint is severely subluxated or when bone shortening is required to reduce a chronic dislocation without placing undue tension on the neurovascular bundles, the tongue-in-groove technique is highly effective.
* On the proximal end of the proximal phalanx, use a rongeur or burr to shape a protruding "tongue" of bone.
* On the distal end of the first metacarpal, create a corresponding V-shaped notch or "groove."
* Impact the tongue into the groove. This inherently stable configuration places large surfaces of cancellous bone in direct contact while allowing the angle of fusion to be easily adjusted.
* Pack any remaining small fragments of local autograft bone into the spaces around the joint margins to augment the fusion mass.
Surgical Warning: Regardless of the preparation technique, meticulously remove any protruding small edges or osteophytes to smooth the arthrodesis site. Prominent dorsal bone edges will cause severe irritation to the overlying EPL tendon, potentially leading to tenosynovitis or delayed rupture.
Optimal Positioning
Positioning the MCP joint correctly is the most critical step of the procedure. A malpositioned fusion will severely impair hand function.
- Flexion: The joint should be fused in 15 degrees of flexion.
- Pronation: Ensure the thumb is in appropriate pronation so that the pulp of the thumb can seamlessly oppose the pulp of the index and middle digits.
- Abduction: If the first metacarpal is chronically adducted (a common compensatory posture in advanced CMC arthritis or rheumatoid disease), some of this adduction contracture can be overcome by fusing the MCP joint in slight abduction. This places the thumb in a functional position without the need for extensive soft-tissue releases in the palm.
Fixation Strategy
While plates and screws or tension band constructs can be used, longitudinal Kirschner wire fixation remains a classic, reliable, and low-profile method.
- Wire Insertion: Fix the arthrodesis with three K-wires inserted longitudinally.
- Trajectory: Insert the wires first through the dorsal aspect of the metacarpal, advancing them distally across the arthrodesis site and into the proximal phalanx.
- Safety Checks: Fluoroscopically ensure that the wires do not pierce the flexor pollicis longus (FPL) tendon volarly or penetrate the distal IP joint.
- Hardware Management: Cut the wires off under the skin to prevent pin-tract infections and allow for cast immobilization.
- Closure: Approximate the extensor tendons and capsule with a small absorbable suture (e.g., 3-0 Vicryl). Close the skin meticulously.
POSTOPERATIVE CARE AND REHABILITATION
A strict and well-monitored postoperative protocol is essential to prevent nonunion and hardware failure. The timeline is generally consistent for both IP and MCP joint arthrodesis.
Phase 1: Immediate Postoperative (0 to 14 Days)
- Immediately following wound closure, place the hand in a bulky, well-padded volar plaster splint that includes the thumb but leaves the other digits free for immediate active range of motion.
- Elevate the extremity strictly to minimize edema.
- At 10 to 14 days, the patient returns to the clinic. The initial splint and skin sutures are removed.
Phase 2: Cast Immobilization (2 to 6 Weeks)
- Following suture removal, the thumb is protected in a rigid, short-arm thumb spica cast.
- The cast should immobilize the fused joint while allowing full motion of the uninvolved fingers to prevent stiffness.
- This cast is maintained for an additional 4 weeks (totaling approximately 6 weeks post-surgery).
Phase 3: Hardware Removal and Transition (6 to 10 Weeks)
- At the 6-week mark, clinical and radiographic evaluations are performed.
- If K-wires were used and left prominent or just beneath the skin, they are typically removed in the clinic at this stage. (Note: Headless compression screws or buried plates are left in situ unless symptomatic).
- Following wire removal, the patient is transitioned to a custom-molded thermoplastic thumb spica splint. This splint is worn continuously for another 3 to 4 weeks, removed only for hygiene.
Phase 4: Functional Restoration (10 Weeks and Beyond)
- Active use of the thumb is resumed gradually.
- Patients are instructed to begin with light activities of daily living (ADLs) and progressive pinch-strengthening exercises.
- It is crucial to educate the patient that functional, active use can safely commence at this stage, despite the potential absence of complete radiographic evidence of fusion. Radiographic consolidation often lags behind clinical union by several weeks to months.
COMPLICATIONS AND MANAGEMENT
While thumb arthrodesis is generally highly successful, surgeons must be prepared to manage potential complications.
- Nonunion: The nonunion rate for thumb MCP and IP arthrodesis ranges from 5% to 10%. Risk factors include smoking, inadequate bone preparation, and non-compliance with immobilization. Asymptomatic nonunions (fibrous unions) often require no treatment if the joint is stable and painless. Symptomatic nonunions require revision arthrodesis with structural bone grafting and rigid plate fixation.
- Malunion: Fusing the joint in excessive extension or supination prevents effective pinch. Revision osteotomy is required if the functional deficit is severe.
- Hardware Prominence: Subcutaneous K-wires or bulky dorsal plates can cause skin irritation or tendon attrition. Symptomatic hardware should be removed only after solid radiographic union is confirmed.
- Infection: Superficial pin-tract infections are managed with oral antibiotics and early pin removal if union is sufficient. Deep infections require formal surgical debridement and hardware removal.
CONCLUSION
Arthrodesis of the thumb interphalangeal and metacarpophalangeal joints remains a cornerstone technique in reconstructive hand surgery. By adhering to strict biomechanical principles—specifically achieving 15 to 20 degrees of flexion, ensuring appropriate pronation, and utilizing meticulous joint preparation techniques like the cup-and-cone or tongue-in-groove methods—surgeons can reliably restore a powerful, painless pinch. Rigorous adherence to postoperative immobilization protocols ensures high union rates and excellent long-term functional outcomes for patients suffering from debilitating thumb pathology.
You Might Also Like